Article Text

Abstract
Objectives In the phase II FGF-18 Osteoarthritis Randomized Trial with Administration of Repeated Doses (FORWARD) study, sprifermin demonstrated cartilage modification in the total femorotibial joint and in both femorotibial compartments by MRI in patients with knee osteoarthritis. Here, we evaluate whether sprifermin reduces cartilage loss and increases cartilage thickness, independent of location.
Methods Patients were randomised 1:1:1:1:1 to three once-weekly intra-articular injections of 30 µg sprifermin every 6 months (q6mo); 30 µg sprifermin every 12 months (q12mo); 100 µg sprifermin q6mo; 100 µg sprifermin q12mo; or placebo. Post-hoc analysis using thinning/thickening scores and ordered values evaluated femorotibial cartilage thickness change from baseline to 24 months independent of location. Changes were indirectly compared with those of Osteoarthritis Initiative healthy subjects.
Results Thinning scores were significantly lower for sprifermin 100 µg q6mo versus placebo (mean (95% CI) difference: 334 µm (114 to 554)), with a cartilage thinning score similar to healthy subjects. Thickening scores were significantly greater for sprifermin 100 µg q6mo, 100 µg q12mo and 30 µg q6mo versus placebo (mean (95% CI) difference: 425 µm (267 to 584); 450 µm (305 to 594) and 139 µm (19 to 259), respectively) and more than doubled versus healthy subjects.
Conclusions Sprifermin increases cartilage thickness, and substantially reduces cartilage loss, expanding FORWARD primary results.
Trial registration number NCT01919164.
- knee osteoarthritis
- MRI
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Clinical studies support the structure-modifying effects of sprifermin, a recombinant human fibroblast growth factor 18, in patients with knee osteoarthritis. The 2-year primary analysis of the phase II FORWARD study demonstrated statistically significant dose-dependent modification of change in cartilage thickness in the total femorotibial joint (TFTJ), medial and lateral femorotibial joints, and central medial and lateral TFTJ subregions with intra-articular sprifermin.
MRI is commonly used for measuring cartilage thickness changes in specific femorotibial regions in clinical trials. However, region-specific analysis cannot elucidate whether cartilage loss is reduced, wherever it occurs in an individual joint. Application of location-independent analysis methodology can provide a more sensitive and informative analysis of cartilage loss and thickening independent of the location where it occurs.
What does this study add?
This post-hoc exploratory analysis reports cartilage thickness change based on thinning/thickening scores and ordered values of subregional cartilage thickness change for patients with knee osteoarthritis enrolled in the FORWARD study between baseline and 24-month follow-up. It shows that treatment with sprifermin increases cartilage thickness and reduces cartilage loss. Corresponding results for healthy reference subjects from the Osteoarthritis Initiative were summarised to indirectly compare changes in thinning/thickening scores with FORWARD study patients. This comparison to the reference set indicates that thickening more than doubled, whereas thinning almost reduced to the level of healthy subjects, providing strong support for substantial cartilage modification by sprifermin.
Key messages
How might this impact on clinical practice or future developments?
There are currently no disease- (or structure-) modifying osteoarthritis drugs (DMOADs) approved for use in Europe or the USA.
Primary results from the FORWARD study combined with findings from this post-hoc analysis suggest that sprifermin should be evaluated further in clinical trials as a potential DMOAD therapy for knee osteoarthritis that can substantially reduce cartilage loss.
Introduction
Osteoarthritis (OA) is characterised by loss of articular cartilage, which is associated with clinical outcomes including knee replacement.1 2 Whereas current treatments alleviate symptoms without targeting structural progression,3 disease-modifying OA drugs (DMOADs) aim to modify tissue structure, such as articular cartilage, ideally in conjunction with improving clinical outcomes.4 5 No DMOADs have yet been approved in the USA or Europe.
