Article Text

Abstract
Background Poor prognostic factors (PPFs; e.g. elevated anti-citrullinated protein antibody/RF levels and erosions) are associated with higher disability and mortality in RA.1–2 In addition, high seropositivity or CRP/ESR levels are correlated with erosive disease.3
Objectives To evaluate if the presence of specific PPFs of seropositivity with erosions (PPF+) in patients (pts) with RA have an effect on treatment with abatacept (ABA) and anti-TNFs.
Methods This retrospective study was based on electronic medical record data. This database includes >6500 pts with RA from 50+ rheumatologists. At each visit, data on diagnosis, medications and test results were collected. A homunculus was used to record joint tenderness, swelling, deformity or decreased range of motion. Disease activity was measured by DAS28 (ESR/CRP), SDAI, CDAI, RAPID3 and Vectra DA blood tests. For this analysis, pts aged ≥18 yrs with an RA diagnosis from 1 Jan 2009 to 3 Mar 2016 were followed until lost to follow-up, death or end of study period. Date of first ABA/anti-TNF prescription was designated as index date, preceded by the baseline (BL) period. The ABA cohort comprised pts with a record of ABA in the study period, while the anti-TNF cohort comprised pts with a record of anti-TNF and no record of ABA in the study period. Primary outcome was change (Δ) in CDAI at 6 months (M); other outcomes were SDAI, DAS28 (CRP), pain, RAPID3 and Patient Global Assessment. Descriptive statistics were used for BL characteristics. Univariate and multivariate regression analyses were used to evaluate ΔCDAI. Subgroup analyses were conducted by line of therapy, after excluding switch pts.
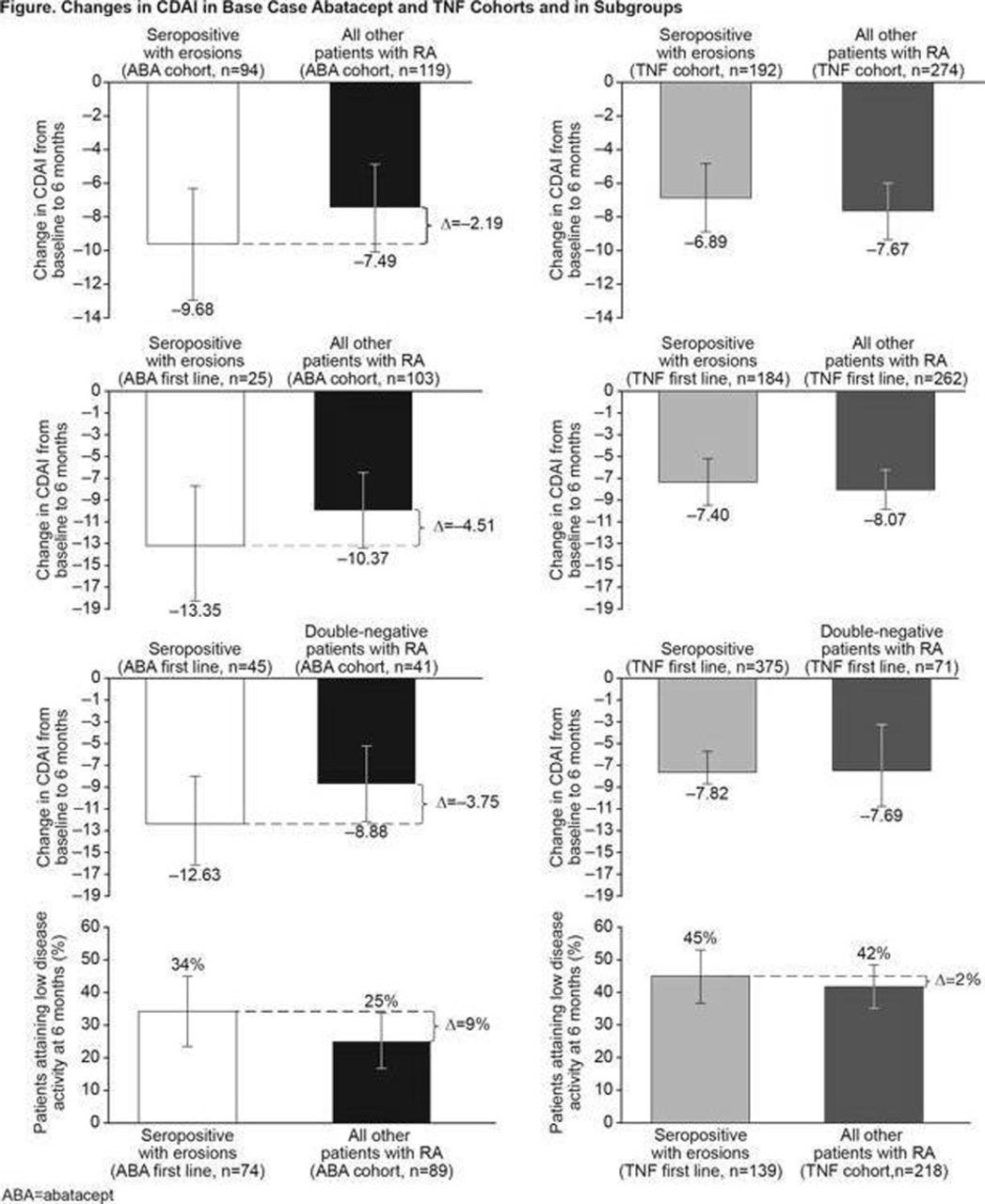
