Article Text

Abstract
Objectives Weight loss is commonly recommended for gout, but the magnitude of the effect has not been evaluated in a systematic review. The aim of this systematic review was to determine benefits and harms associated with weight loss in overweight and obese patients with gout.
Methods We searched six databases for longitudinal studies, reporting the effect of weight loss in overweight/obese gout patients. Risk of bias was assessed using the tool Risk of Bias in Non-Randomised Studies of Interventions. The quality of evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation.
Results From 3991 potentially eligible studies, 10 were included (including one randomised trial). Interventions included diet with/without physical activity, bariatric surgery, diuretics, metformin or no intervention. Mean weight losses ranged from 3 kg to 34 kg. Clinical heterogeneity in study characteristics precluded meta-analysis. The effect on serum uric acid (sUA) ranged from −168 to 30 μmol/L, and 0%–60% patients achieving sUA target (<360 μmol/L). Six out of eight studies (75%) showed beneficial effects on gout attacks. Two studies indicated dose–response relationship for sUA, achieving sUA target and gout attacks. At short term, temporary increased sUA and gout attacks tended to occur after bariatric surgery.
Conclusions The available evidence is in favour of weight loss for overweight/obese gout patients, with low, moderate and low quality of evidence for effects on sUA, achieving sUA target and gout attacks, respectively. At short term, unfavourable effects may occur. Since the current evidence consists of a few studies (mostly observational) of low methodological quality, there is an urgent need to initiate rigorous prospective studies (preferably randomised controlled trials).
Systematic review registration PROSPERO, CRD42016037937.
- systematic review
- hyperuricemia
- serum uric acid
- weight reduction
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Gout is a common form of inflammatory arthritis,1 2 with an age-standardised global prevalence of 0.08% and is higher in developed countries.3 Gout is a crystal-deposition disease resulting from chronic elevation of serum uric acid (sUA) above the saturation point for monosodium urate (MSU).4–7 Initial presentation is severely painful episodes of peripheral joint synovitis (acute ‘attacks’), but joint damage and subcutaneous tophus deposition may develop.8 The general management principle is to reduce sUA levels, allowing MSU crystals to dissolve, leading to the elimination of acute attacks, disappearance of tophi and possibly cure of the disease.9–11
Body mass index (BMI) is strongly positively correlated to sUA levels,12 13 and weight loss is a commonly recommended treatment for gout.14–23 Furthermore, weight loss from bariatric surgery is associated with reduced incidence of hyperuricaemia and gout.24 The mechanism by which weight loss can lower sUA levels is poorly understood. Some suggest that improved insulin resistance results in less insulin-enhanced reabsorption of organic anions such as urate,2 and a study demonstrated decreased sUA in overweight patients receiving either weight loss from low-energy diet or an insulin-sensitising agent.25 However, a study of severe obese patients receiving bariatric surgery found no association between reduced sUA levels and improved insulin resistance,26 making a relationship questionable.
Guidelines recommending weight loss for gout patients14–23 are based on evidence from only few clinical studies,27 28 one population-based study29 and indirect evidence from studies on non-gout subjects. The evidence for effectiveness in clinical studies has to our knowledge not previously been evaluated in a systematic review. Therefore, the primary objective of this systematic review was to determine the benefits and harms associated with weight loss in overweight and obese individuals with gout. Furthermore, we had an explicit focus on the weight loss intervention (including magnitude and intensity) to see whether a dose–response relationship exists at the study (ie, group) level.
Methods
Protocol
A protocol adhering to the Preferred Reporting Items for Systematic review and Meta-Analysis Protocols 2015 statement30 was registered online (PROSPERO: CRD42016037937) and published on www.parkerinst.dk.
Search strategy
We searched four bibliographic databases on 26 April 2016; MEDLINE via Ovid from 1946, EMBASE via Ovid from 1974, Web of Science via Web of Knowledge from 1900, Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library), as well as ClinicalTrials.gov and WHO International Clinical Trial Registry Platform portal (search strategy presented: online supplementary text S1). We screened reference lists of relevant articles, as well as the American College of Rheumatology (ACR) and European League Against Rheumatism conference abstracts from 2014 and 2015, the ACR conference abstracts from 2016 and content experts were asked if they were aware of any other relevant studies.
