Article Text

Abstract
Objectives The impact of inflammatory arthritis (IA) on male fertility remains unexplored. Our objective was to evaluate the impact of IA on several male fertility outcomes; fertility rate (number of biological children per man), family planning, childlessness and fertility problems.
Methods We performed a multicentre cross-sectional study (iFAME-Fertility). Men with IA 40 years or older who indicated that their family size was complete were invited to participate. Participants completed a questionnaire that included demographic, medical and fertility-related questions. To analyse the impact of IA on fertility rate, patients were divided into groups according to the age at the time of their diagnosis: ≤30 years (before the peak of reproductive age), between 31 and 40 years (during the peak) and ≥41 years (after the peak).
Results In total 628 participants diagnosed with IA were included. Men diagnosed ≤30 years had a lower mean number of children (1.32 (SD 1.14)) than men diagnosed between 31 and 40 years (1.60 (SD 1.35)) and men diagnosed ≥41 years (1.88 (SD 1.14)).This was statistically significant (p=0.0004).The percentages of men diagnosed ≤30 and 31–40 years who were involuntary childless (12.03% vs 10.34% vs 3.98%, p=0.001) and who reported having received medical evaluations for fertility problems (20.61%, 20.69% and 11.36%, p=0.027) were statistically significant higher than men diagnosed ≥41 years.
Conclusions This is the first study that shows that IA can impair male fertility. Men diagnosed with IA before and during the peak of reproductive age had a lower fertility rate, higher childlessness rate and more fertility problems. Increased awareness and more research into the causes behind this association are urgently needed.
- arthritis
- rheumatoid
- spondylitis
- ankylosing
- epidemiology
- inflammation
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Inflammatory arthritis (IA) is associated with male infertility, erectile dysfunction and hypogonadism.
What does this study add?
The diagnosis of IA before or during the peak of the male reproductive age was associated with a lower fertility rate, higher rates of involuntary childlessness and fertility problems.
How might this impact on clinical practice or future developments?
Rheumatologists should be aware that IA and/or the pharmacological treatment associated with IA may impair male fertility.
Multiple biological and non-biological mechanisms can be responsible for this association and more research is urgently needed.
Introduction
Spondyloarthritis (SpA) and rheumatoid arthritis (RA) are frequent causes of inflammatory arthritis (IA) that can affect men before or during the peak of their reproductive age.1–4 Even though IA is associated with male infertility, erectile dysfunction and hypogonadism5 6 the impact of IA on male fertility remains largely unexplored. This is even more striking if we consider that several frequently prescribed anti-rheumatic drugs have been associated with reversible or irreversible testicular toxicity.7
The majority of people aspire to have children and it is known that men desire parenthood as much as women do.8–10 Nonetheless, the impact of IA on one of the most important markers of fertility, the male fertility rate (total number of children per man),11–13 has never been studied before.
Childbearing decisions and reproductive potential are strongly influenced by multiple psychosocial, demographic and biological factors.9 14 Furthermore, it has been demonstrated that men diagnosed with chronic diseases are exposed to additional factors that have an effect on their childbearing decisions and their reproductive potential.15 16
In women diagnosed with IA, several factors related to IA have been associated with lower fertility rates.17–19 It can be expected that some of these factors could also influence the fertility rate of men diagnosed with IA, such as impaired sexual function, lower intercourse frequency, deciding not to have a family or to have smaller families due to concerns about the impact of IA or antirheumatic treatment.
Therefore, we aimed to evaluate the impact of IA on relevant markers of male fertility. Our primary objective was to compare the fertility rate of men diagnosed with IA based on their age at diagnosis. Additionally, we compared the fertility rate of men diagnosed with IA with the general male population of the Netherlands. To further evaluate the impact of IA on male fertility, as secondary objectives we compared the total number of pregnancies per man, desired family size (family planning), the proportion of childless men and fertility outcomes based on the results from medical evaluations for fertility problems.
Methods
Study design and patient selection
We conducted a multicentre cross-sectional study in eight Dutch hospitals (iFAME (Inflammunity and Fertility in Men)-Fertility study). In the Netherlands, most men become a father between the age of 30 and 40 years and this period is considered to be the peak of reproductive age.20 Therefore, men who were diagnosed with IA based on the expert opinion of their rheumatologists (RA, juvenile idiopathic arthritis (JIA) and SpA (ankylosing spondylitis (AS), psoriatic arthritis (PsA), reactive arthritis, enteropathic arthritis), who at the time of inclusion were 40 years or older and who indicated that their ‘family size’ was completed were included. Men who were still planning on having biological children in the future were excluded.