Clinical studies support the structure-modifying effects of the recombinant human fibroblast growth factor 18, sprifermin, in knee OA.6–8 The 2-year primary analysis of the phase II FORWARD study demonstrated statistically significant dose-dependent modification of cartilage thickness change by quantitative MRI in the total femorotibial joint (TFTJ), and (central) medial and lateral femorotibial compartments with intra-articular (i.a.) sprifermin.8
MRI can measure cartilage thickness change in femorotibial subregions.9 Yet, region-specific analysis cannot elucidate whether cartilage loss is reduced wherever it occurs in an individual joint. Location-independent analysis methodology, based on ordering subregional cartilage thickness change, provides a more sensitive and informative analysis of cartilage loss and thickening.9–12 Location-independent methods were used in a 1-year, placebo-controlled, proof-of-concept phase Ib study,7 which suggested that i.a. sprifermin reduced cartilage loss in addition to increasing cartilage thickness.10 However, this used a small sample size, and the extent to which structure modification affected the cartilage thinning score compared with healthy subjects was not studied.
We conducted a post-hoc, exploratory analysis using thinning/thickening scores and ordered values (OVs) calculated from the larger FORWARD study, to evaluate whether sprifermin reduces cartilage loss independent of location in a given knee, in addition to the dose-dependent increase in mean cartilage thickness in the TFTJ.8 Further, we indirectly compared changes in thinning/thickening scores10 in FORWARD8 with those in healthy reference subjects from the Osteoarthritis Initiative (OAI).13–15
Methods
FORWARD study design
FORWARD is a multicentre, randomised, double-blind, placebo-controlled, dose-finding, phase II, 5-year study (NCT01919164). Study methods have been reported previously.8 Briefly, patients aged 40–85 with symptomatic radiographic knee OA, Kellgren-Lawrence Grade 2 or 3, and medial minimum joint space width ≥2.5 mm in the target knee were randomised (1:1:1:1:1) to receive three once-weekly i.a. injections of: 30 µg sprifermin every 6 months (q6mo); 30 µg sprifermin every 12 months (q12mo); 100 µg sprifermin q6mo; 100 µg sprifermin q12mo; or placebo. The primary endpoint was change in total TFTJ cartilage thickness from baseline to 2 years, by quantitative MRI. See online supplementary file 1 for patient involvement information.
Supplemental material
Structural change measurements
Clinical MRI scanners (1.5/3 Tesla (T)) obtained MRI acquisitions8 for assessing cartilage thickness in 16 femorotibial subregions.16
Changes in subregional cartilage thickness between baseline and 24 months were ranked by magnitude to create 16 location-independent OVs, as described previously.10–12 OV1 corresponded to the largest loss/smallest gain and OV16 to the smallest loss/largest gain in cartilage thickness in any subregion within each knee. Thinning and thickening scores for each knee were defined as the sum of each of the 16 subregions with negative and positive changes, respectively.10 11 To determine the relationship between cartilage loss and gain, the ratio of the thickening to thinning score was calculated for each patient. Mean thinning/thickening scores were informally compared with measurements from an OAI reference group,17 comprising 82 healthy subjects without radiographic knee OA, who were assessed at baseline and 24 months using the same image acquisition and analysis technology16 as in the FORWARD study.8 Healthy reference subjects from the OAI had no knee pain, no radiographic signs of knee OA and no risk factors for knee OA.13
Statistical analysis
In this exploratory, post-hoc analysis, differences between treatment groups were evaluated using a t-test, without adjusting for multiple comparisons. Patients in the modified intent-to-treat (mITT) population who had baseline and 24-month MRI data (thinning/thickening analysis set) were included. All endpoints were considered exploratory.
Results
Patients
Baseline characteristics for the thinning/thickening score analysis set (online supplementary table 1) were similar to those previously reported for the mITT population.8
Cartilage thinning and thickening scores
Thinning scores were lower for all sprifermin doses versus placebo; statistically significantly less thinning was observed for the highest sprifermin dose (100 µg q6mo; table 1). Thinning scores with this dose approached those observed in OAI healthy reference subjects over the same 24-month observation period.