Supplementary file 4
Study selection
Anticipating only few randomised controlled trials (RCTs), we also included longitudinal observational studies (non-randomised studies) that quantitatively estimated the effect following weight loss. Studies needed to include ≥10 adult and overweight/obese patients (author described or BMI ≥25 kg/m231) with diagnosed gout (author described or meeting the 1977 ACR criteria for gout32). Eligible interventions included those where a weight reduction was reported explicitly, whether intentional or unintentional. The weight reduction was required to be the only difference in terms of intervention from the defined control group. Two reviewers (SMN supported by EMB) assessed the records. Disagreements were resolved by consensus or by discussion with a third reviewer (RC).
Data extraction and management
Two reviewers (SMN supported by RC) extracted the data. Prespecified outcomes included essential outcome domains for chronic gout33 34: (1) joint pain; (2) tophus/tophi; (3) physical function; (4) health-related quality of life (HRQoL); (5) sUA change; (6) Achieving sUA target (ie, sUA reduction to <360 μmol/L (6 mg/dL)); (7) serious adverse events (SAEs, defined as adverse events that are fatal, life-threatening or require hospitalisation); (8) withdrawals due to adverse events (WDdtAEs); (9) patient global assessment; (10) wody weight change; and (11) gout attacks (any measure).
Assessment of risk of bias in included studies (internal validity)
Two reviewers (SMN supported by RC) assessed risk of bias using the tool Risk of Bias In Non-Randomised Studies of Interventions35 36 for evaluation of the risk of bias in non-randomised studies comparing health effects of two or more interventions. Post hoc, we decided to also use this tool for assessing studies with only one study group, by assuming that a virtual control group not receiving any intervention and experiencing no effect on any outcome was available, and for assessing RCTs, making comparisons possible. We resolved disagreements by discussion.
Important confounders of interest and cointerventions possibly affecting the effect of weight loss were not specified at protocol stage but prior to the risk of bias assessment (online supplementary text S2).
Supplementary file 5
Reporting bias in individual studies was further investigated by comparing the constructed outcome reporting matrix,37 with the protocols (if available).
Statistical analyses and evidence synthesis
None of our planned meta-analyses were conducted due to indisputable clinical heterogeneity in study characteristics (PICOTs). Instead it was decided post hoc that data for each study would be presented for all time points in a summary of findings table and the latest time point as changes from baseline would be summarised for each study in a summary of findings and GRADE evidence profile table. Based on the tables, we qualitatively considered the impact of follow-up time, that is, short-term (<3 months), medium (3–12 months) and long-term (>12 months), acute versus chronic gout, presence versus absence of concurrent urate-lowering medication use, presence versus absence of tophi, the dose–response phenomena of weight loss in magnitude and intensity (ie, magnitude over time) and the impact of bias. A graph showing the relationship between weight loss and sUA was constructed post hoc.
Dealing with missing data
Where data were missing or incomplete, we searched for information from the study authors and from additional records for the study. No imputations were carried out for patients lost at follow-up. Missing body weights were estimated from BMI, assuming a height of 1.70 m. Missing SDs were calculated from other statistics such as standard errors, or estimated from other studies investigating gout patients; for sUA, we used a SD for change from baseline of 137 μmol/L.
Assessing the quality of the evidence
We assessed the quality of the evidence with the GRADE approach,38 starting at low quality of evidence, since the evidence was primarily based on observational studies and subsequently down-rated or up-rated the evidence.
