Article Text

Abstract
Background: Rheumatoid arthritis (RA) is associated with higher cardiovascular disease (CVD) risk due to the underlying inflammation (1). It is uncertain if the excess CV risk could be reduced by effective suppression of inflammation using the treat-to-target (T2T) approach in patients with early RA (ERA).
Objectives: This study compared the 5-year cardiovascular event (CVE) rate among ERA patients managed by a T2T strategy with a CV risk factor-matched non-RA population.
Methods: This was an observational study using the Hong Kong Hospital Authority population-based hospital database known as the Clinical Data Analysis and Reporting System (CDARS) and the Clinical Rheumatology Systematic Treat-to-target in Asia Leadership (CRYSTAL) registry. ERA subjects from the registry with baseline disease duration less than 2 years were recruited between 2012-2016. All patients received a tight control, T2T treatment strategy aiming at remission and had been followed for at least 5 years. Each ERA subject was matched to 3 non-RA controls according to age, gender, smoking status, and the presence of diabetes mellitus (DM), hypertension (HT) and hyperlipidaemia (HL). All subjects on antiplatelet agents, with pre-existing CVD or chronic kidney disease were excluded. All subjects were analysed up to 5 years from baseline. The primary end point was the first occurence of a CVE, namely ischaemic cerebrovascular disease, ischaemic heart disease and heart failure.
Results: The study identified 261 ERA subjects and 783 matched controls. Their characteristics were shown on Table 1. The mean age was 60+/-12 years, 78% were female, 18% were smokers, 8%, 25% and 22% had DM, HT and HL respectively.
Characteristics of ERA subjects and the matched controls
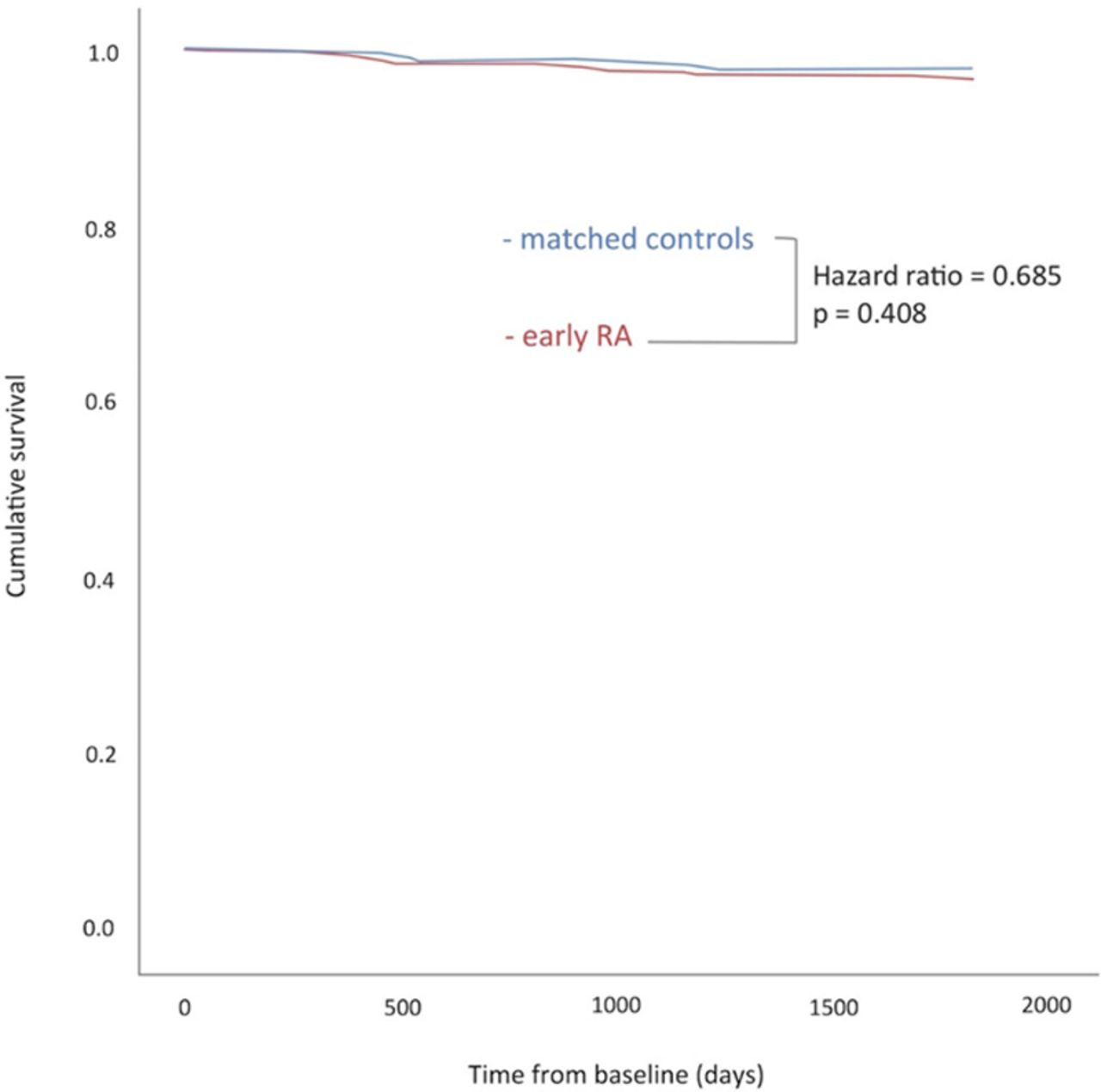
CVEs occurred in 2.3% ERA subjects and in 3.3% controls. The difference was statistically insignificant. The CVE-free survival was shown in Figure 1.
{kind=link}
CVE-free survival curves of ERA subjects & matched controls
In the ERA cohort, after adjusting for baseline age and atherogenic index, cox-regression analysis showed that i) a longer DAS28 remission duration was protective for CVE with an adjusted hazard ratio (AHR) of 0.46 (95% CI 0.23-0.93), while ii) poor baseline function as reflected by a higher health assessment questionnaire (HAQ) score was predictive of CVE with an AHR of 5.2 (95% CI 1.2-23).
Conclusion: ERA patients treated by a T2T strategy did not develop excess CVE compared to CV risk factor-matched controls over 5 years. A longer disease remission duration was protective while a higher baseline HAQ was associated with a higher CVE risk.
References: [1]Agca R et al. EULAR recommendations for cardiovascular disease risk management in patients with rheumatoid arthritis and other forms of inflammatory joint disorders: 2015/2016 update. Annals of the Rheumatic Diseases.
Disclosure of Interests: None declared