To evaluate the impact of IA on male fertility we considered the age at diagnosis of IA and divided participants into three study groups: diagnosis ≤30 years (before the peak of reproductive age), diagnosis between 31 and 40 years (during the peak of reproductive age) and diagnosis ≥41 years (after the peak reproductive age).
We estimated the mean number of children number per men without IA in their reproductive lifespan at 1.7 (SD: 1.0) and estimated a mean number of 1.4 children as significantly different. Using data simulation that accounted for dispersion and under-dispersion, to reject the null hypothesis with a 80% power (alpha=0.05; two sided), it was estimated that 548 men were needed to be included in the study (n=137, n=137 and n=274 per group, respectively).
Data collection
A self-reported questionnaire developed for this study was used. The design of this questionnaire was based on the ‘fertility experiences questionnaire (FEQ)’. The FEQ was validated in women with subfertility and when compared with medical records it was proven to be over 90% sensitive for fertility outcomes.21 In addition, we adapted the questionnaire to our population using previous questionnaires that have evaluated fertility outcomes in male kidney transplant recipients22 and in women with rheumatic diseases.23 24 Our questionnaire was divided into four sections: general demographic information, medical history, family planning and fertility outcomes (online supplemental 1). The digital version of the questionnaire that was distributed to participants was built using the survey software GemsTracker/LimeSurvey (LimeSurvey, Hamburg, Germany).
Supplemental material
Men who fulfilled the inclusion criteria of being 40 years or older and diagnosed with IA were invited to participate in the study. These men received a letter from their hospital that included information about the study. To ensure the protection of privacy data, the letter included a personalised link to complete the digital questionnaire. To increase the number of responders, a second letter was sent to all non-responders.
Our primary outcome, the male fertility rate, was calculated using the answers to the question ‘How many biological children did you have?’. This is a validated method that has been used to evaluate fertility. For secondary outcomes, other collected data include, but are not limited to, total number of pregnancies, desired family size, satisfaction with final family size and relevant medical history regarding fertility and pregnancy outcomes. A pregnancy was defined as ‘any positive pregnancy test (even if it did not result in a live born child)’ and time to pregnancy (TTP) was determined with the answers provided to the question ‘How many months did it take for your partner to get pregnant?’.
A Likert scale questionnaire (scale ranging from completely disagree (0) to completely agree (10)) was used to evaluate the impact of IA on family planning/desired number of children.
Statistical analysis
Comparisons between the three groups and between the groups and the general population were tested. Categorical variables were presented as number (percentage), and continuous variables are reported as mean±SD or median ±IQR, as appropriate. Continuous variables were compared using a one-way analysis of variance, Tukey post hoc test, paired t-test and Wilcoxon rank. Categorical variables were compared using χ2 tests and Fisher’s exact tests. To control for confounders, multivariate regression model (analysis of covariance) was used. All potential confounders were fitted into the model. The level of significance was set as a two-tailed p≤0.05, and statistical analyses were completed using Stata V.15 (StataCorp).
Patient and public involvement
Six male patients diagnosed with IA and who are active members of the research advisory board from the Department of Rheumatology of the Erasmus University Medical Center were involved in the design of the questionnaire and the invitation letter. We carefully assessed the burden on participating patients. We intend to share the results to participating patients and will appropriately disseminate the results.
Results
Between September 2019 and January 2021, a total of 1841 men were invited to participate in the study. All hospitals invited men from the three study groups using a 1:1:2 ratio until the necessary number of patients per group to achieve statistical power was reached. In total, 628 men agreed to participate (response rate of 34.1%). A detailed description of the demographics characteristics of these men is presented in table 1. Due to current privacy regulations that are applicable in the Netherlands, it was not possible to describe the demographic characteristics of the non-responders.
