Article Text

Abstract
Background: In the FINCH 1 study, filgotinib (FIL)—an oral, potent, selective Janus kinase 1 inhibitor—in combination with methotrexate (MTX) provided significant improvements in the signs and symptoms of rheumatoid arthritis (RA) in patients (pts) with inadequate response to MTX.1 While EULAR guidelines recommend a treat-to-target approach focusing on reducing inflammation to prevent joint damage, physical disability, and mortality, pts consider control of pain and fatigue, along with maintenance of physical function and health-related quality of life (HRQoL), to be important aspects for their care.2,3
Objectives: To evaluate the rate and magnitude of change in patient-reported outcomes (PROs) from FINCH 1.
Methods: In the FINCH 1 study (NCT02889796), pts with active RA received oral FIL 200 mg + MTX, FIL 100 mg + MTX, PBO + MTX, or subcutaneous adalimumab (ADA) 40 mg + MTX for up to 52 weeks (W); pts receiving PBO at W24 were rerandomised 1:1 to FIL 100 or 200 mg. PROs included the HAQ-DI and VAS pain scale, SF-36, and FACIT-Fatigue questionnaire. The change from baseline (CFB) at each time point was assessed up to W52 for each treatment group. The mixed-effects model for repeated measures was used to compare each FIL group with PBO for the CFB at each time point through W24. The logistic regression model was used to compare each FIL group with PBO for the proportion of pts achieving the minimum clinically important difference (MCID) of ≥0.22 reduction in CFB in HAQ-DI at each time point through W24.
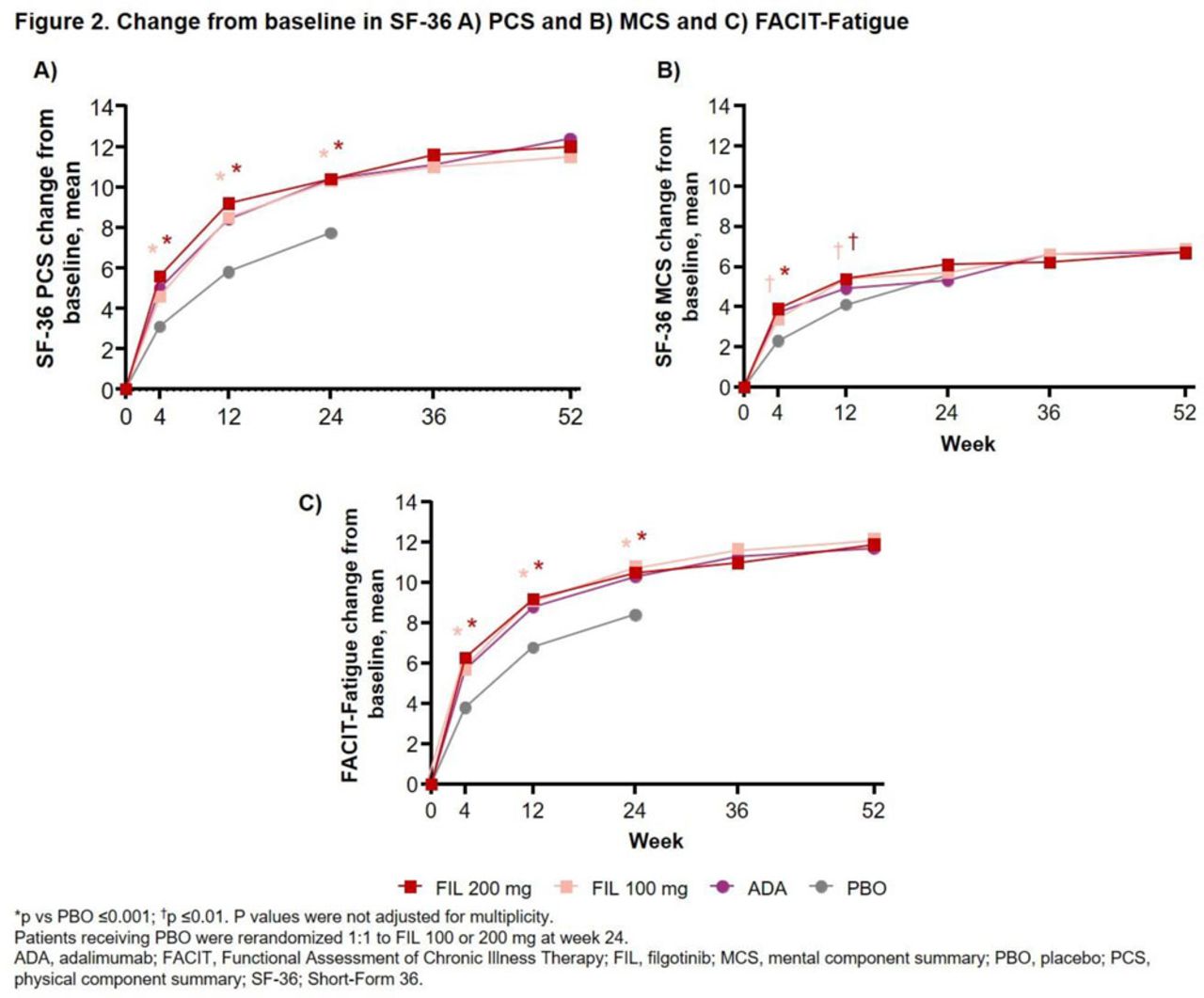
Results: Of 1755 pts randomised and treated (475 FIL 200 mg + MTX; 480 FIL 100 mg + MTX; 325 ADA + MTX; and 475 PBO + MTX), 1417 (80.7%) received study drug through W52. As early as W2 through W24, pts receiving either dose of FIL experienced nominally significantly greater (p <0.001) CFB in HAQ-DI and VAS pain scale than those receiving PBO; CFB improvements were maintained through W52 (Fig 1A, B). At W2, compared with PBO (40.2%), a nominally significantly greater proportion of pts achieved the HAQ-DI MCID in both the FIL 200 (52.5%; p <0.001) and 100 mg (46.7%; p = 0.043) groups. This benefit vs PBO was maintained up to W24 and the proportion of pts who achieved a HAQ-DI reduction of ≥0.22 remained ≥75.8% in the FIL 200 mg group and ≥71.5% in the FIL 100 mg group from W12 through W52. FIL provided nominally significantly greater improvement in HRQoL vs PBO at W4 and W12 for both the CFB of the SF-36 