Article Text

Statistics from Altmetric.com
Pisetsky et al recently reported substantial variability between two antinuclear antibodies (ANA) indirect immunofluorescence (IIF) assays as well as one solid-phase assay (SPA) from different manufacturers in a study of a cross-sectional cohort of systemic lupus erythematosus (SLE) patients.1 This publication triggered several responses related to the performance of IIF for ANA detection.2–6 Bizzaro questioned whether ANA testing by IIF can be replaced by SPAs for the diagnosis of ANA-associated rheumatic disorders (AARD).7 On the basis of his experience and a literature review, he concluded that (1) overall screening by SPAs yields results that are at least comparable to the sensitivity of ANA-IIF results, (2) the performance of the assays depends on the disease being investigated and (3) the best diagnostic strategy seems to be the concomitant use of the two methods,7 which is in accord with previous suggestions.8
We hereby further illustrate that combining SPA with IIF adds value based on the data from a recently published study of 480 patients with AARD [SLE (n=119), primary Sjögren’s syndrome (SjS, n=65), systemic sclerosis (SSc, n=220), idiopathic inflammatory myopathies (IIM, n=50) and mixed connective tissue disease (n=56)] and 767 diseased controls.9 ANA detection was performed by automated IIF (NOVA View, Inova Diagnostics, San Diego, CA, USA) and by two automated SPAs, a chemiluminescent assay (CIA) and a fluoroenzyme immunoassay (FEIA). Both SPAs measure antibodies to a set of relevant AARD-associated autoantigens (for an overview of the antigens, see below legend).
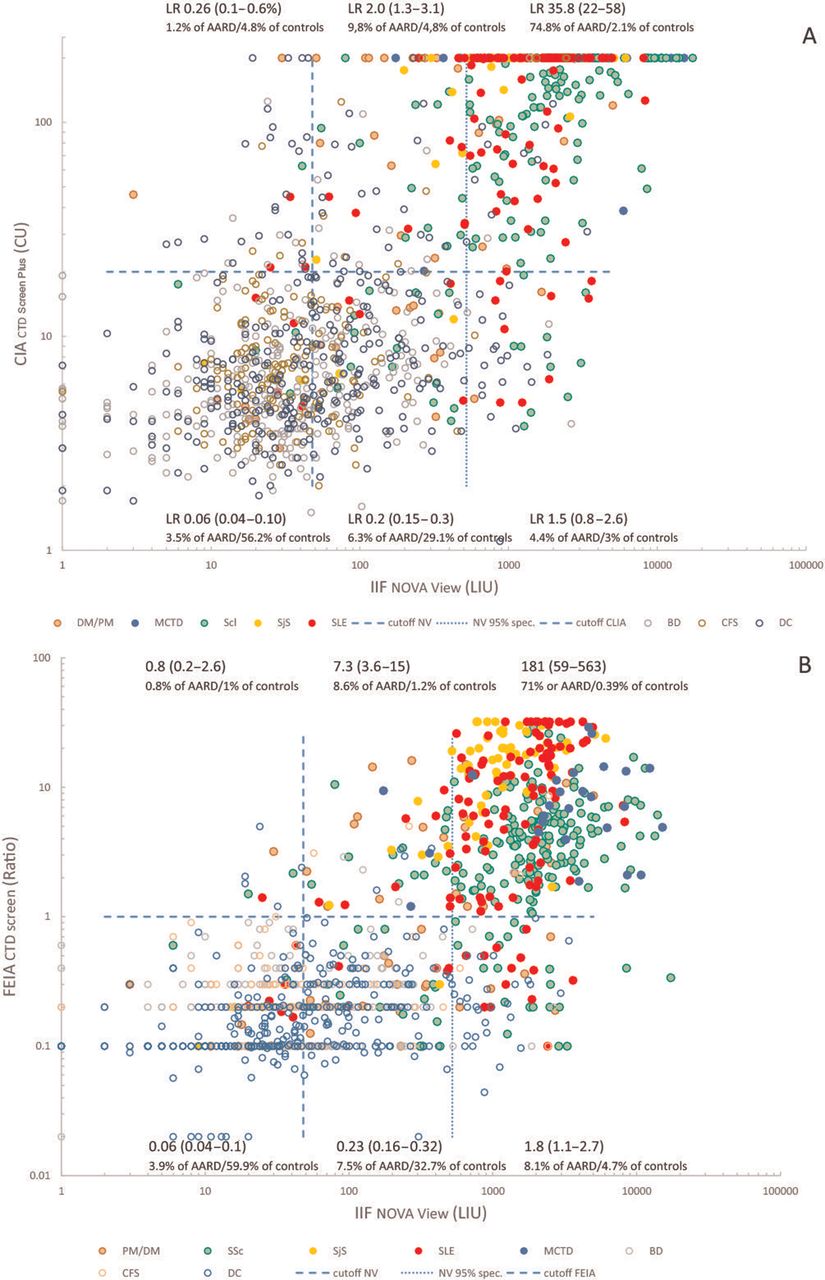
The results obtained by IIF, CIA and FEIA in patients with AARD and in controls are shown in figure 1, where the cut-off values for SPA and IIF as well as the IIF threshold that corresponded to a specificity of 95% are represented. These cut-off values and the 95% IIF specificity threshold divide the figure into six sections (categories).

