Article Text

Abstract
Objective To assess if arthroscopic partial meniscectomy (APM) is superior to placebo surgery in the treatment of patients with degenerative tear of the medial meniscus.
Methods In this multicentre, randomised, participant-blinded and outcome assessor-blinded, placebo-surgery controlled trial, 146 adults, aged 35–65 years, with knee symptoms consistent with degenerative medial meniscus tear and no knee osteoarthritis were randomised to APM or placebo surgery. The primary outcome was the between-group difference in the change from baseline in the Western Ontario Meniscal Evaluation Tool (WOMET) and Lysholm knee scores and knee pain after exercise at 24 months after surgery. Secondary outcomes included the frequency of unblinding of the treatment-group allocation, participants' satisfaction, impression of change, return to normal activities, the incidence of serious adverse events and the presence of meniscal symptoms in clinical examination. Two subgroup analyses, assessing the outcome on those with mechanical symptoms and those with unstable meniscus tears, were also carried out.
Results In the intention-to-treat analysis, there were no significant between-group differences in the mean changes from baseline to 24 months in WOMET score: 27.3 in the APM group as compared with 31.6 in the placebo-surgery group (between-group difference, −4.3; 95% CI, −11.3 to 2.6); Lysholm knee score: 23.1 and 26.3, respectively (−3.2; −8.9 to 2.4) or knee pain after exercise, 3.5 and 3.9, respectively (−0.4; −1.3 to 0.5). There were no statistically significant differences between the two groups in any of the secondary outcomes or within the analysed subgroups.
Conclusions In this 2-year follow-up of patients without knee osteoarthritis but with symptoms of a degenerative medial meniscus tear, the outcomes after APM were no better than those after placebo surgery. No evidence could be found to support the prevailing ideas that patients with presence of mechanical symptoms or certain meniscus tear characteristics or those who have failed initial conservative treatment are more likely to benefit from APM.
- knee osteoarthritis
- orthopaedic surgery
- treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Arthroscopic partial meniscectomy (APM) is one of the most common orthopaedic operations,1 with an incidence that has increased steadily from 1990s until late 2010s.2–5 Most APMs are carried out in middle-aged and older patients with knee symptoms and degenerative knee disease.1 2 Several recent meta-analyses based on randomised controlled trials (RCTs) have failed to show a treatment-benefit of APM over conservative treatment or placebo surgery for these patients.6–10
Aligned with the evidence, most guidelines and expert opinion now refrain from recommending APM as the first-line treatment for patients with a degenerative meniscus tear, but still advocate surgery after a failed attempt of conservative treatment.11–16 Such recommendations rest on three issues: generally favourable clinical experience, some before-after studies on patients undergoing APM due to persisting symptoms despite conservative treatment17 18 and particularly the evidence from three RCTs19–21 in which one-third of participants initially allocated to non-surgical treatment opted for crossing over to APM due to persisting knee symptoms or insufficient improvement. After undergoing APM, participants achieved similar outcomes compared with those initially assigned to surgery and those responding favourably to initial non-surgical/conservative treatment.19–21 These findings have been interpreted as evidence that APM should be performed after failed conservative treatment.22 Although such hypotheses might well be true, an alternative accounting can explain the number of crossovers and the beneficial treatment effects of surgery after failed conservative treatment: lack of blinding (participants’ knowledge of not having undergone surgery) may drive conservatively treated patients to request surgery and also make them feel more content with the outcome once having undergone surgery.23 24
In addition to patients failing to improve after conservative treatment, other subgroups considered to benefit from APM are those with so-called ‘mechanical symptoms’25–28 or those with ‘unstable’ meniscal tear.15 17 28
Accordingly, the aim of this extension of our recently published Finnish Degenerative Meniscal Lesion Study (FIDELITY) trial29 was twofold: (a) to assess if APM is superior over placebo surgery over the course of 24-month follow-up determined using patient relevant outcomes, the frequency of unblinding of the treatment-group allocation and clinical examination of the knee and (b) to assess whether our data corroborates or refutes common assertions regarding existence of subgroups of patients likely to benefit from APM.