Results
Study selection
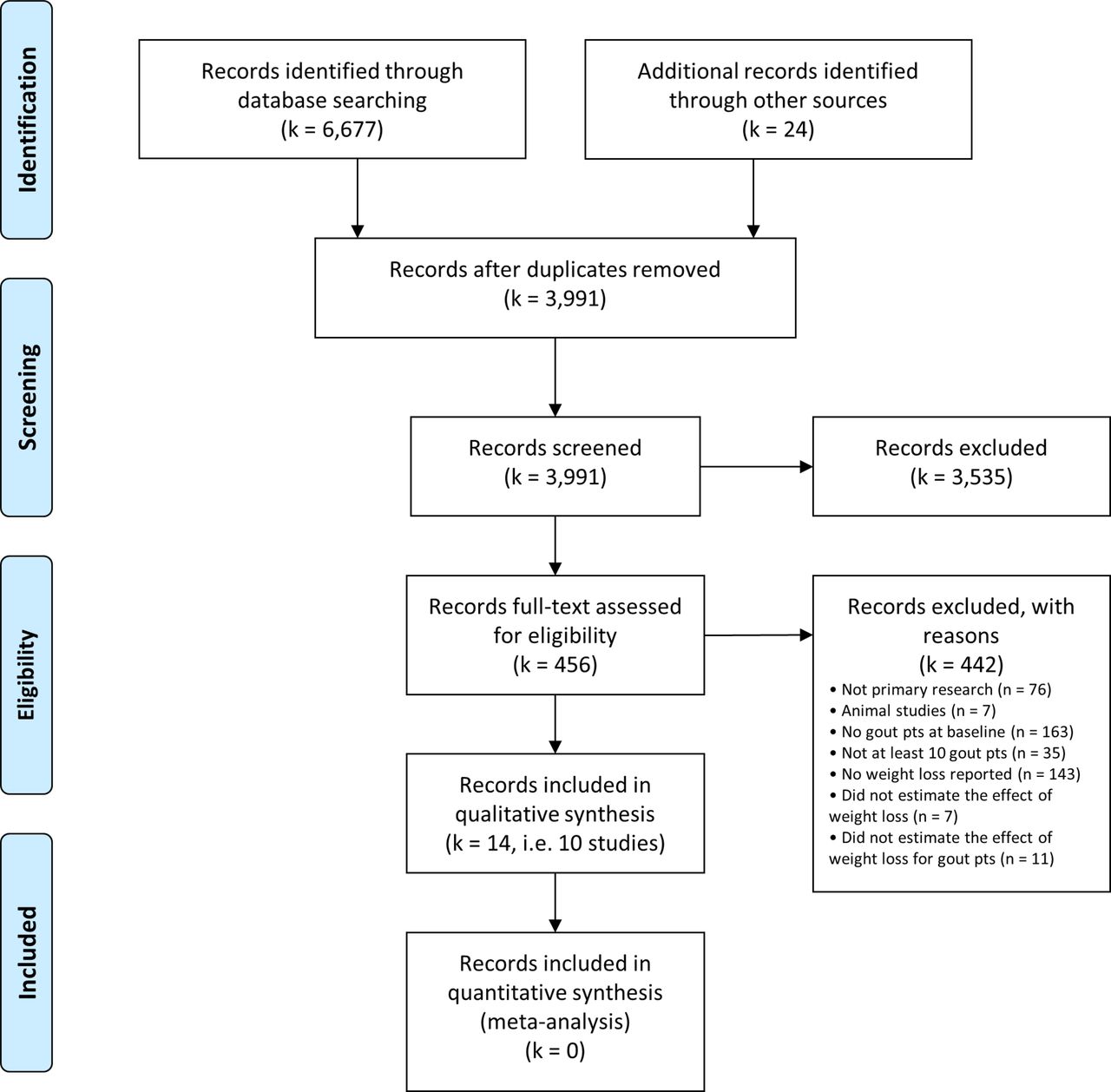
We identified 3991 records after removal of duplicates, forwarding 456 for full-text assessments after screening (figure 1). After excluding 442 records (see online supplementary text S3), we identified 14 records describing 10 studies for inclusion in the systematic review.27–29 39–49
Supplementary file 6

PRISMA flow diagram. Modified from Moher et al.75 pts, patients.