{kind=link}
Results for IIF and CIA (A), and IIF and FEIA (B) obtained in patients with an AARD and controls. On the X-axis, the values obtained with automated IIF are given, on the Y-axis, the values obtained by SPA (CIA for panel A and FEIA for panel B). Cut-off values (thresholds) are indicated by dashed lines. For IIF, an additional threshold that corresponds to a specificity of 95% is given as well. The two cut-off values and the 95% IIF specificity value divides the figure into six section. For each section, the LR (with 95% CI) for AARD is given, as well as the fraction of AARD patients and controls that have such value. AARD, ANA-associated rheumatic disorders; ANA, antinuclear antibodies; CIA, chemiluminescent assay; FEIA, fluoroenzyme immunoassay; IIF, indirect immunofluorescence; SjS, Sjögren’s syndrome; SLE, systemic lupus erythematosus; SPA, solid-phase assay; SSc, systemic sclerosis.
Upper right category: applying the 95% specificity threshold, the majority of AARD patients [71%/75% for SLE, 75%/80% for SSc, 80% for SjS, 88% for MCTD and 30%/36% for IIM (first values for FEIA)] are positive for both SPA and IIF. The likelihood ratio for AARD for such results is high [36 (95% CI 22–58) for CIA and 181 (95% CI 59–563) for FEIA].
Lower right category: a proportion of AARD patients [11%/7.5% for SLE, 9.5%/4.5% for SSc and 10%/4% for IIM (first values for FEIA)] are negative by SPA but clearly positive by IIF (values>95% specificity threshold).
Upper and lower middle category: weak positive IIF results (values between the cut-off and the 95% specificity threshold) have a low LR for AARD [0.5 (95% CI 0.4–0.6)]. Within this group, SPA-positive results (upper middle section) have a higher LR [2 (95% CI 1–3) for CIA and 7 (95% CI 4–15) for FEIA] for AARD than SPA-negative results (lower middle section) [LR 0.2 (95% CI 0.15–0.3)].
Upper left category: SPA detects some SLE patients [0.8%/2.5% (first value for FEIA)] and SSc patients [0.4%/0.9% (first value for CIA)] that are negative by IIF.
Lower left category: only a small fraction of AARD patients is double-negative [5%/3% for SLE, 1.3%/1.8% for SSc, 6% for SjS and 12%/10% for IIM (first values for FEIA)]. The likelihood ratio for AARD for such results is low (0.06).
Taken together, double positive results detected by SPA and IIF are strongly associated with AARD. SPAs have good sensitivity for SjS, but fail to detect a sizeable proportion of SLE, SSc and IIM patients that have high IIF reactivity. On the other hand, in IIF weak positive or IIF negative patients, SPA can identify patients with a higher likelihood for AARD. Similar results were reported by Willems et al 10 and Op De Beeck et al.11
In conclusion, these data suggest that combining both SPA and ANA-IIF assay adds clinical value to the routine investigation of patients with suspected AARD.
Our figure 1 corresponds to figure 1 from Claessens et al,9 except that the different AARD diseases are distinguishable and that the IIF threshold that corresponds to a 95% specificity has been added. We received permission from Autoimmunity Reviews (editor) and Elsevier to use a modified version of figure 1.9
Automated IIF was performed by NOVA View, Inova Diagnostics, San Diego, CA, USA at a serum dilution of 1/80.
CIA was performed by QUANTA Flash CTD Screen Plus, Inova Diagnostics. The autoantigens include dsDNA, Sm/RNP, Ro60/SSA, Ro52/TRIM21, SS-B/La, centromere (A and B), Scl-70/topoisomerase I, Mi-2, RNA-Pol III, PM/Scl, Jo-1, PCNA, Ribosomal-P protein (C22 peptide), Ku and Th/To.
FEIA was performed by EliA CTD screen, Thermo Fisher, Freiburg, Germany. The autoantigens include dsDNA, Sm, SSA/Ro60 and Ro52/TRIM21, SS-B/La, centromere B, Scl-70/topoisomerase I, Mi-2, RNA-Pol III, PM/Scl, Jo-1, PCNA, Ribosomal-P protein, U1-RNP (RNP-70, A, C) and fibrillarin.
Footnotes
Contributors JC acquired the data and analysed the data. EDL, RW and DB took care of the patients and helped with clinical classification of the patients. MJF, TB and SH provided patient sera and clinical data. MM provided reagents and discussed the data. XB analysed the data and wrote a draft of the manuscript. All authors reviewed the draft and approved the submission of the manuscript.
Funding This study was supported by Inova Diagnostics.
Competing interests XB has been a consultant for Inova Diagnostics and Thermo Fisher. MJF has been a consultant for Inova Diagnostics. MM is employed by Inova Diagnostics. Inova Diagnostics provided reagents to perform the study.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.