Materials and methods
We conducted a multicentre, randomised, participant-blinded and outcome assessor-blinded, placebo-surgery controlled efficacy trial involving participants aged 35–65 years with knee symptoms over 3 months, consistent with degenerative medial meniscus tear and unresponsive to conventional conservative treatment and no clinical30 or radiographic (Kellgren-Lawrence grade ≤1)31 knee osteoarthritis. The study took place in five orthopaedic centres in Finland during the period from December 2007 through March 2014. All patients had a suspicion of a meniscus tear based on symptoms and clinical tests, a tear that was later verified on both MRI and knee arthroscopy. Patients with an obvious trauma-induced onset of symptoms or with a recent history of a locked knee were excluded from the trial. On entering the study, participants were informed that they would be allowed to consider a reoperation 6 months or later after the procedure if they did not have adequate relief of symptoms.
Participants first underwent diagnostic knee arthroscopy and then (during the same operation) were assigned to APM or placebo surgery. For the randomisation, the sequentially numbered, opaque, sealed envelopes were prepared by a statistician. Randomisation was performed in a 1:1 ratio with a block size of 4, and with stratification according to study site, age (35–50 or 51–65 years), sex and the absence or presence of minor degenerative changes on a radiograph (Kellgren-Lawrence grade 0 or 1, respectively).
The participants, all caregivers and those assessing the outcomes were blinded to the treatment assignment. Participants were followed-up by questionnaires at 2, 6, 12 and 24 months. At the 24-month follow-up, all participants were also clinically examined by an independent orthopaedic surgeon unaware of the treatment allocation. Standardised clinical examination included clinical meniscal tests32: McMurray test,33 pain provoked by joint line palpation and pain provoked by forced flexion and varus. Also, range of knee motion, knee crepitus, bony enlargement, effusion, location of pain at palpation and knee stability was recorded.
The study was registered at ClinicalTrials.gov (NCT00549172). We have described the design34 and published the 12-month results29 of the trial previously. The protocol was approved by the institutional review board of the Pirkanmaa Hospital District (R 06157). The study was conducted in accordance with the Declaration of Helsinki. All participants gave written informed consent.
Interventions
Arthroscopic evaluation included recording the presence of intra-articular pathology (meniscus tears, loose bodies and characterisation of chondral lesions of both tibiofemoral and patellofemoral chondral surfaces) according to the International Cartilage Repair Society cartilage injury classification scale35 and the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine classification of meniscal tears.36
During the APM, the damaged and loose parts of the meniscus were removed with the use of arthroscopic instruments until solid meniscal tissue was reached with preservation of as much of the meniscus as possible. No other surgical procedure was performed. For the placebo surgery, APM was simulated to mimic the sensations and sounds of a true APM. The participants were also kept in the operating room for the amount of time required to perform an actual APM.
In both the APM and the placebo-surgery groups, postoperative care was delivered according to a standardised protocol specifying that all participants receive the same walking aids and instructions for the same graduated home-based exercise programme.
Outcomes
Primary outcomes were the change in Western Ontario Meniscal Evaluation Tool (WOMET), the Lysholm knee score and pain after exercise from baseline to 24 months after surgery. The WOMET37 is a meniscus-specific health-related quality-of-life instrument, validated especially for patients with a degenerative meniscal tear.38 The Lysholm knee score is a validated, condition-specific outcome measure.39 40 WOMET and Lysholm scores each range from 0 to 100, with 0 indicating the most severe symptoms and 100 the absence of symptoms. Knee pain (during the preceding week) was assessed on an 11-point numerical rating scale ranging from 0 (no pain) to 10 (extreme pain).