During the study selection and data extraction, authors of 18 studies27–29 40 43–46 49–58 were contacted; three responded27 44 45 and provided additional information, including unpublished data for Perez-Ruiz et al.45
Study characteristics
The studies were comprised of one RCT49 and nine non-randomised studies (table 1). Gout patients were a subgroup in three of the studies,27 29 44 of which one study initially only included non-gout patients but did a subanalysis on recurrent gout attacks for those who developed gout during follow-up.44 The studies included between 12 and 408 gout patients, including 0%–75% females. The average age and BMI ranged from 49 to 63.3 years, and 26.0 to 49.6 kg/m2, respectively. Case definitions of gout included the use of the 1977 ACR criteria in one study,42 diagnosis confirmed by detecting crystals in three studies,28 40 45 asking ‘Have you been told by your physician that you have gout?’ in two studies,29 44 medical history and documentation of previous gout attacks in one study,43 documented episode(s) or evidence of medication use in one study,46 or not specified in two studies41 49 (online supplementary table S1). Comorbidities selected in the studies, besides overweight, included type 2 diabetes,27 hypertension41 and a high cardiovascular risk profile.29 44
Supplementary file 1
Characteristics of the included studies
Interventions included intentional weight loss from dietary changes with or without increased physical activity,27 28 bariatric surgery27 43 46 and unintentional weight loss from high protein diet,49 diuretics41 and metformin.40 Three studies29 44 45 stratified according to weight or BMI reduction, using no reduction as control. Four studies had no control group.27 28 40 43 Follow-up ranged from 4 weeks to 7 years, and a mean weight loss of 3–34 kg at latest follow-up was reported.
Effect of weight loss
No data were available for joint pain, HRQoL or patient global assessment (outcome matrix: online supplementary table S2). One study45 provided data on tophi, reporting none for both groups at baseline and follow-up, and one study27 provided data on physical function measured by Short Form-36 physical functioning domain, reporting diminished function with the values 43.3 (SD 21.8), 24.6 (SD 28.2), 10.8 (SD 12.8) at baseline, 6 months and 1.5 years, respectively. One study40 reported four WDdtAEs from metformin, and one study27 did not report any SAEs in gout patients. On sUA, achieving sUA target and gout attacks, eight, five, and eight studies provided data, respectively (table 2).
Supplementary file 2
Study findings
The effect on mean sUA ranged from −168 μmol/L to 30 μmol/L (−2.8 mg/dL to 0.5 mg/dL) at latest follow-up (table 3). Studies with the largest (and fastest) weight loss showed in general the largest decrease (figure 2).27 28 46 Furthermore, a dose–response relationship was shown by Zhu et al29 with a weight loss of ≥10 kg being associated with a change in sUA of −37 μmol/L. It should be noted that non-gout and non-overweight patients were included in their analysis as well. At short term, Dalbeth et al (part 2)27 reported an immediate postoperative mean sUA of 510 (SD 130) μmol/L, that is, an increase of 70 μmol/L from bariatric surgery, and at latest follow-up, sUA had dropped to 330 (SD 90) μmol/L. In that period, three out of seven patients terminated urate-lowering medication, that is, the decrease may truly be larger. Three studies showed no effect on sUA; Perez-Ruiz et al45 and Dalbeth et al (part 1),27 both with a concurrent decrease in urate-lowering medication, and Brandstetter et al,41 where the weight loss may partly be due to diuretics and hence truly lower. Barskova et al40 showed a decrease in sUA from a weight loss of only 3 kg. However, the use of metformin can have affected the results.
