Article Text

Statistics from Altmetric.com
We note with interest and express our principle agreement with the views put forward by Professor Rosenzwajg M1 in the recent Editorial ‘Immunological and clinical effects of low-dose interleukin-2 across 11 autoimmune diseases in a single, open clinical trial’ published in Annals of the Rheumatic Diseases. The authors conclude that any autoimmune or inflammatory disease denotes a regulatory T cells (Tregs) insufficiency, which is restored by low-dose interleukin (IL)−2 ((1 million IU/day) for 5 days, followed by fortnightly injections for 6 months) selectively and safely activate and expand Tregs in 11 autoimmune diseases. This study is important and deserves a practical value. In our study, the absolute changes of peripheral lymphocyte subpopulations and CD4+ T subsets, especially Tregs, and the safety and efficacy of low-dose IL-2 in dermatomyositis (DM)/polymyositis (PM), which are idiopathic inflammatory myopathies and not shown in the above article, are shared with the readers.
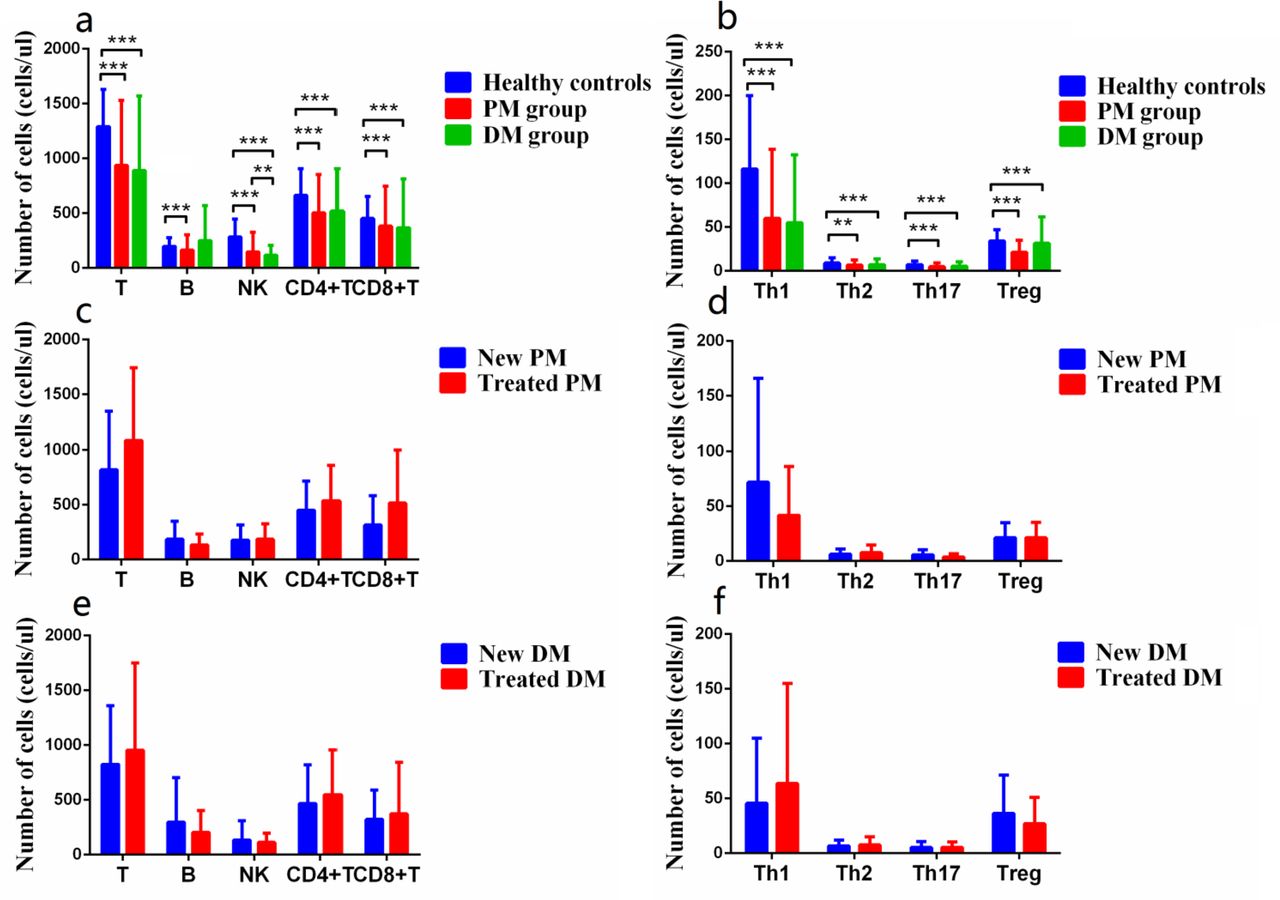
In our study, total 147 patients with PM/DM were enrolled and 128 gender-matched and age-matched healthy adults were participated as controls from February 2016 to October 2018. The absolute numbers of T, B, natural killer (NK), CD4+ T, CD8+ T, Th1, Th2, Th17 and Tregs in peripheral blood of these individuals were detected by flow cytometry combined with standard absolute counting beads.2 Patients with DM/PM, regardless of new onset (no prior treatment) or treatment with immunosuppressants, had significantly lower absolute numbers of Tregs as well as T, B, NK, CD4+ T, CD8+ T, Th1, Th2 and Th17 than healthy controls (figure 1a,b), which were significantly correlated with disease activity. There were no any significant differences in the numbers of above subsets between new PM/DM and treated PM/DM (figure 1c–f), indicating that those decreases in the subsets are associated directly with the pathogenesis of PM and/or DM rather than high-dose glucocorticoids or immunosuppressive agents.3 Reduced Tregs should fail to prevent autoimmunity and control inflammation, contributing to the pathogenesis of DM/PM patients. Furthermore, these reductions could be aggravated by conventional therapies, especially immunosuppressive agents, to increase patients’ risk of malignancies and infection.3–5