As a secondary outcome, the frequency of patients in the two treatment groups who did not have adequate relief of symptoms and whose treatment-group allocation was therefore unblinded was determined. Participants were also asked to respond to the following questions: “Are you satisfied with your knee at present?” and “ Is your knee better than before the intervention?” on a 5-point Likert scale. As before,41 the responses ‘very satisfied’ or ‘satisfied’ were categorised as satisfied, while responses ‘neither satisfied nor dissatisfied’, ‘dissatisfied’ and ‘very dissatisfied’ were categorised as dissatisfied. Similar to satisfaction, the responses ‘much better’ and ‘better’ were considered to indicate improvement, while responses ‘unchanged’, ‘worse’ or ‘much worse’ were deemed not improved. Serious adverse events were registered. In addition, the participants were asked whether or not they were able to return to their previous activities. Finally, the frequency of participants with a positive meniscus test at clinical examination was assessed.
APM was also compared with placebo surgery within two subgroups of participants, those with mechanical symptoms of the knee and those with unstable meniscus tear. The presence of mechanical symptoms was assessed using the locking domain question of the Lysholm knee score.39 In brief, we asked patients to choose one out of five following responses that best reflected the status of their knee: i) no locking or catching, ii) catching sensations but no locking, iii) occasional locking, iv) frequent locking or v) locked at present. Meniscus tears with longitudinal tear pattern, bucket handle tear or flap were determined as unstable, whereas radial, horizontal and complex were determined as stable.13
Patient involvement
There was no active patient involvement in the design of the study, in the recruitment to or conduct of the study. However, one of the main outcome measures (the WOMET) was initially developed with a patient-centred approach: the items included in the final version of the questionnaire were those identified by patients to impact most significantly on their quality of life.37 The results of this RCT will be conveyed to the participants in lay language in a pamphlet distributed by mail after the 5-year follow-up.
Statistical methods
The trial was designed to ascertain whether APM is superior to placebo surgery in treating patients with knee pain and a degenerative meniscus tear. Baseline characteristics were analysed with the use of descriptive statistics. For the primary analysis, the change in each score (mean with 95% CI) from baseline to 24 months was compared between the two study groups. This analysis was also performed after adjustment for the baseline score and for the stratifying variables used for randomisation. The study was powered to detect a minimal clinically important improvement in the WOMET and Lysholm scores (described as improvements of at least 15.5 and 11.5 points, respectively) and in the score for knee pain after exercise (improvement of at least 2.0 points).34 For the secondary analyses, the frequency of assessed outcomes were compared between the two groups. Two subgroup analyses were carried out, for those with mechanical symptoms and for those with unstable meniscus tear; p values for interaction were calculated for the subgroup analyses.
A Student’s t-test and non-parametric test (Mann-Whitney U test) were used to compare continuous variables (normally distributed and not normally distributed, respectively) between the groups, and Fisher’s exact test was used with binomial and categorical variables. All statistical analyses were performed on an intention-to-treat basis; as the frequency of crossover was low, no per-protocol analysis was performed. A p value of 0.05 was considered to indicate statistical significance. SPSS Statistics, V.23 (IBM), was used for all statistical analyses.
Results
The flow chart of the trial is shown in figure 1. Of the 205 eligible patients, 146 underwent randomisation; 70 were assigned to APM and 76 to placebo surgery. The baseline characteristics of the two groups were similar. On average, half of the participants in both groups reported mechanical symptoms preoperatively. There were 34 participants with a tear morphology defined as ‘unstable’ in the APM group and 41 in the placebo-surgery group (table 1). There were 24 patients who were eligible but declined to participate in the study. They were similar to those who underwent randomisation with respect to age, sex and body mass index at baseline, and all of them underwent arthroscopic partial meniscectomy. At the 24-month follow-up, two participants were lost to follow-up (one not responding to contact attempts and one deceased), both from the placebo-surgery group.

Participant enrolment flow diagram.