Demographic characteristics
Total number of biological children (fertility rate)
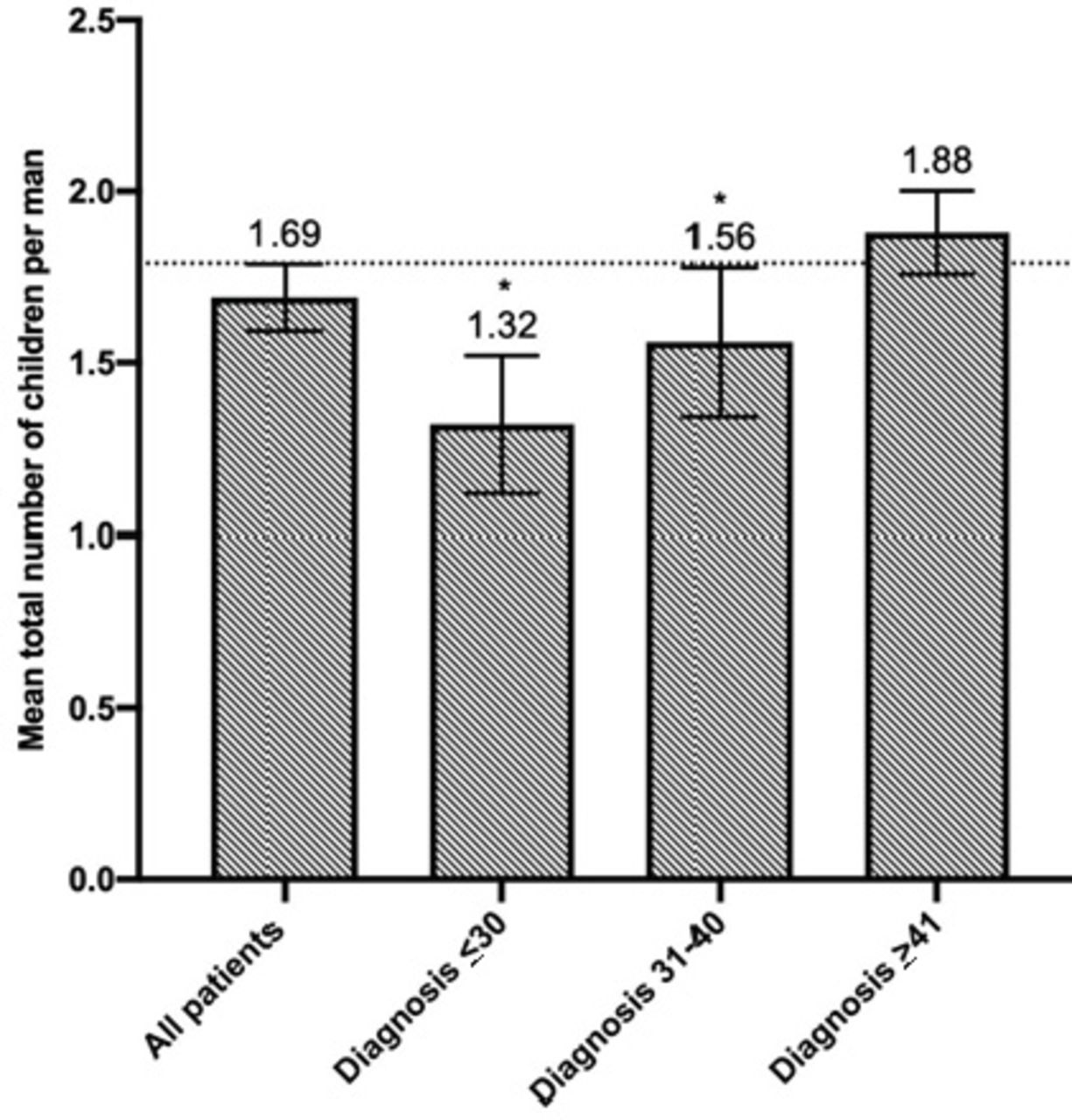
Men diagnosed ≤30 years had a lower number of children (1.32 (SD 1.14)) than men diagnosed between 31 and 40 years (1.56 (SD 1.27)) and men diagnosed ≥41 years (1.88 (SD 1.14)) (see figure 1). There was a statistically significant difference between groups (p=0.0004). The total number of children was statistically significant lower in men diagnosed <30 years and in men diagnosed 31–40 years compared with men diagnosed >41 years (p<0.001 and p=0.020, respectively). The difference between men diagnosed <30 and 31–40 years was not statistically significant (p=0.264).