Mean (95% CI) thinning and thickening scores by FORWARD treatment group (modified intent-to-treat population) and in the Osteoarthritis Initiative healthy reference cohort over 24 months
Thickening scores were substantially greater with sprifermin versus placebo; differences were statistically significant for the 100 µg q6mo, 100 µg q12mo and 30 µg q6mo dose groups. The highest doses (100 µg q6mo and q12mo) of sprifermin approximately doubled the cartilage thickening score compared with placebo and OAI healthy reference subjects (table 1).
The thickening:thinning score ratio was 1.06 in OAI healthy reference subjects, indicating no net loss or gain of cartilage. For the sprifermin 100 µg q6mo and q12mo dose groups, the thickening:thinning score ratio was higher than that obtained for the OAI healthy reference subjects (1.98 and 1.48, respectively), indicating cartilage thickness gain. The thickening:thinning score ratio was lower in the placebo group (0.56) versus OAI healthy reference subjects, indicating cartilage thickness loss (figure 1).
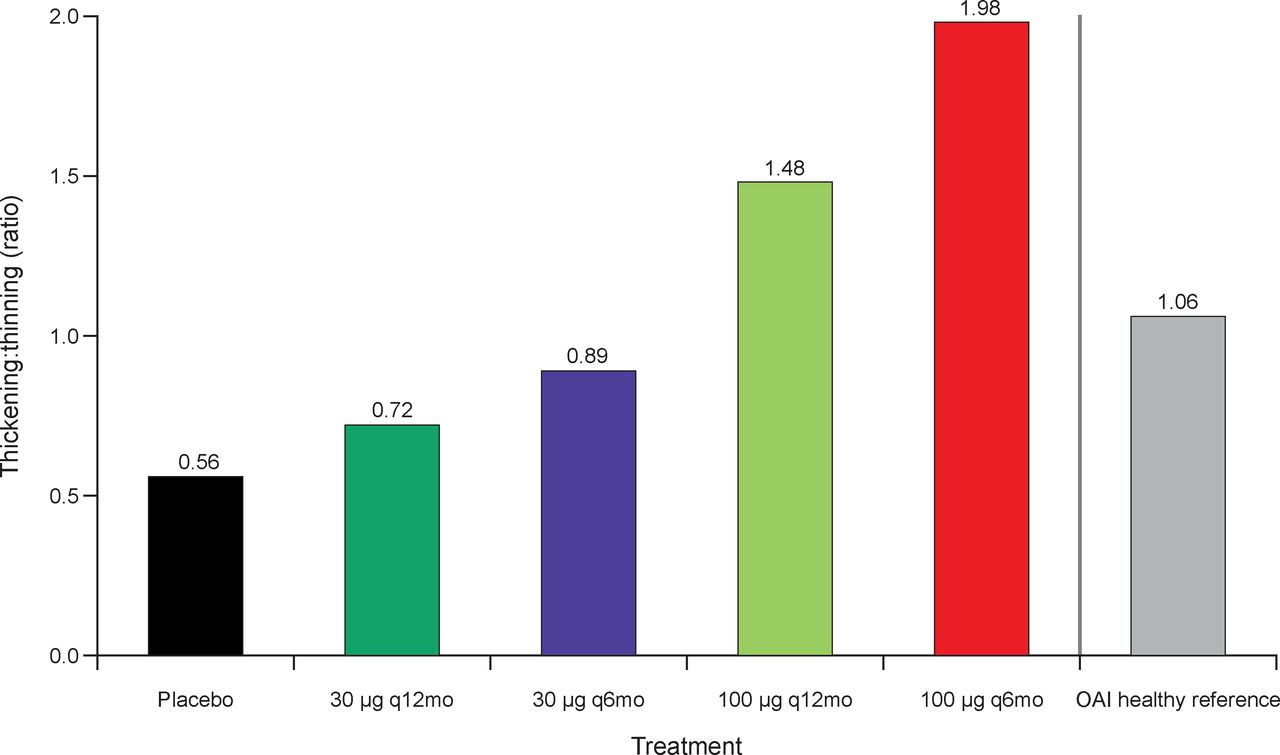
Ratio of thickening:thinning scores by FORWARD treatment group (modified intent-to-treat population) and in the Osteoarthritis Initiative healthy reference cohort over 24 months. q6mo, every 6-month active cycles; q12mo, every 12-month active cycles.