Baseline characteristics of the participants allocated to APM or placebo surgery. Values are numbers (percentages), means±SD or medians (ranges)
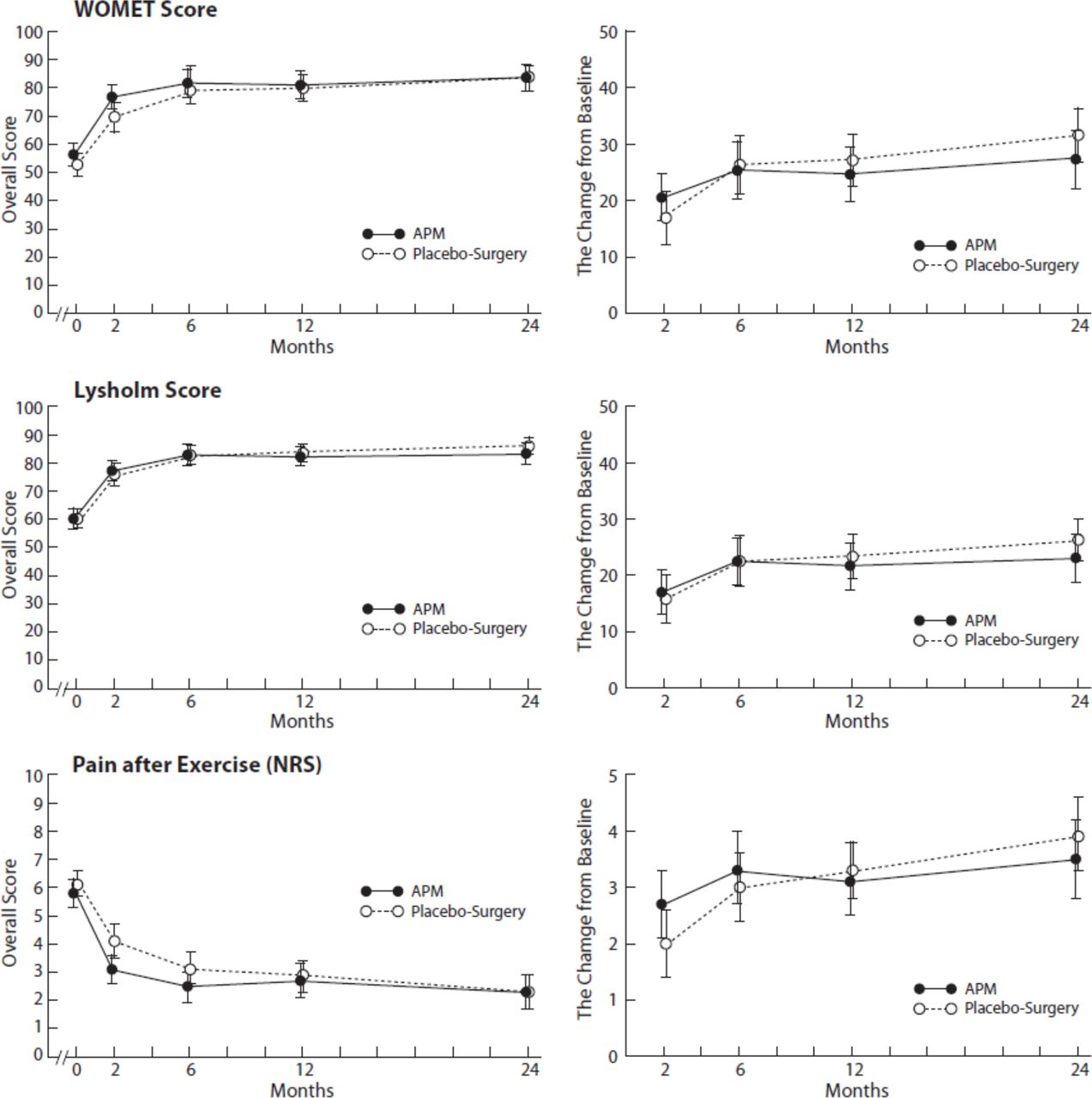
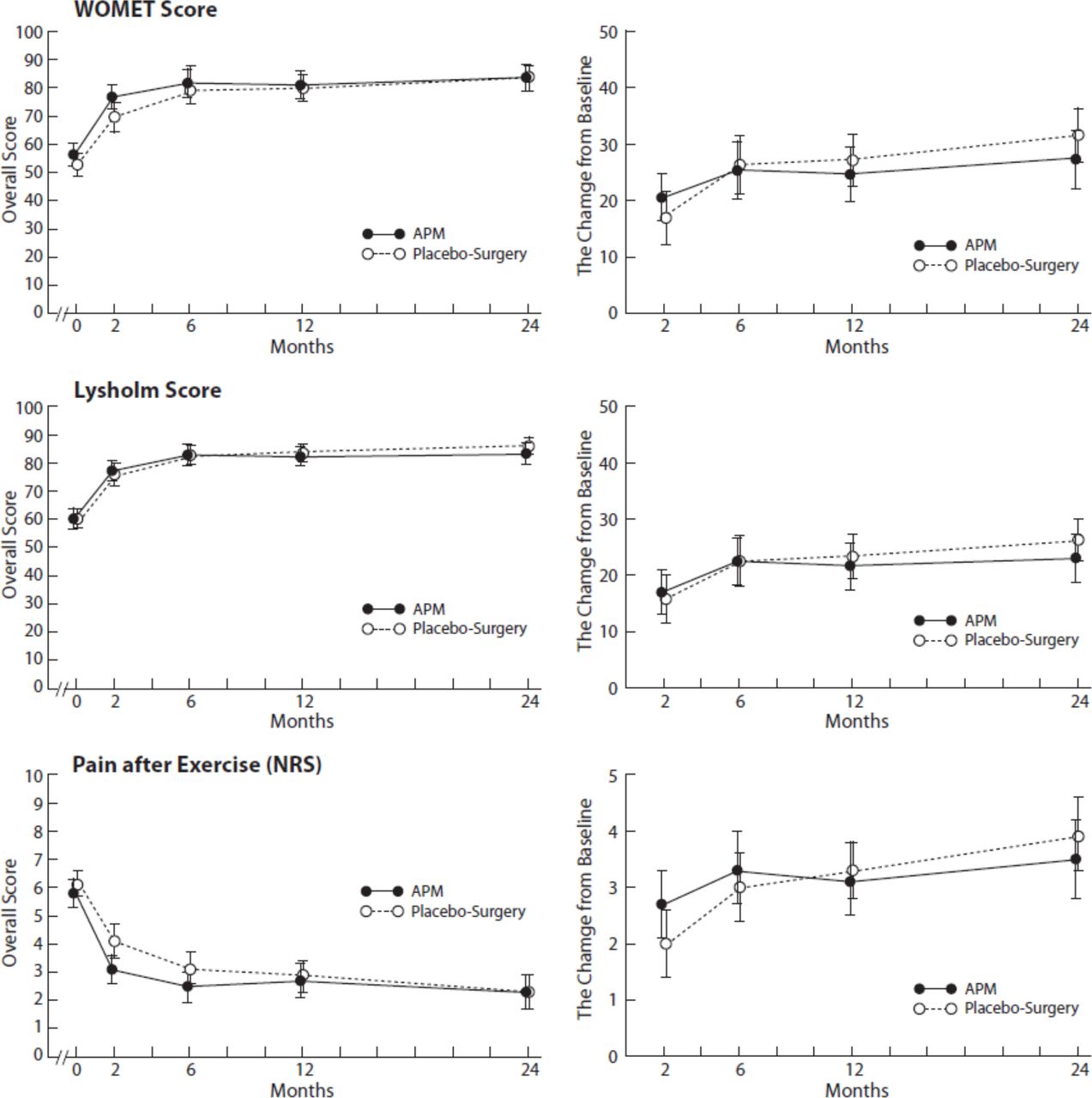
Both groups showed a marked improvement in all primary outcomes. However, the difference between the two groups did not reach statistical significance and 95% CIs excluded clinically relevant effect in any of the three primary outcomes over the course of the 24-month follow-up (table 2 and figure 2). Five participants (7.1%) in the APM group and seven (9.2%) in the placebo-surgery group complained of symptoms severe enough to result in the unblinding of the treatment-group allocation (p=0.767). Most of the participants, in both groups, were satisfied and reported improvement with no statistically significant difference between the two treatment groups. One participant in the APM group had a serious adverse event (a knee infection 4 months after the initial operation). No between-group difference was observed in the participants’ frequency in returning to normal activity level or in the frequency of mechanical symptoms. No statistically significant difference was found between the two groups in the meniscal tests during clinical examination either (table 3). The outcome of the patients who declined to participate (n=17, five lost to follow-up) were similar with those randomised, excluding the change in WOMET score (SD), which was greater for those declined (43.2±22.4) as compared with those randomised (29.5±21.1) with a between-group difference −13.7 (95% CI −25.6 to −2.9).
{kind=link}
{kind=link}
Mean values with 95% CIs in all three primary scores during the 24-month follow-up for both groups. APM, arthroscopic partial meniscectomy; NRS, numerical rating scale; WOMET, Western Ontario Meniscal Evaluation Tool.