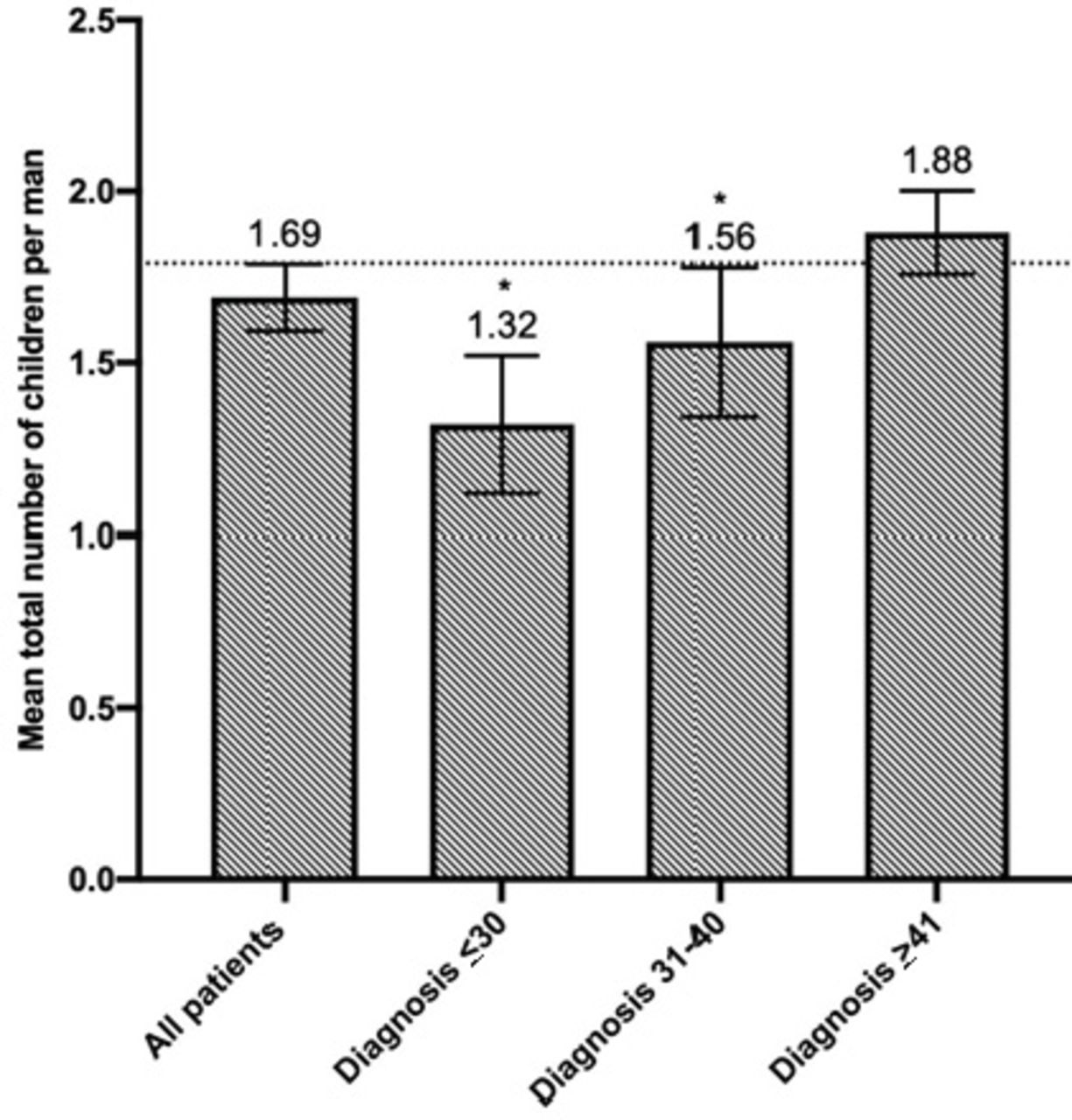
Mean total number of children per man for all participants and per group. Error bars represent 95% CI. The dotted line represents the mean number of children per man for men older than 40 years in the Netherlands. *Statistically significantly different compared with men diagnosed ≥41 years.
After adjusting for potential confounders (current age, education level, history of cardiovascular disease, diagnosis of infertility in partner and diagnosis of RA, JIA and SpA) and considering the total number of children of men diagnosed ≥41 years as our reference group, we observed a statistically significant negative effect on the total number of children of men diagnosed ≤30 years (p=0.002) (see table 2). Furthermore, the total number of children per disease was not statistically significant between diseases.
Lastly, we compared the fertility rate of the study groups with the fertility rate of all men living in the Netherlands who at the time of our last inclusion were 40 years or older (1.79, Statistics Netherlands (CBS),personal communication, 18 August 2020). Compared with the fertility rate of men ≥40 years from the general population, the fertility rate of men diagnosed ≤30 and 31–40 years was statistically significant lower (1.32, p=0.001 and 1.56 p=0.03, respectively). The fertility rateof men diagnosed ≥41 years was not statistically significant different (1.88, p=0.128).