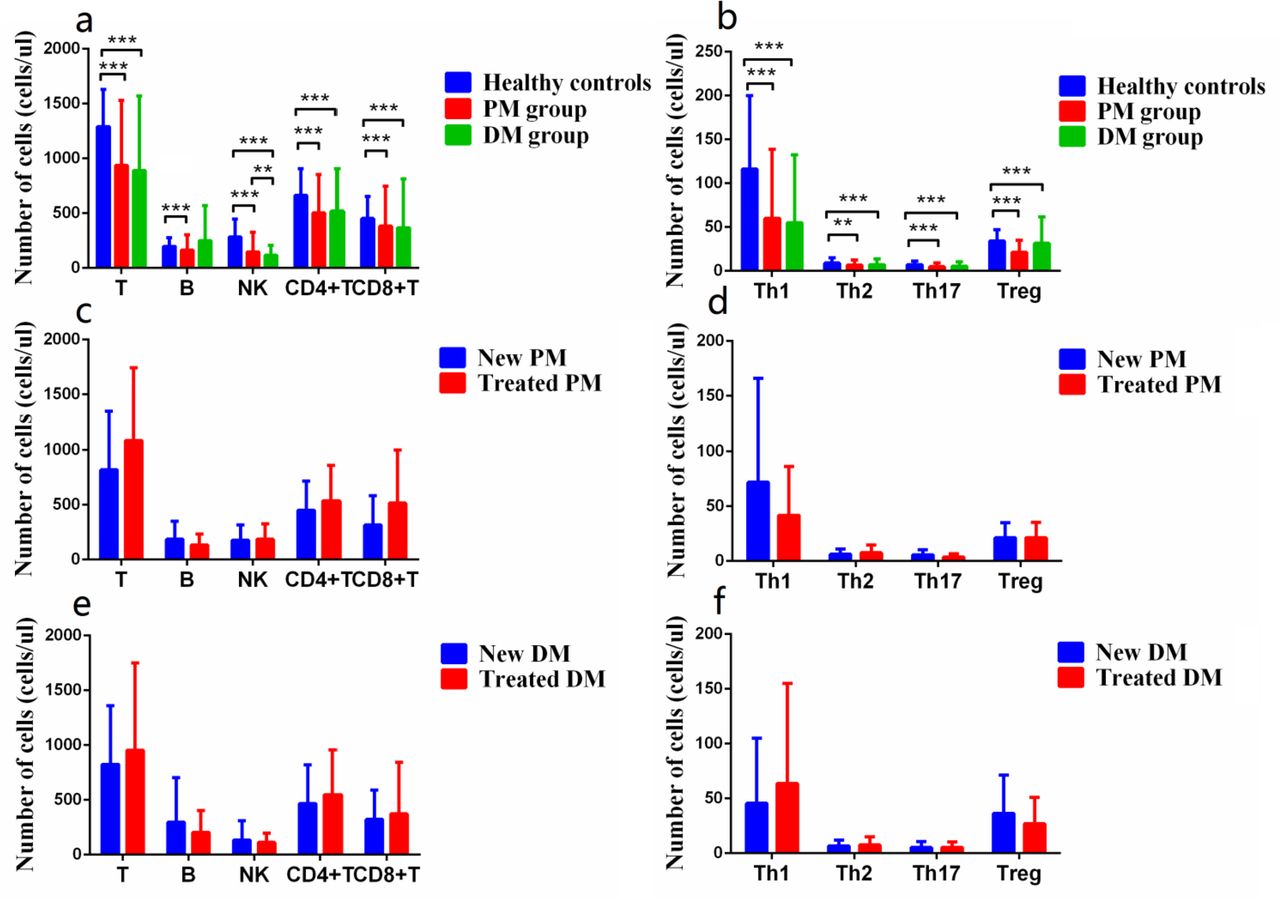
Absolute numbers of peripheral lymphocyte subsets between healthy controls and patients were assessed by flow cytometry using one-platform method. (a) PM (n=39)/DM (n=108) patients had lower levels of T, B, NK, CD4+ T and CD8+ T in PB compared with those of healthy controls (n=128). (b) The levels of Th1, Th2, Th17 and Tregs in PB were significantly decreased in patients with PM/DM. (c–f) There were no significant changes of the absolute numbers of T, B, CD4+ T, CD8+ T, NK, Th1, Th2, Th17 and Tregs in PB between new patients (PM, n=22 or DM, n=53) and treated patients (PM, n=17 or DM, n=55). Data were presented as mean±SD and statistical analysis was determined by two-tailed unpaired t-test. *p<0.05, **p<0.01, ***p<0.001. DM,dermatomyositis; PB, peripheral blood; PM, polymyositis; Tregs, regulatory Tcells.
Total 116 patients in non-IL-2 group were given only conventional treatments while 31 patients in IL-2 group were not only given conventional treatments but also injected subcutaneously human IL-2 (aldesleukin) at 0.50 Million IU/day for a 5-day course. After IL-2 administration, the absolute numbers of Tregs increased dramatically about fourfolds (figure 2b). Besides, other cells, such as T, B, CD4+ T, CD8+ T, Th1, Th2 and Th17, were also increased mildly to modestly as compared with those before treatment (figure 2a,b). The treatment of short-term and low-dose IL-2 led to a better remission, indicated by a decrease in disease indicators (VAS, ESR, CK, CK-MB, LDH and HBDH) compared with conventional therapy only (figure 2c–h).

{kind=link}
{kind=link}
Efficacy of short-term and low-dose IL-2 treatment in regulating levels of peripheral lymphocyte subsets and reducing disease activity. (a) Absolute numbers of lymphocytes, including T, B, CD4+ T and CD8+ T cells in patients were significantly increased after treatment. (b) Absolute numbers of CD4+ T subsets, especially Tregs, were significantly increased in patients after treatment. (c–h) VAS, ESR, CK, CK-MB, LDH and HBDH in all patients were significantly lower than