Primary outcomes of the trial at 24-month follow-up. Values are means with 95% CIs
Secondary outcomes of the trial at 24-month follow-up. Values are numbers (percentage)
In the two subgroup analyses, one assessing the effect of preoperative mechanical symptoms and the other the effect of unstable tear on the treatment outcome, there was no difference in any of the primary or secondary outcomes between the APM and placebo-surgery groups (tables 4 and 5).
Primary and secondary outcomes at 24-month follow-up for the subgroup of patients with mechanical symptoms at baseline. Values are means with 95% CIs and numbers (percentage)
Primary and secondary outcomes at 24-month follow-up for the subgroup of patients with unstable meniscus tear. Values are means with 95% CIs and numbers (percentage)
Discussion
In this extension of the FIDELITY trial,29 we found no statistically significant difference between the APM and placebo surgery for symptomatic patients with a degenerative meniscus tear and no osteoarthritis (OA) in any of the used outcome measures over the course of 24-month follow-up. No evidence could be found to support the prevailing ideas that patients with presence of mechanical symptoms or certain meniscus tear characteristics or those who failed initial conservative treatment are more likely to benefit from APM.
The strengths of the FIDELITY trial have been elaborated in detail previously.29 34 In brief, our study was a multicentre, randomised, placebo-controlled efficacy trial with a 2-year follow-up. Controlling for the possible placebo effects of surgery requires that besides participants, all caregivers and outcome assessors are blinded to the treatment allocation.42 The use of multiple validated outcomes covering many different possible symptoms related to degenerative knee and meniscus tear can also be considered strength of this trial.