Analysis of covariance: effect of dichotomised age at diagnosis of IA (based on our study groups) on total number of children per man and considering the total number of children of men diagnosed ≥41 years as our reference group
Total number of pregnancies per man
In contrast to the fertility rate, where only live births are taken into account, the total number of pregnancies per man includes any positive pregnancy test independent of the final pregnancy outcome. Men diagnosed ≤30 years had a lower total number of pregnancies (1.45 (SD 1.37)) than men diagnosed between 31 and 40 years (1.73 (SD 1.69)) and men diagnosed ≥41 years (1.98 (SD 1.45)). There was a statistically significant difference between groups (p=0.0023). The total number of pregnancies was statistically significant lower in men diagnosed ≤30 years compared with men diagnosed ≥41 years (p=0.002). There were no statistically significant differences between men diagnosed <30 and 31–40 years (p=0.261) and between men diagnosed 31–40 and ≥41 years (p=0.219).
Childlessness
In the Netherlands, the percentage of childless men ranges between 20% and 25%.25 In total, 143 men (22.27%) were childless most of whom were voluntary childless (n=99 (69.23%)). The percentage of childless men was significantly higher in men diagnosed ≤30 years (n=45 (33.83%)) and in men diagnosed 31–40 years (n=39 (26.90%)) compared with men diagnosed ≥41 years (n=59 (17.25%), p=0.001).
In addition, we compared the percentages of voluntary and involuntary childlessness between the groups. The proportion of men who were voluntary childless was statistically significant different (29 (24.79), 24 (18.32) and 46 (14.64), p=0.048). The proportion of men who were involuntary childless was also statistically significant different between our groups (16 (12.03%), 15 (10.34%) and 13 (3.98%), p=0.001). Among childless men, the percentage of men who were involuntary childless was statistically significant between our groups (35.56% vs 38.46% vs 22.03%, p=0.046).
Desired number of children and family planning
The desired number of children was not statistically different between the three groups (1.75 (SD 1.32) vs 1.86 (SD 1.22) vs 2.03 (SD 1.18), p=0.083). Statistically significant more men diagnosed ≤31 years and 31–40 years reported feeling unsatisfied with their final number of children than men diagnosed ≥41 years (n=22 (16.67%), n=14 (9.66%) and n=18 (5.50%), p=0.010). Approximately one-third of these men reported that the diagnosis of IA and/or the medical treatment associated with it, were the main reason to have less children (31% and 28%, respectively).
The difference between desired and final number of children was significantly wider in men diagnosed ≤30 years (0.41 (SD 0.98)) compared with men diagnosed ≥41 years (0.14 (SD 0.77), p=0.003). Compared with men diagnosed 31–40 years, the difference between desired and final number of children was not statistically significant different (0.29 (SD 0.74), p=0.181) (see figure 2).

