Article Text

Abstract
Objectives To analyse the impact of active and passive smoking and intestinal transit disorders on the risk of incident RA
Methods This study is based on the French E3N cohort (“Etude Epidémiologique auprès de femmes de l'Education Nationale”), which included 98,995 women volunteers born between 1925 and 1950 and prospectively followed since 1990. Eleven self-administered questionnaires were sent to the participants between 1990 and 2014 to collect medical, demographic, environmental and hormonal data and dietary habits. The diagnosis of RA was collected on 2 successive questionnaires. Cases were considered certain if having declared RA and had taken a RA specific medication (methotrexate, leflunomide or biologic) since 2004 (period from which drug reimbursement data was available). Only incident and certain cases were included. Women were excluded if they had an inflammatory bowel disease and/or no information on their smoking status. Passive smoking was assessed by the following question: “When you were children, did you stay in a smoky room?”. Patients were considered exposed if the answer was “yes, a few hours, or yes, several hours a day”. The usual intestinal transit, reported by women prior to RA diagnosis (on average 10 years), were classified as normal transit, chronic diarrhoea, chronic constipation, and alternation between diarrhoea and constipation.
The risk of incident RA was estimated using an age-adjusted Cox model that considers smoking status as a time-dependent variable.
Results 70598 women from the E3N study were included in the study. A total of 1239 patients reported an incidental RA, of which 350 cases were included in the study (and 280 in the analysis of intestinal transit disorders). Non-ascertained cases were excluded form the analyses. The age at inclusion in the study was 49.0 years (± 6.4). The mean duration of follow-up was 21.2 (± 1.3) years.
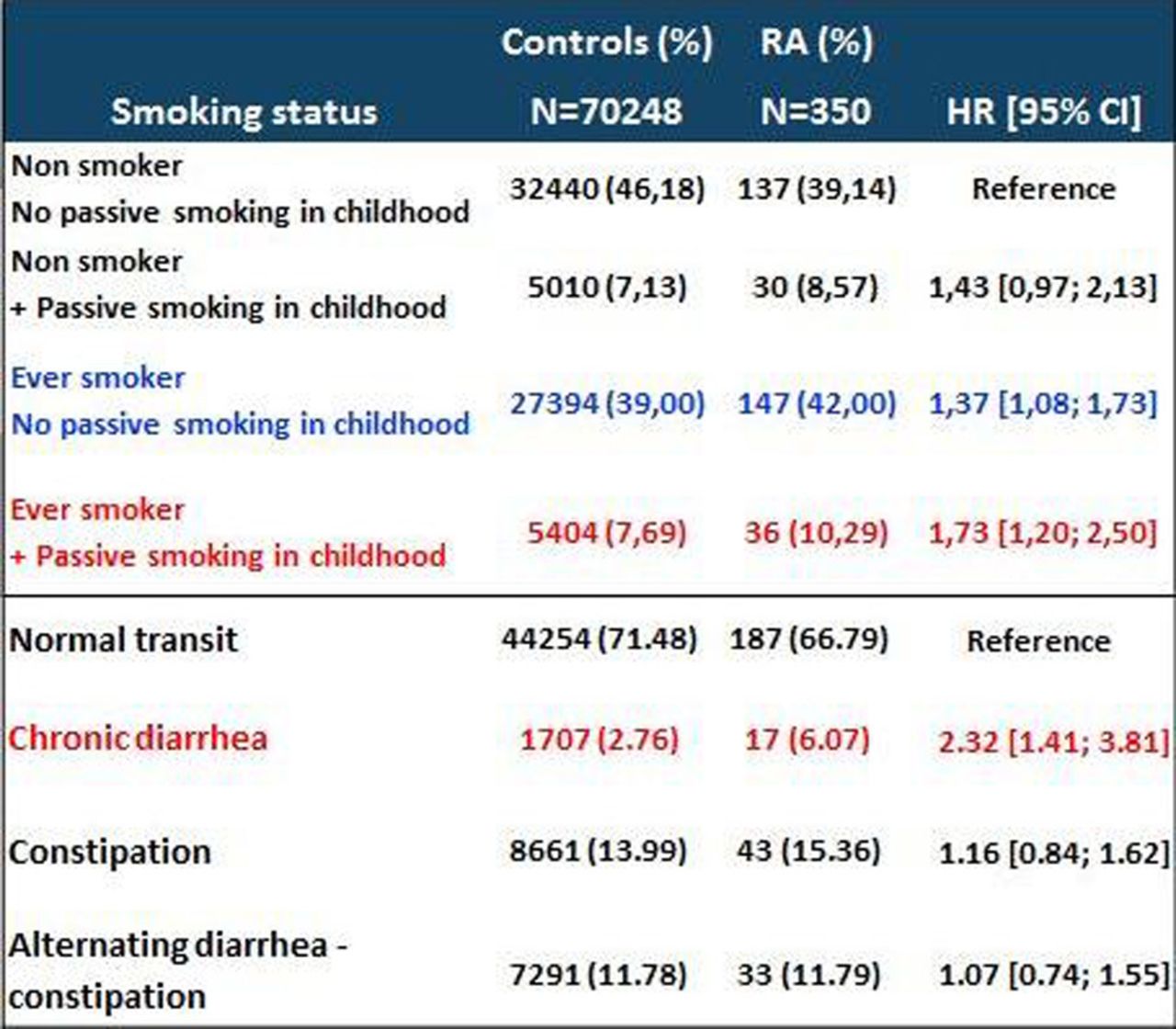
Passive smoking exposure during childhood increased the association between the RA risk active and adult active smoking. In ever smokers who had childhood passive exposure to smoke, the HR was 1.73 [1.20; 2.50] as compared with non-smokers who were not exposed during childhood, while it was 1.37 [1.08; 1.73] in active smokers who were not exposed during childhood.
A history of chronic diarrhea was associated with increased RA risk (HR =2.32 [1.41, 3.81]), while chronic constipation or alternation between diarrhoea and constipation did not.
{kind=link}
Conclusions This study confirms the link between active smoking and the risk of RA. It suggests for the first time that in smokers, exposure to tobacco early in life, through passive smoking in childhood significantly increases this risk. Our study highlights the importance of avoiding any tobacco environment in children, especially in those with a family history of RA. Also, it shows for the first time an association between a history of chronic diarrhoea and the risk of developing RA. The association supports the hypothesis of dysbiosis (microbiota abnormality) as a risk factor for the emergence of autoimmunity. These data perfectly fit with the preclinical scheme of RA where an external event occurs at an early stage to promote emergence of auto-immunity, followed years after by clinical RA.
Disclosure of Interest None declared