There are also some limitations worth discussing. We excluded patients with a truly ‘traumatic’ onset of symptoms, so our results are only directly applicable to patients with non-traumatic meniscus tears. Obviously, the concepts ‘degenerative’ or ‘traumatic’ in the context of meniscal injuries are very vague by nature. In this trial, all patients with sudden injuries related to their own voluntary muscle activities (such as kneeling, bending or kicking) and patients with a minor twisting of the knee were included. In essence, our criteria for labelling a tear as ‘traumatic’ required a more substantial event, such as falling from a chair, stairs or bicycle, or slipping on ice. In this context, to our knowledge, the only study specifically testing the assumption that meniscal tear outcomes would be any better for those with a traumatic onset of symptoms than for those without does not support such hypothesis.43 Moreover, a very recent study showed that patients with traumatic meniscal tears do not experience greater improvements in patient-reported outcomes after APM than patients with degenerative tears.44
The generalisability of the FIDELITY trial has been questioned.25 45 46 Although the design of the FIDELITY has been elaborated in detail previously,34 it is worth reasserting that it was designed as an efficacy trial to test the therapeutic potential of APM. Accordingly, we recruited a sample that potentially would have an ‘optimal response’ to APM (medial meniscus tear, no OA). Such patients are rare to find among ordinary patients with a degenerative meniscus tear. This explains the lengthy recruitment period (4 years) despite five high-volume centres, but given our finding of lack of efficacy, this methodological choice actually increases —rather than diminishes—the generalisability of our study.