Comparison of the desired and final number of children per man for all participants and per group (mean+95% CI).
Furthermore, to analyse the impact of IA on the fertility rate of men who wanted to become a father, we conducted a subgroup analysis where all men who were voluntary childless were excluded (see table 3).
Analysis of covariance: effect of dichotomised age at diagnosis of IA (based on our study groups) on total number of children per man (excluding men who were voluntary childless) and considering the total number of children of men diagnosed ≥41 years as our reference group
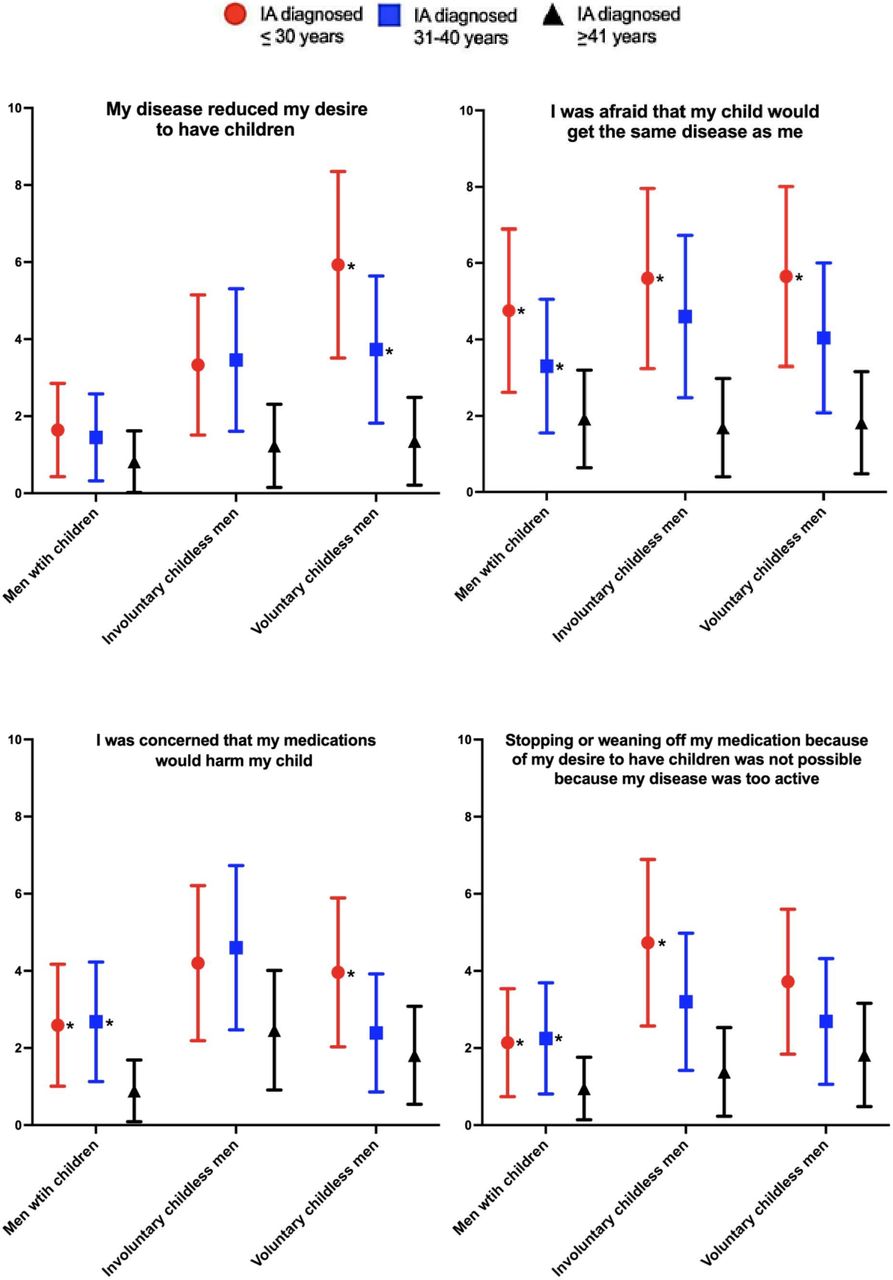
Using a Likert scale questionnaire, a significant negative effect of IA on family planning was reported by men diagnosed ≤30 and 31–40 years (see figure 3). Statements such as ‘I was concerned that my medications would harm my child’ or ‘I was afraid that my child would get the same disease as me’ were graded with a significantly higher degree of agreement among men diagnosed ≤30 and 31–40 years.

Likert scale questionnaire regarding the influence of Ia on family planning. men answered the questions using a 0–10 scale where 0 meant ‘totally disagree’ and 10 ‘totally agree’ (mean with SD) *P≤ 0.05 compared with those diagnosed age ≥41 years. **P≤0.05 compared with those diagnosed 31–40 years and ≥41 years. IA, inflammatory arthritis.
Moreover, among men who remained voluntary childless, the statement ‘My disease reduced my desire to have children’ was graded higher by men diagnosed ≤30 years (5.93 (2.42)) than by men diagnosed 31–40 years (3.73 (1.91)) and by men diagnosed ≥41 years (1.35 (1.14)). This was statistically significant different (p=0.001).Among men who remained involuntary childless and compared with men diagnosed ≥41 years, the statement ‘Stopping of weaning off my medication because of my desire to have children was not possible because my disease was too active’ was graded statistically significant higher by men diagnosed ≤30 years (see figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of the reported impact of Ia on different aspects of family planning in men with children, involuntary and voluntary childless men. A Likert scale with 0 meaning ‘totally disagree’ and 10 ‘totally agree’ was used (mean with SD). *p≤ 0.05 compared with those diagnosed age ≥41 years. IA, inflammatory arthritis.
Fertility
Statistically significantly more men diagnosed ≤30 and 31–40 years reported having received medical evaluations for fertility problems, compared with men diagnosed ≥41 years (n=27 (20.61%), n=30 (20.69%) and n=35 (11.36%), p=0.027) and ultimately receiving a diagnosis of low sperm quality (n=9 (6.57%), n=12 (8.05%) and n=12 (3.51%), p=0.086). Statistically significant more female partners of men diagnosed ≤30 years received a diagnosis of infertility secondary to an unknown cause (see table 4).