Summary of findings and GRADE evidence profile
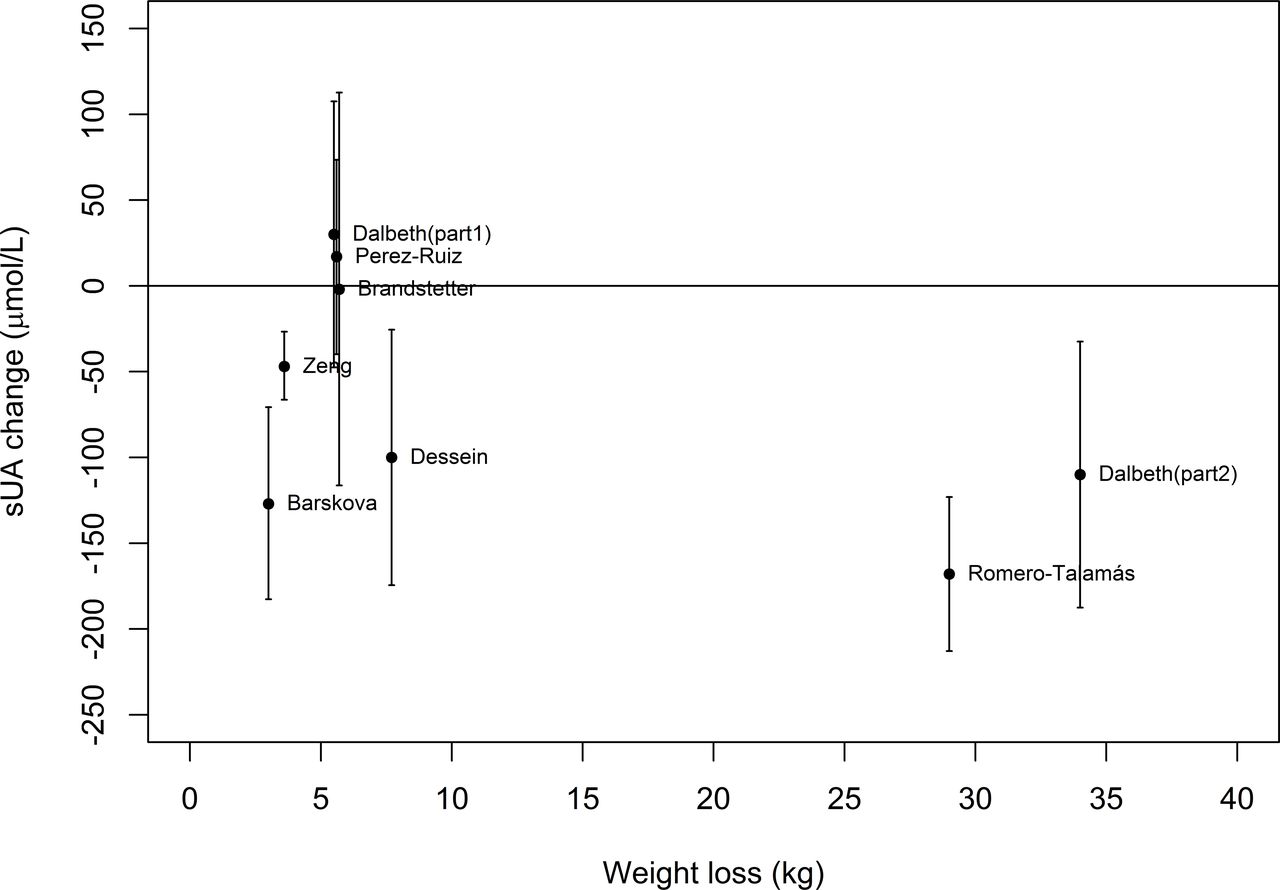
Relationship between weight loss and serum uric acid at latest follow-up. Estimates are shown with 95% confidence intervals. sUA, serum uric acid.
The proportion achieving sUA target (<360 μmol/L) ranged from 0% to 60% reduction in patients with raised sUA. Furthermore, a dose–response relationship was shown by Zhu et al29 with approximately three times higher odds of achieving sUA target with loss of ≥10 kg body weight during 7 years compared with not losing weight. It should be noted that non-overweight gout patients were included in their analysis as well. The 0% and 1% reduction in patients with raised sUA reported by Dalbeth et al (part 1)27 and Perez-Ruiz et al,45 respectively, are consistent with no change in sUA. Furthermore, achieving sUA target reported by Dessein et al28 may be overestimated due to using a higher sUA cut-off of 510 μmol/L.
All studies, except two,27 43 with data on gout attacks, showed a beneficial effect, and Dessein et al28 reported 71% fewer attacks. Furthermore, a dose–response relationship was shown by Nguyen et al.44 It should be noted that non-overweight patients were included in their analysis as well. Dalbeth et al (part 2)27 reported an increase from zero patients experiencing ≥1 attack during 6 months to three patients during 12 months. This is possibly due to including the immediate postoperative phase where attacks could be a consequence of the increased sUA. Likewise, Romero-Talamás et al46 report a possible increase from 24% experiencing ≥1 attack during 1 year at baseline to 18% during 1 month at 1-month follow-up, and a subsequently decrease to 8% during 1 year at last follow-up.