OVs and subregion analysis
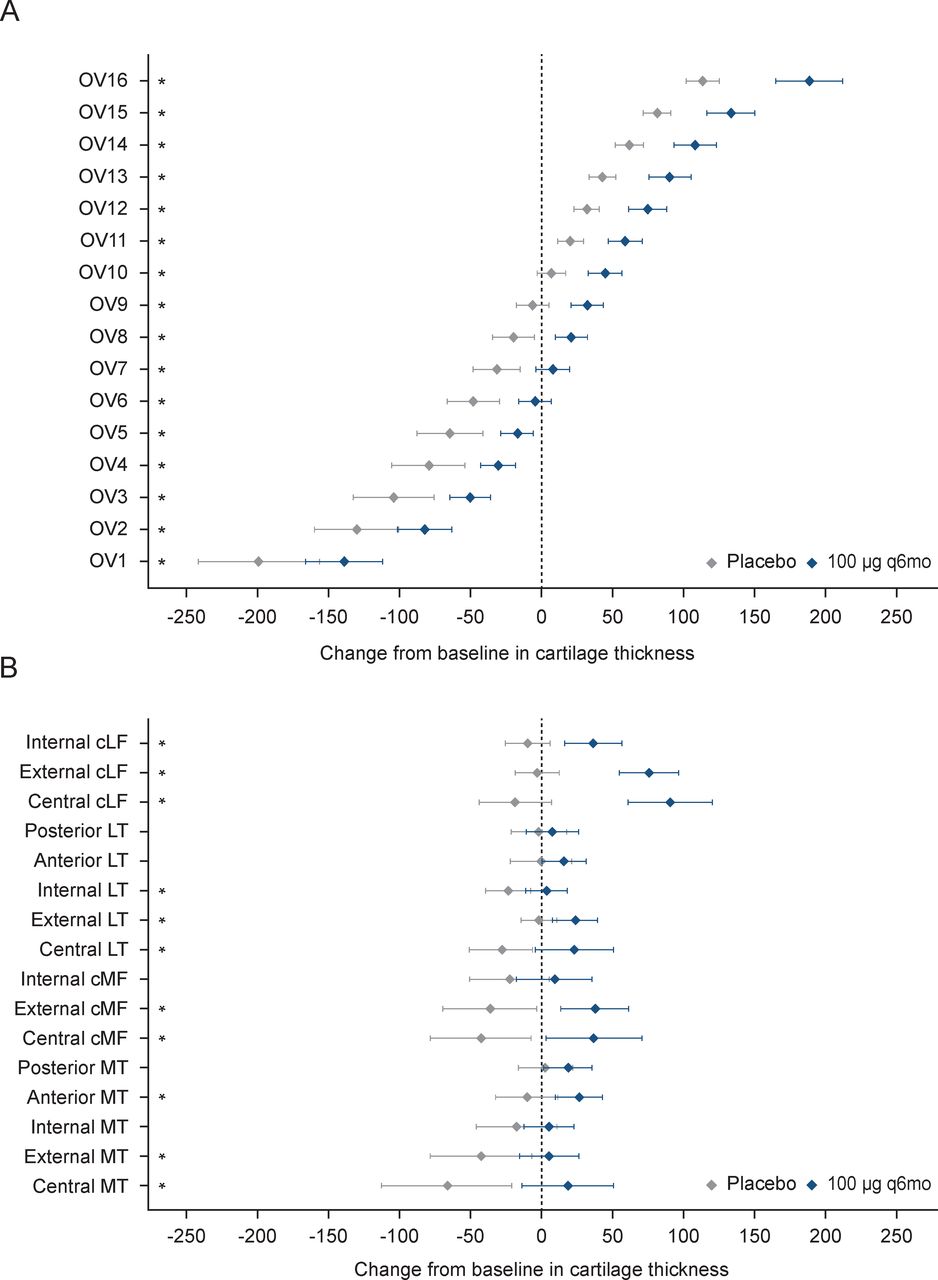
Sprifermin-treated patients (100 µg q6mo) gained more and lost less cartilage thickness across OVs versus placebo-treated patients over 24 months; the difference reached statistical significance in all 16 OVs (figure 2A; online supplementary table 2). The decrease from baseline was substantially lower in OV1 (the largest loss in cartilage thickness in any subregion within each knee) and the increase substantially greater in OV16 (the largest gain in any subregion within each knee) with sprifermin than placebo.
Supplemental material
{kind=link}
{kind=link}
Mean change from baseline (95% CI) in cartilage thickness (μm) over 24 months for (a) 16 OVs and for (b) the 16 subregions in the sprifermin 100 µg q6mo and placebo groups (modified intent-to-treat population). CLF, condyle lateral femur; CMF, condyle medial femur; LT, lateral tibia; MT, medial tibia; OV, ordered value; q6mo, every 6-month active cycle. *Denotes statistically significant treatment effect: t-test p value<0.05.
Change in cartilage thickness from baseline to 24 months was modified significantly with sprifermin 100 µg versus placebo in 11 of 16 femorotibial subregions. The greatest differences were observed in the central lateral femur and central medial tibia (figure 2B; online supplementary table 3).
Supplemental material
Discussion
This is the largest study, to date, to apply location-independent analysis of cartilage change in a DMOAD trial, and the first to compare cartilage thinning/thickening scores from treated patients versus healthy reference subjects. Location-independent analysis of thinning and thickening scores demonstrated efficacy with sprifermin over 24 months, whereby sprifermin increased cartilage thickness, and substantially reduced cartilage loss compared with placebo. Thinning scores with sprifermin 100 µg q6mo were approaching those observed in OAI healthy reference subjects, whereas thickening scores were more than doubled.
In a subset of the OAI progression cohort, the greatest per cent change and sensitivity to change in cartilage thickness were observed in the external and central medial tibia, and in the central medial femoral condyle.17 These regions might be assumed to represent high load-bearing regions of the joint and regions with pre-existing cartilage damage. Sprifermin did not appear to be less effective in these subregions than in other subregions in the medial compartment or in the lateral tibia. Indeed, one of the regions with the greatest difference between sprifermin and placebo was the central medial tibia.