Some have criticised the FIDELITY trial for recruiting patients with symptoms that were not attributable to a meniscal tear,25 yet our subjects’ eligibility was confirmed by both MRI and arthroscopy. APM is typically advocated for patients with knee symptoms in whom a tear is confirmed by MRI, particularly those without concomitant knee osteoarthritis.47 Increasing evidence, however, suggests that a degenerative meniscal tear may be an early sign of knee osteoarthritis rather than a separate clinical problem that causes symptoms.48–50 Moreover, specific meniscal pathology and other structural joint pathologies found at meniscal surgery were not associated with preoperative self-reported pain and function in patients with meniscal tears.51 We interpret our findings as supportive of the idea that degenerative meniscus tear does not cause specific symptoms even in knees without osteoarthritis.52
We are also aware of the limitations related to post hoc subgroup analyses53: the number of participants in our subgroups was small, the analyses were not planned a priori and there was no formal power calculation. However, as patients with mechanical symptoms and with unstable tear have been—and still are—widely suggested as the ideal subgroup to benefit from APM25 27 54–56 and the hypothesis is backed by a credible biological rationale, we felt that our analyses were of high clinical relevance.53
We set out to address a few apparent gaps in the existing evidence base regarding arthroscopic surgery for patients with knee pain and degenerative meniscus tear/knee disease. First, although a 24-month follow-up is a commonly held ‘minimal requirement’ for any procedure in orthopaedics, only three19 57 58 of the eight previous RCTs on this topic have followed-up patients longer than 12 months. Our 24-month data show that most of the improvement observed with both APM and placebo surgery was evident already at 6 months after surgery and the extended follow-up did not have an effect on our primary finding.29 Second, many authors and organisations advocate APM for patients ‘unresponsive to conservative treatment’,12–16 a strategy based on the previous unblinded trials.19–21 These trials showed that about 30% of participants initially allocated to conservative treatment have opted to crossover to surgery due to persisting symptoms. Although such behaviour is intuitively rational, it should be recalled that when patients are told of the possibility of surgical treatment but are allocated to conservative care, this so-called ‘failed opportunity’ may drive patients to seek surgery if symptoms persist.42 In our blinded trial, the frequency of unblinding of the treatment-group allocation due to persisting symptoms was clearly lower than in the previous—unblinded—studies and we found no difference between our two treatment groups. Our data thus highlight the vital importance of proper blinding of study participants in surgical RCTs. Considering the rationale to carry out APM on those having failed previous conservative treatment further, a recent study comparing exercise therapy to APM alone (with no postoperative rehabilitation) showed that although 19% of participants allocated to exercise therapy crossed over to surgery during the 2-year follow-up, APM did not result in any additional benefit for them.58
Another widely held assertion is that the presence of mechanical symptoms (sensation of knee catching or locking) represents a valid indication for arthroscopic surgery.25–27 59 This is premised on a rationale that mechanical symptoms are caused by a joint structure lodging between the gliding articular surfaces. Our recently published secondary analysis (1-year follow-up of this trial) showed that resection of a torn meniscus has no added benefit over placebo surgery in relieving knee catching or occasional locking.60 The findings of this 2-year extension corroborate our previous findings. The absence of an effect of APM on patients with mechanical symptoms is also supported by previous subgroup analyses of controlled trials21 61 and our own recent prospective cohort study of 900 consecutive patients undergoing APM.62 With respect to the present data, patients with a true locked knee (unable to extend their knee fully) were excluded from the FIDELITY and thus some caution may be warranted in the interpretation of our current findings. Finally, meniscus tear morphology is often asserted to explain the success of APM,17 28 63 64 but our data fail to support such notion.