Only one study40 included patients with tophi at baseline, therefore the impact on tophi could not be assessed.
Risk of bias assessment
The most frequent risk of bias was ‘Bias due to confounding’, with four studies rated critical due to studying one group without adjustment for confounders.28 40 42 43 Five studies were rated serious (figure 3), and only the RCT49 was rated low risk of bias. All studies were rated serious risk for ‘Bias due to departures from intended interventions’ (see possible confounders and cointerventions in online supplementary table S3). Reporting bias was suspected for two studies reporting change in BMI instead of change in weight.40 46 Protocols were only found for two substudies29 44 of one main study39 47 and three studies reported no published protocol.27 44 45
Supplementary file 3

{kind=link}
{kind=link}
{kind=link}
Risk of bias summary figure. Similar outcomes has been put together in the figure but has been assessed separately. *Multiple publications existed. A primary publication was chosen. †Potentially serious risk of bias, since physical function was not reported in the article, but assessed low since data were provided from the author through email contact. BMI, body mass index; sUA, serum uric acid.
Quality of the evidence using GRADE
For a beneficial effect of weight loss at medium-term/long-term follow-up, we evaluated the overall quality of evidence to be low for sUA, moderate for achieving sUA target and low for gout attacks.
Discussion
Overall, we found low to moderate quality of evidence for beneficial effects of weight loss for overweight gout patients in terms of sUA, achieving sUA target and gout attacks. No or few data were available on our remaining prespecified outcomes. We did not find evidence for the optimal magnitude and intensity of weight loss. However, our data suggest that a weight loss of >7 kg and/or >2 kg per week from either surgery or diet results in a beneficial effect on sUA at medium-term/long-term follow-up based on three studies27 28 46 and that weight loss of >3.5 kg showed beneficial effects on gout attacks at medium-term/long-term follow-up based on six studies.27 28 40 45 46 49 However, with the present quality of evidence, further research may change these findings. WDdtAEs and SAEs were poorly reported. At short term, weight loss from bariatric surgery showed temporarily increased sUA levels and gout attacks, that is, a harmful effect, in the immediate postoperative period based on two studies.27 46
It is well known that there is a higher risk of gout attacks during the first months of urate-lowering therapy, postsurgery and starvation.59 One hypothesis is that dramatic changes in sUA, rather than absolute level, triggers gout attacks.60 In line with this, a study61 comparing gout patients experiencing postoperative gout attacks with those who did not, find that the first group had higher presurgical sUA and a more rapid and larger decrease in sUA 3 days after surgery. Dalbeth et al27 reported a drastic increase 2 weeks after surgery, which they suggested was due to renal dysfunction associated with major surgery, or metabolic effects from fasting or rapid weight loss (catabolic state), and they report one case of postoperative gout attack together with severe hyperuricaemia. Other factors increasing sUA levels are fasting,62–64 dehydration65 and tissue hypoxia.66 Fasting-associated increase in sUA is likely due to tissue breakdown.67 68 In line with this, daytime fasting during Ramadan, without weight loss, compared with non-fasting did not increase sUA or gout attacks in gout patients.69
Increased sUA seems to be related to decreased estimated glomerular filtration rate (eGFR).70 71 This is probably related to sUA affecting blood pressure,72 which may be caused by increased vascular stiffness.73 74 Reducing sUA may therefore have beneficial effect on susceptibility towards cardiovascular disease and diminished renal function.