Results Overall, 3959 pts met inclusion criteria and 2045 had data on PPF; 344 and 814 pts received ABA and anti-TNF. Mean (SD) age of ABA pts was 60.3 (12.5) yrs and median (interquartile range; IQR) CDAI was 25.5 (18.1). Mean (SD) age of anti-TNF pts was 56.4 (13.3) yrs and median CDAI (IQR) was 19.8 (18.1). PPF+ pts treated with ABA (vs all other ABA pts) had a better CDAI outcome at 6M (–9.7 [16.1] vs –7.5 [14.4]). In sensitivity analyses, the difference persisted (–10.4 vs –8.4; Fig). PPF+ pts treated with ABA as first-line therapy (vs all other ABA pts) had a better CDAI outcome (–13.4 vs –10.3). Similar trends were not observed in the anti-TNF cohort (Fig). Adjusted mean (SE) ΔCDAI in PPF+ vs PPF– pts treated with ABA was –12.1 (2.01) vs –9.5 (0.79); covariates included in the model were age, sex and BL CDAI (p=0.24). During follow-up, more PPF+ pts treated with ABA changed from high/medium to LDA or remission vs all other pts (34% vs 25%), while this was not seen in anti-TNF pts (45 vs 42%).

{kind=link}
Conclusions Pts with RA treated with abatacept had higher disease activity at BL and a greater reduction in disease activity was observed in seropositive pts with RA and erosions compared with all other abatacept pts. Similar trends were not observed in anti-TNF pts. No direct comparisons between treatments were conducted in these cohorts.
References
Humphreys JH, et al. Arthritis Res Ther 2014;16:483.
Quinn MA, et al. Rheumatology (Oxford) 2006;45:478–80.
Dixey J, et al. J Rheumatol Suppl 2004;69:48–54.
References
Disclosure of Interest E. Alemao Shareholder of: Bristol-Myers Squibb, Employee of: Bristol-Myers Squibb, K. Knapp Employee of: Discus Analytics, V. Anupindi: None declared, S. Annamalai: None declared, G. Craig Shareholder of: Discus Analytics, Grant/research support from: Bristol-Myers Squibb, Consultant for: Premera Blue Cross/Blue Shield of Washington and Alaska, Employee of: Arthritis Northwest, Speakers bureau: Bristol-Myers Squibb, UCB, Genentech, Celgene, Novartis