Limitations were potential for type 1 error due to multiple comparisons, and use of healthy reference subjects from a different cohort (the OAI13); consequently, caution must be applied when interpreting the data. However, subjects in the OAI study cohort were of a similar age to the FORWARD population and the studies used the same MR imaging sequences, orientation (coronal), parameters, spatial resolution and analysis technology.18 Additionally, the current analysis did not evaluate the association of the modification of thinning/thickening scores with change in pain and/or inflammation (synovitis). Although a potential limitation, as 1.5 T MRI has a slightly lower signal-to-noise ratio than 3 T, precision errors have been shown to be only marginally greater at 1.5 T, and thickness measures were consistent between 1.5 T and 3 T.19
Key strengths of this study include the robust design and relatively large sample size of FORWARD, and the comparison of findings with healthy reference subjects. In knee OA, some knees show preferential changes in the medial compartment, while others show greater changes in the lateral compartment.12 Clinical trials often do not account for differences in disease laterality, or restrict observations to those with only medial disease, limiting generalisation to subjects with lateral OA. In contrast, FORWARD intentionally included patients with both medial and lateral disease. In this context, location-independent analysis is particularly advantageous, as it covers cartilage thinning and thickening wherever it occurs in a joint, independent of the compartment and location primarily affected. Thinning/thickening scores and OVs were shown to be sensitive and efficient methods for measuring independent changes in cartilage thickness in either direction.9–12 In contrast, global or regional cartilage volume or thickness measurements may miss increases or decreases in cartilage thinning or thickening that occur simultaneously in a joint, although in different subregions.11 Furthermore, such measurements cannot be used to discriminate between an increase in cartilage thickening (in some regions) in isolation, or in combination with modification of cartilage thinning at any given position within a joint.9–12
The current results support the concept that sprifermin increases cartilage thickness, and reduces cartilage loss. They expand the primary FORWARD results, showing structural modification of cartilage thickness with sprifermin.8 Sprifermin should be evaluated further in clinical trials as a potential DMOAD for knee OA.
Acknowledgments
The authors would like to thank the FORWARD patients and their families, the study investigators at each participating site and study committee team members. Medical writing assistance was provided by Jen Shepherd PhD, Bioscript Group, Macclesfield, UK and supported by Merck KGaA, Darmstadt, Germany, in accordance with Good Publication Practice guidelines (http://www.ismpp.org/gpp3).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Presented at This work was previously presented at OARSI 2018 (Poster No. 551).
Contributors AA contributed to study design, data analysis, data interpretation and writing of the manuscript. FE contributed to study design, data collection, data analysis, data interpretation and writing of the manuscript. JK contributed to the data interpretation and writing of the manuscript. SM and WW contributed to data collection, data analysis, data interpretation and writing of the manuscript.
Funding The FORWARD study was funded by Merck KGaA, Darmstadt, Germany and EMD Serono Research & Development Institute, Inc. (a business of Merck KGaA, Darmstadt, Germany).
Competing interests FE is CEO of Chondrometrics GmbH and has received consulting fees from Merck KGaA, Samumed LLC, Abbvie, Bioclinica, Kolon TissueGene, Servier, Galapagos, Novartis and Roche. JLK and AA are employees of EMD Serono Research & Development Institute, Inc. (a business of Merck KGaA, Darmstadt, Germany). WW and SM are co-owners and employees of Chondrometrics GmbH, and WW has received consulting fees from Galapagos. MCH has received consulting fees from Bristol Myers Squibb, Eli Lilly, EMD Serono Research & Development Institute, Inc., Flexion Therapeutics, Galapagos, Hofmann LaRoche, IBSA Biotechniq SA, Novartis Pharma AG, Pfizer, Plexxikon, Samumed LLC, Symic Bio, Theralogix LLC, TissueGene, TLC Biopharmaceuticals and Zynerba.
Patient consent for publication Not required.
Ethics approval The study was conducted in accordance with the Declaration of Helsinki, the International Conference on Harmonisation Guidelines for Good Clinical Practice and local regulations. The study protocol and all major amendments were approved by the relevant Institutional Review Boards or Independent Ethics Committees and by Health Authorities, according to country-specific laws.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Any requests for data by qualified scientific and medical researchers for legitimate research purposes will be subject to Merck’s Data Sharing Policy. All requests should be submitted in writing to Merck’s data sharing portal (https://www.merckgroup.com/en/research/our-approach-to-research-and-development/healthcare/clinical-trials/commitment-responsible-data-sharing.html). When Merck has a co-research, co-development, or co-marketing or co-promotion agreement, or when the product has been out-licensed, the responsibility for disclosure might be dependent on the agreement between parties. Under these circumstances, Merck will endeavour to gain agreement to share data in response to requests.