Fertility evaluation
In men who achieved a pregnancy, TTP was statistically significant higher in men diagnosed 31–40 years (6.74 (SD 11.12) months) compared with men diagnosed ≤41 years (4.77 (SD 8.47) months, p=0.045) and not statistically significantly different when compared with men diagnosed ≤30 years (5.69 (SD 10.93), p=0.623).
Discussion
Our study is the first of its kind to demonstrate that IA can significantly impair male fertility. The diagnosis of IA before or during the peak of the male reproductive age was associated with a lower fertility rate, lower number of pregnancies, higher rates of involuntary childlessness and fertility problems.
Respecting family planning we observed that the number of desired children per man was lower in men diagnosed before and during the peak of male reproductive age. Nonetheless, this was not statistically significant different between our groups and it was similar to the number of desired children per man reported for the general population of the Netherlands (1.81–2.29).26 Conversely, the difference between the desired and final number of children was significantly larger in men diagnosed before and during the reproductive age, indicating that the lower fertility rates are primarily affected by reduced fertility potential and not by a reduced desire for parenthood.
In this regard, men diagnosed with IA before and during the peak of their reproductive age were two times more likely to remain involuntary childless (12% and 10%). To put this into perspective, it is estimated that around 4% of healthy couples who want children remain involuntary childless.27
Moreover, it was shown that the diagnosis of IA may have a major impact on family planning. Not only did IA significantly reduce the desire to have children of men diagnosed before and during the peak of reproductive age who remained voluntary childless but also concerns or difficulties with regard to pharmacological treatment were larger in men diagnosed with IA before the peak of reproductive age who remained involuntary childless.
Lastly, the diagnosis of IA before and during the peak of reproductive age is associated with male fertility problems. These men were twice as likely to be evaluated for fertility problems and being subsequently diagnosed with abnormal sperm quality. In this regard, it has been estimated that abnormal sperm quality affects 2% of adult men.28 This estimation is considerably lower compared with the 6.5% and 8% reported by men diagnosed with IA before and during the peak of reproductive age.
Similar to our results, Uzunaslan et al reported that, compared with healthy men, men diagnosed with AS had statistically significant fewer children (1.9 vs 2.5) and a higher rate of infertility (9.1 vs 2.9%).29 These findings could be in part explained by the high incidence of varicocele and sperm abnormalities that have been reported for men diagnosed with AS.6 30 31 Nonetheless, this study was primarily designed to study the impact of Behçet’s syndrome on male fertility and only included 79 male patients diagnosed with AS.
Multiple mechanisms can be responsible for our findings. Biological mechanisms, namely inflammation, may contribute to the impaired fertility in men with IA. Several cytokines that are characteristic of the immune response associated with IA, such as tumour necrosis factor (TNF), play important roles in modulating testicular homoeostasis and regulating spermatogenesis.32 33 Increased expression of messenger RNA for interleukin-1-beta, TNF and interferon-gamma has been observed in testicular tissue of men with disturbed spermatogenesis.34 Correspondingly, inflammation may impair normal reproductive development before or during puberty, or have a direct negative impact on the spermatogenesis during the reproductive age.35–40
Beyond inflammation, pharmacological treatment associated with IA can also result in damage to the male reproductive axis.41 42 Moreover, side effects such as hypogonadism and low sperm quality have been associated with frequently used immunosuppressive agents.13 It has been estimated that among involuntary childless men that present to infertility clinics, 25% take drugs that have the potential to negatively impact male sexual function and 10% take drugs associated with male fertility impairment.42
Furthermore, several psychosocial factors, associated with a diagnosis of IA, may have contributed to the lower fertility rate as observed in this study.43 In our study, due to problems or concerns associated with IA and its treatment and based on medical advice (or the lack of), men with IA and their partners decided to become voluntarily childless or to delay their plans to become parents. These psychosocial factors were of special importance for men diagnosed before the peak of reproductive age. Moreover, some of these psychosocial factors could be associated with psychological comorbidities that are highly prevalent in patients diagnosed with IA such as depression and anxiety. These comorbidities have also been associated with sexual health problems.44–46
Our study has several strengths. It is the first large study (≥600 participants) specifically designed to detect statistically significant differences in a robust outcome measure (fertility rate). In addition, we used an extensive questionnaire to gain insight into most of the factors that might have influenced our primary outcome measure. Our study has important limitations. First, our response rate was low. However, the response rate is comparable to similar studies that explored male fertility rate in chronic diseases.22 Second, men diagnosed with chronic diseases and especially those who use pharmacological therapy are more aware of potential fertility problems47 48 and it can be expected that these men are more likely to seek fertility evaluation. Furthermore, men who experience fertility problems might be more willing to participate in these type of studies. Both factors are potential sources of selection bias in our study. In this respect, in the Netherlands, strict healthcare policies and referral guidelines reduce the possibility of self-referrals or unnecessary fertility evaluations. It is also reassuring that the response rates were similar between the three groups of men and that the results from our control group, men diagnosed ≥41 years, were strikingly similar to the data available in the general population further strengthening our comparisons. Lastly, this was a retrospective study. Recently, it has been shown that the sperm quality of male patients diagnosed with AS improved after being treated with TNF-α inhibitors.49 50 Furthermore, to get approval, new drugs are facing more strict protocols with regard to testicular toxicity. Therefore, the current conditions for men with IA, regarding treatment options and treatment strategies (biological therapy, shared-decision process, treat to target strategies), might be different than they were when our participants were in the peak of their reproductive age.