Physical Component Summary (PCS) (p <0.001) and Mental Component Summary (MCS) (p ≤0.006); nominal significance was also seen at W24 for CFB of SF-36 PCS (Fig 2A, B). By W4, pts receiving either dose of FIL reported a nominally significantly greater mean CFB in FACIT-Fatigue scores vs PBO (p <0.001); significance was maintained through W24 and improvement in reported fatigue continued through W52 in the FIL groups (Fig 2C). In general, CFB for HAQ-DI, VAS pain scale, and FACIT-Fatigue observed for the FIL groups was higher or comparable to ADA at various time points (Fig 1, 2).

{kind=link}
{kind=link}
Conclusion: Both doses of FIL provided rapid and sustained improvements in functional status, pain, HRQoL, and fatigue compared with PBO for pts with RA and inadequate response to MTX throughout the 52-week period.
References: [1]Combe BG, et al. Ann Rheum Dis. 2019;78 (Suppl 2):A77.
[2]Fautrel B, et al. Rheumatol Int. 2018;38:935–47.
[3]Smolen JS, et al. Ann Rheum Dis. 2017;76:960–77.
Disclosure of Interests: Alan Kivitz Shareholder of: AbbVie, Amgen, Gilead, GSK, Pfizer Inc, Sanofi, Consultant of: AbbVie, Boehringer Ingelheim,,Flexion, Genzyme, Gilead, Janssen, Novartis, Pfizer Inc, Regeneron, Sanofi, SUN Pharma Advanced Research, UCB, Paid instructor for: Celgene, Genzyme, Horizon, Merck, Novartis, Pfizer, Regeneron, Sanofi, Speakers bureau: AbbVie, Celgene, Flexion, Genzyme, Horizon, Merck, Novartis, Pfizer Inc, Regeneron, Sanofi, Yoshiya Tanaka Grant/research support from: Asahi-kasei, Astellas, Mitsubishi-Tanabe, Chugai, Takeda, Sanofi, Bristol-Myers, UCB, Daiichi-Sankyo, Eisai, Pfizer, and Ono, Consultant of: Abbvie, Astellas, Bristol-Myers Squibb, Eli Lilly, Pfizer, Speakers bureau: Daiichi-Sankyo, Astellas, Chugai, Eli Lilly, Pfizer, AbbVie, YL Biologics, Bristol-Myers, Takeda, Mitsubishi-Tanabe, Novartis, Eisai, Janssen, Sanofi, UCB, and Teijin, Susan Lee Shareholder of: Gilead Sciences Inc., Employee of: Gilead Sciences Inc., Lei Ye Shareholder of: Gilead Sciences Inc., Employee of: Gilead Sciences Inc., Hao Hu Shareholder of: Gilead Sciences Inc., Employee of: Gilead Sciences Inc., Robin Besuyen Shareholder of: Galapagos, Employee of: Galapagos, Bernard Combe Grant/research support from: Novartis, Pfizer, Roche-Chugai, Consultant of: AbbVie; Gilead Sciences, Inc.; Janssen; Eli Lilly and Company; Pfizer; Roche-Chugai; Sanofi, Speakers bureau: Bristol-Myers Squibb; Gilead Sciences, Inc.; Eli Lilly and Company; Merck Sharp & Dohme; Pfizer; Roche-Chugai; UCB