In conclusion, the results of this randomised, placebo-controlled trial with 24 months follow-up show that APM provides no significant benefit over placebo surgery in patients with a degenerative meniscal tear and no knee osteoarthritis. These results support the evolving consensus that degenerative meniscus tear represents an (early) sign of knee osteoarthritis, rather than a clinical entity on its own, and accordingly, caution should be exercised in referring patients with knee pain and suspicion of a degenerative meniscal tear to MRI examination or APM, even after a failed attempt of conservative treatment.
Unanswered questions and future research
Arthroscopic surgery for knee pain in middle-aged and older patients is one of the most rigorously studied orthopaedic procedures. The evidence base shows very consistently that APM offers no benefit over conservative treatment or placebo surgery.65 Still, hundreds of thousands of procedures are performed worldwide each year. Given the mounting evidence, anyone still advocating APMs should promptly launch methodologically rigorous, practical, real-world trial(s) embedded in the flow of practice to prove that APM truly works in the asserted subgroups of patients.
Acknowledgments
We thank the patients for their participation. We would like to thank research nurses Marja-Liisa Sutinen, Sari Karesvuori, Pekka Karppi, Saara-Maija Hinkkanen, Johanna Koivistoinen, Kirsi Saarioja, Elina Jalava, Ina Fagerlund and Marketta Rautanen for their vital role in the implementation of the study.
References
Supplementary materials
Lay summary
Disclaimer : This is a summary of a scientific article written by a medical professional (“the Original Article”). The Summary is written to assist non medically trained readers to understand general points of the Original Article. It is supplied “as is” without any warranty. You should note that the Original Article (and Summary) may not be fully relevant nor accurate as medical science is constantly changing and errors can occur. It is therefore very important that readers not rely on the content in the Summary and consult their medical professionals for all aspects of their health care and only rely on the Summary if directed to do so by their medical professional. Please view our full Website Terms and Conditions.
Copyright © 2018 BMJ Publishing Group Ltd & European League Against Rheumatism. Medical professionals may print copies for their and their patients and students non commercial use. Other individuals may print a single copy for their personal, non commercial use. For other uses please contact our Rights and Licensing Team.
Footnotes
Contributors The Finnish Degenerative Meniscal Lesion Study (FIDELITY) trial (patient enrolment and execution of follow-up assessments in 2007–2015) is carried out by the FIDELITY Investigators. Conception and design: RS, MP, AM and TLNJ. Analysis and interpretation of the data: RS and TLNJ. Drafting of the article: RS and TLNJ. Critical revision of the article for important intellectual content and final approval: all authors. Ensuring the accuracy of the work: RS and TLNJ. Obtaining of funding: TLNJ. All authors had full access to all of the data in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This study was supported by the Jane and Aatos Erkko Foundation, the Sigrid Juselius Foundation, the State funding for university-level health research (Tampere and Helsinki University Hospitals), the Social Insurance Institution of Finland (KELA) and the Academy of Finland. Dr Sihvonen is supported also by The Finnish Medical Foundation and Orion-Pharmos Research Foundation. The funding sources had no role in in the collection, analysis and interpretation of data; in the writing of the report and in the decision to submit the article for publication.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Given that the informed consent forms of the Finnish Degenerative Meniscal Lesion Study trial did not include a provision for data sharing (trial launched in 2007), the full dataset cannot be shared due to a potential breach of the Finnish Personal Data Act. Scientists with a specific question regarding the trial data are encouraged to contact the corresponding author (TLNJ).