Article Text

Abstract
Background: Sleep disturbances are common in individuals with rheumatological diseases in general and systemic lupus erythematosus (SLE) in particular1. Studies suggest that obstructive sleep apnea (OSA) might correlate with SLE disease activity and the presence of additional symptoms such as pain, fatigue, affective symptoms and steroid use2. Sleep disturbances symptomatology such as fatigue and increased pain overlap with constitutional inflammatory symptoms of SLE and may mimic or mask disease related relapse3,4. Therein lies the importance of diagnosing and treating such disorders in SLE.
Objectives: To determine whether patients with SLE have increased prevalence of OSA as assessed by the apnea hypopnea index (AHI) and to explore possible contributors to OSA including SLE disease activity and accrued damage, medications, secondary fibromyalgia and depression.
Methods: 42 consecutive patients with SLE (38 women, 4 men) and 20 healthy, sex, body mass index (BMI) and age matched controls (15 women, 5 men) were consecutively recruited and underwent an ambulatory sleep study using the WatchPAT device. All participants completed questionnaires including Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), Functional Assessment of Chronic Illness Therapy (FACIT), Widespread Pain Index (WPI), Symptoms Severity Scale (SSS) and Beck Depression Inventory. SLE disease activity and damage were assessed using the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) and Systemic Lupus International Collaborating Clinics (SLICC) damage index.
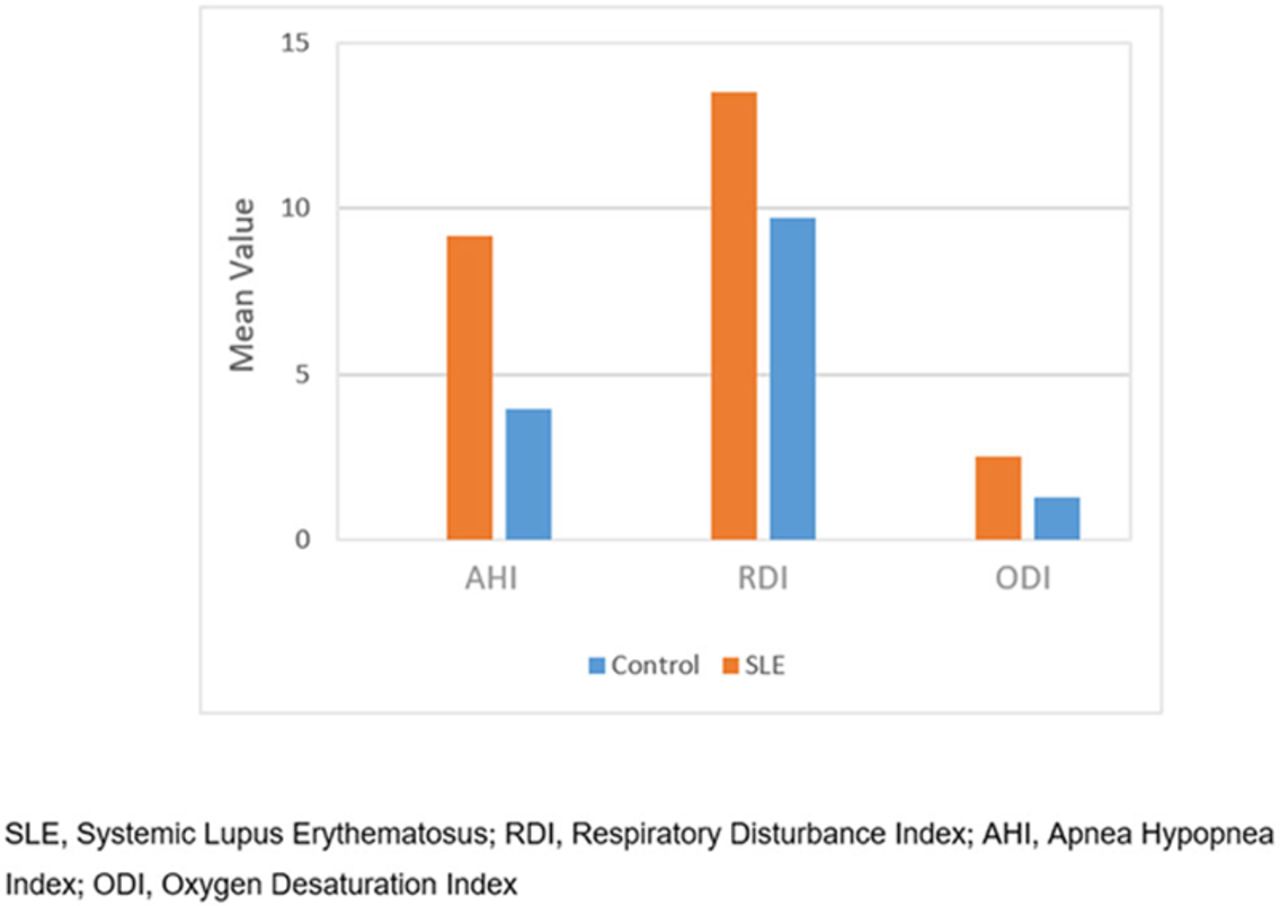
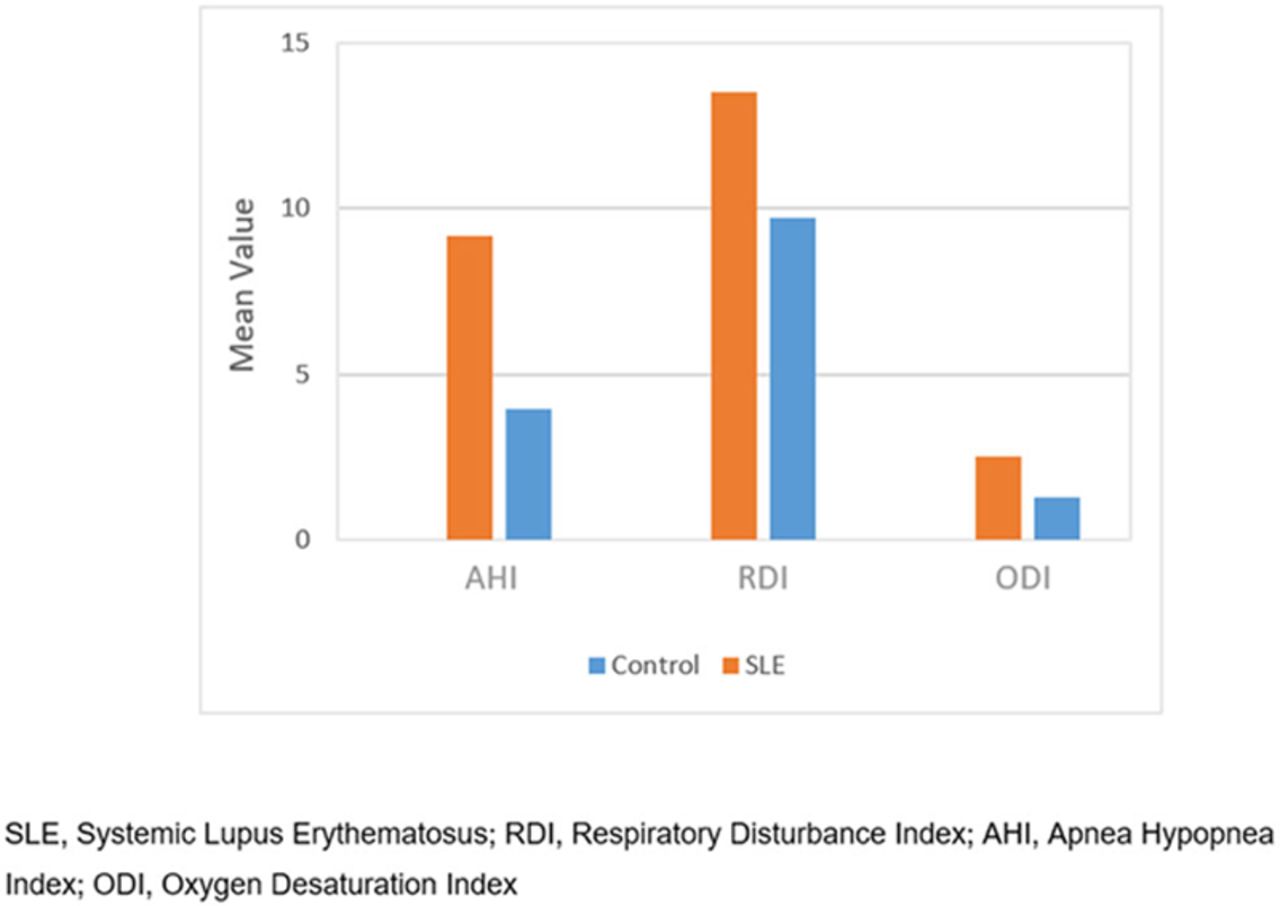