those before treatment. After treatment, VAS in IL-2 group decreased more obviously, while the other indexes of IL-2 group had a trend towards lower values without statistical significance compared with non-IL-2 group. Two-tailed unpaired t-test was used to compare the disease activity measures between IL-2 (red) and control groups (blue). *p<0.05, **p<0.01, ***p<0.001. CK,creatine kinase; CK-MB, creatine kinase MB; ESR, erythrocyte sedimentation rate;HBDH, hydroxybutyric dehydrogenase; IL, interleukin; LDH, lactate dehydrogenase;Tregs, regulatory T cells; VAS, visual analogue scale/score.
Notably, low-dose IL-2 treatment reduced muscle tissue inflammation through specific Treg expansion and activation to balance Teff cells. In addition, other study showed that the treatment can reduce the secretion of chemokines by fibroblasts and thus reduce the migration of peripheral lymphocytes that can further cause muscle damage and creating a loop,6 which may be one of the reasons for the increase in peripheral lymphocyte subsets and efficacy of IL-2 in DM/PM patients.
In conclusion, our study showed first that there was a decrease in absolute numbers of peripheral Tregs in PM/DM patients with or without immunosuppression treatment. Low-dose IL-2, synergising with conventional therapy, can markedly increase the number of Tregs, as well as other lymphocytes to some degree, and maintain the immunologic balance, which may help for DM/PM patients’ symptom remission without over-treatment and evaluated side effect and enhance the ability to resist infection. Our study on DM/PM that was not stated in the study of Rosenzwajg M reconfirmed the involvement of Treg dysfunction in the pathogenesis of autoimmune diseases, which can be restored by low-doses IL-2.
Ethics statements
Ethics approval
This study was approved by The Second Hospital of Shanxi Medical University Ethics Committee (2016 KY-007).
Footnotes
S-XZ and JW are joint first authors.
Contributors Study design and manuscript writing: S-XZ and JW. Data extraction, quality assessment, analysis and interpretation of data: S-XZ, JW and H-HS. All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published. XL had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.