In our study, we lacked evidence for many prespecified outcomes important to patients. Serum uric acid was among the most frequently reported outcomes and is recommended as a treatment target,15–19 21–23 since elevated sUA is considered to cause the disease. Gout attacks in this study is not well defined and was reported in various ways and over various follow-up times. Therefore, stating fewer gout attacks following weight loss is not very specific and not necessarily assessable in smaller study sizes, or when attacks were not systematically assessed. At least three studies27 43 45 did not point at reduced frequency of attacks, of which Friedman et al43 did not report any baseline and Perez-Ruiz et al45 did show less increase compared with control. Other studies can mask increasing number of attacks by reporting number of patients experiencing ≥1 attack over various follow-ups. Therefore, one could consider rating the evidence for gout attacks further down for indirectness.
Limitations of our methods include no independent double study selection, data extraction or risk of bias assessment. A limitation of investigating weight loss per se is that weight loss can be a consequence of many different interventions, that is, cointerventions, or conditions. Hence, it was impossible to ensure the weight reduction to be the only difference in terms of intervention from the comparison group, resulting in the inclusion of a wide variety of study settings. This is also observed as for which variables have been measured longitudinally. The included cohort studies stratifying according to weight loss may include unintentional weight loss for example, from illness, which is not relevant as intervention. Adding this to the fact that the majority of our included studies did not have a comparison group introducing non-controllable confounding, we cannot be sure that weight loss is accountable for all the effects observed. As a result, the implementation of weight loss intervention in clinical practice cannot be specified from the included studies. Taking the limitations of the available evidence into account, one may suggest, in order to address the effect of weight loss on sUA, that there currently is a need to perform a systematic review and meta-analysis of data not only for gout patients.
In conclusion, the available evidence is in favour of weight loss for overweight gout patients at medium-term/long-term follow-up on sUA, achieving sUA target and gout attacks. However, the evidence is of low, moderate and low quality, respectively. Harms were poorly reported. However, gout attacks might occur at short term when initiating treatment. We believe that there is an urgent need to initiate rigorous prospective studies (preferably RCTs) to provide more trustworthy estimates of gout-related benefits and harms including the effect on joint pain, tophi, physical function, HRQoL, adverse events and patient global assessment. Future research should aim at identifying the optimal magnitude and intensity of weight loss, the preferred method of weight loss, including prevention of flare, which cointerventions result in a better effect, and which gout patients will benefit the most, for example, grouped according to type (and possibly severity) of overweight and comorbidities.
Acknowledgments
The authors would like to thank the Copenhagen University Library, Frederiksberg for their hard work in retrieving full texts from all over the world. In particular, we want to thank the librarian, Karen Bendix Larsen. We would also like to thank for assistance with translation of articles in Russian, Chinese and Bulgarian from Natalia Manilo, MD, Department of Rheumatology, Rigshospitalet Glostrup and Frederiksberg, Copenhagen, Denmark; Tao Ma, MD, PhD, Laboratory of Genomics and Molecular Biomedicine, Department of Biology, University of Copenhagen, Copenhagen, Denmark; and Nora Vladimirova, MD, Department of Rheumatology, Rigshospitalet Glostrup and Frederiksberg, Copenhagen, Denmark, respectively. Furthermore, we would like to thank professor Nicola Dalbeth, Department of Rheumatology, Counties Manukau District Health Board, Auckland, New Zealand, who responded to our data and information requests.
References
Footnotes
Contributors Study concept and design: SMN, EMB, LEK and RC. Drafting of the manuscript: SMN, EMB and RC. Search strategy: EMB and SMN. Study selection, data extraction, bias assessment and synthesis: SMN, EMB and RC. Critical revision of the manuscript for important intellectual content and final approval before submission: All authors. Obtained funding: HB, LEK and RC.
Funding The Parker Institute, Bispebjerg and Frederiksberg Hospital is supported by a core grant from the Oak Foundation (OCAY-13-309). This research received a specific grant from the will of Mrs Elise Fredriksen; the Oak Foundation had no role in study design or writing of this manuscript.
Competing interests This study had no financial competing interests. The Parker Institute is grateful for the financial support received from public and private foundations, companies and private individuals over the years. The Oak Foundation is a group of philanthropic organisations that, since its establishment in 1983, has given grants to not-for-profit organisations around the world.
Patient consent No patients were directly included in the study (only in the primary studies of this review).
Provenance and peer review Not commissioned; externally peer reviewed.