The results of this study may have several implications. In the clinical setting, rheumatologists should be aware that IA and/or the pharmacological treatment associated with IA may impair male fertility. Accordingly, they should discuss this with their patients, inform them about the impact of IA on male fertility and if indicated, adjust treatment aiming at low disease activity with the safest treatment strategy possible.6 50 For research purposes, basic, translational and epidemiological studies are needed to understand the impact of inflammation, pharmacological treatment and psychosocial factors associated with IA on male fertility. To corroborate our findings and to further describe the magnitude of the impact of IA on male fertility, large prospective studies are strongly recommended.
In conclusion, the diagnosis of IA before or during the peak of reproductive age can result in impaired male fertility. Rheumatologists should be aware of this novel association and approach their patients accordingly. Multiple biological and non-biological mechanisms can be responsible for this association and more research is urgently needed to improve the quality of care for men diagnosed with IA and a desire for parenthood.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study was reviewed by the ethics review boards of all participating centers in compliance with the Declaration of Helsinki. All patients gave their informed consent. 1. Erasmus MC - Ethics Committee: MEC-2018-1418. 2. Admiraal de Ruyter Hospital - Ethics Committee: ADRZ2019-010 iFAME-Fertility. 3. Franciscus Hospital - Ethics Committee: T-110. 4. Leiden University Medical Center, Reinier de Graaf Hospital, Haga Hospital - Ethics Committee: N19.081. 5. Maasstad Hospital - Ethics Committee: L2020040.
Acknowledgments
We extend our gratitude to Ron Buijs, data manager of the department of Rheumatology, Erasmus MC for his invaluable help with regards to technical support, data collection and data management. Additionally we would like to thank Annemarie Kraan-Donker, Ellis Niemantsverdriet and Marieke Holtrop for their important administrative and logistical contributions to the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Lay summary
Disclaimer : This is a summary of a scientific article written by a medical professional (“the Original Article”). The Summary is written to assist non medically trained readers to understand general points of the Original Article. It is supplied “as is” without any warranty. You should note that the Original Article (and Summary) may not be fully relevant nor accurate as medical science is constantly changing and errors can occur. It is therefore very important that readers not rely on the content in the Summary and consult their medical professionals for all aspects of their health care and only rely on the Summary if directed to do so by their medical professional. Please view our full Website Terms and Conditions.
Copyright © 2021 BMJ Publishing Group Ltd & European League Against Rheumatism. Medical professionals may print copies for their and their patients and students non commercial use. Other individuals may print a single copy for their personal, non commercial use. For other uses please contact our Rights and Licensing Team.
Footnotes
Handling editor Josef S Smolen
Twitter @DrReumatologo
Presented at EULAR 21 Virtual Congress
Contributors All authors met the authorship criteria, they had a substantial contribution to the conception or design of the work (LFPG, ER, HTWS, JMH, BPK, RJEMD) or the acquisition (LFPG, ER, RJEMD), analysis (LFPG, HTWS and RJEMD) or interpretation of data for the work (all authors) and were involved in revising a draft of this work, gave final approval of this version to be published, and are accountable for all aspects of the work in ensuring accuracy and integrity.
Funding This work was supported by research grants from the Dutch Arthritis Foundation (ReumaNederland) (project number: 16-3-402), ZonMw (project number 849200009) and Consejo Nacional de Ciencia y Tecnologia (CONACYT) (project number 601574). All are non-profit organizations.
Competing interests LFPG Consultant of: Galapagos, MRK Consultant of: Novartis, Grant/research support from: Novartis, RJEMD Speakers bureau: UCB, Roche, Abbvie, Genzyme, Novartis, Consultant of: Galapagos, Grant/research supportfrom: UCB.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.