Results: The mean AHI was 9.19 ± 6.79 in the SLE group and 3.95 ± 3.47 in the control group (p=0.004). Moderate-severe OSA (AHI≥15) was significantly more common in patients with SLE (23.6% vs. 0%, p=0.04). Patients with SLE had lower sleep efficiency (83.38 ± 6.15 vs. 87.22 ± 4.24, p=0.03), increased sleep arousals (7.72 ± 5.66 vs. 5.13 ± 2.29, p=0.01), higher PSQI and FACIT scores SLE (8.14 ± 3.47 vs. 5.10 ± 2.64, p=0.001, 16.89 ± 11.19 vs. 7.29 ± 5.93, p= 0.0008 respectively) and had more fibromyalgia as assessed by WPI and SSS (19.5% vs. 0%, p=0.04). BMI and the SLICC score were independent predictors of OSA (p=0.03 and p=0.02 respectively). A correlation between SLEDAI and moderate-severe OSA was found (p=0.03), although an association to medications, secondary fibromyalgia and depression was not found.
Conclusion: Patients with SLE have increased prevalence of OSA with lower sleep quality compared to healthy controls. Our findings suggest a possible correlation between accrued damage as assessed by the SLE damage index and OSA.
References: [1]Wu, L., Shi, P. L., Tao, S. S., Tao, J. H. & Wu, G. C. Decreased sleep quality in patients with systemic lupus erythematosus: a meta-analysis. Clin. Rheumatol. (2020) doi:10.1007/s10067-020-05300-3.
[2]Palagini, L. et al. Sleep disorders and systemic lupus erythematosus. Lupus vol. 23 115–123 (2014).
[3]Javaheri, S. & Javaheri, S. Update on Persistent Excessive Daytime Sleepiness in OSA. Chest vol. 158 776–786 (2020).
[4]Mertz, P. et al. Towards a practical management of fatigue in systemic lupus erythematosus. Lupus Science and Medicine vol. 7 (2020).
{kind=link}
WatchPAT sleep parameters analysis
Disclosure of Interests: None declared