Article Text

Abstract
Patients with rheumatoid arthritis (RA) and other inflammatory joint disorders (IJD) have increased cardiovascular disease (CVD) risk compared with the general population. In 2009, the European League Against Rheumatism (EULAR) taskforce recommended screening, identification of CVD risk factors and CVD risk management largely based on expert opinion. In view of substantial new evidence, an update was conducted with the aim of producing CVD risk management recommendations for patients with IJD that now incorporates an increasing evidence base. A multidisciplinary steering committee (representing 13 European countries) comprised 26 members including patient representatives, rheumatologists, cardiologists, internists, epidemiologists, a health professional and fellows. Systematic literature searches were performed and evidence was categorised according to standard guidelines. The evidence was discussed and summarised by the experts in the course of a consensus finding and voting process. Three overarching principles were defined. First, there is a higher risk for CVD in patients with RA, and this may also apply to ankylosing spondylitis and psoriatic arthritis. Second, the rheumatologist is responsible for CVD risk management in patients with IJD. Third, the use of non-steroidal anti-inflammatory drugs and corticosteroids should be in accordance with treatment-specific recommendations from EULAR and Assessment of Spondyloarthritis International Society. Ten recommendations were defined, of which one is new and six were changed compared with the 2009 recommendations. Each designated an appropriate evidence support level. The present update extends on the evidence that CVD risk in the whole spectrum of IJD is increased. This underscores the need for CVD risk management in these patients. These recommendations are defined to provide assistance in CVD risk management in IJD, based on expert opinion and scientific evidence.
- Cardiovascular Disease
- Rheumatoid Arthritis
- Ankylosing Spondylitis
- Psoriatic Arthritis
Statistics from Altmetric.com
Introduction
Cardiovascular disease (CVD) risk in patients with rheumatoid arthritis (RA) and other inflammatory joint disorders (IJD), in particular ankylosing spondylitis (AS) and psoriatic arthritis (PsA), is substantially elevated compared with the general population. For RA, the magnitude of this excess risk appears comparable to that reported for patients with diabetes mellitus,1–3 necessitating aggressive and targeted CVD risk management. In 2009, the European League Against Rheumatism (EULAR) task force was convened to critically appraise existing evidence on CVD risk in patients with IJD. This EULAR task force formulated 10 recommendations for the screening and identification of CVD risk factors and the implementation of CVD risk management in IJD (see online supplementary file 1).4 In view of substantial new evidence, an update of the CVD risk management recommendations was performed.
supplementary file
In general, CVD risk management involves the determination of a cardiovascular risk profile of an individual patient by using values including gender, age, smoking status, blood pressure, lipid values and diabetes mellitus status. These variables are used in risk prediction algorithms such as Framingham5 and the Systematic Coronary Risk Evaluation (SCORE)6 to calculate a 10-year risk of CVD events. When this CVD risk exceeds a certain value, that is, a 10-year risk of 10% for a fatal or non-fatal CVD event (Framingham) or a 10-year risk of 5% for fatal CVD events (SCORE), lifestyle changes and treatment with lipid-lowering agents is recommended. The importance of a healthy lifestyle is emphasised for all persons, including patients at low and intermediate cardiovascular risk. Additionally, the European Society of Cardiology (ESC) guideline on CVD prevention in clinical practice also recommends CVD risk stratification for patients with hypertension.7 The initiation of antihypertensives depends on the grade of hypertension and total cardiovascular risk. Drug treatment is recommended for patients with grade 3 hypertension, but also grade 2 and grade 1 hypertension with a high CVD risk.7 Validated RA-specific CVD risk prediction models with a proven superiority over general population CVD risk prediction algorithms are currently lacking.7 Furthermore, the existing general population risk prediction models that aid the identification of patients who would benefit from primary prevention of CVD have been shown to inaccurately estimate the CVD risk in RA.8 ,9 Therefore, in 2009 the EULAR task force advocated the use of a 1.5 multiplication factor for these risk prediction models when certain RA disease characteristics were present.4 In addition, certain commonly used variables in existing CVD risk prediction algorithms are influenced by inflammation and anti-inflammatory therapy. These risk factors behave differently in patients with IJD than in the general population, necessitating clarification and practical guidelines for rheumatologists in daily clinical practice.
For this update, a new EULAR task force reviewed all the previous recommendations from 2009 on CVD risk management in IJD. New areas were addressed, including the value of imaging in the routine assessment of CVD risk.
Methods
Task force
With the approval of the EULAR Executive Committee, the convenor (MTN) and methodologist (DPMS) who guided the task force in 2009 formed a new task force with the aim of reviewing and updating the 2009 EULAR recommendations for CVD risk management in RA and other IJD (see online supplementary file 1).4 The task force comprised 26 members from 13 European countries, including 2 patient representatives, 14 rheumatologists, 2 cardiologists, 3 internists, 1 healthcare professional and 4 fellows. The entire process was conducted in accordance with the 2014 EULAR standardised operating procedures.10
Literature search
The convenor (MTN) started by formulating a list of potential research questions. These were discussed and refined during a teleconference with other members of the task force. Thereafter, the fellows (RA, SCH, SR, MH) under guidance of the convenor (MTN) and the methodologist (DPMS) compiled the search terms for a comprehensive systematic literature review to cover all the research questions. The protocol for the literature search was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement (http://www.prisma-statement.org). The Wiley/Cochrane Library, Pubmed/Medline and Embase were searched from inception (by RA, SCH, MH and librarians LJS and JCFK). The Wiley/Cochrane Library was searched up to 9 February 2015, PubMed up to 10 February 2015 and Embase up to 13 February 2015. A single search was conducted embracing all aspects of the different research questions. The following search terms were used (including synonyms and closely related words) as index terms or free-text words: ‘rheumatoid arthritis’ or ‘spondyloarthritis’ and ‘cardiovascular disease’ and ‘cholesterol’ or ‘blood pressure’ or ‘smoking’ or ‘diabetes’ or ‘chronic kidney insufficiency’ or ‘sex factors’ or ‘vitamin D’ or ‘adrenal cortex hormones’ or ‘tumor necrosis factor’ or ‘anti-inflammatory agents’ or ‘inflammation’ or ‘carotid intima media’. The full search strategies for the Wiley/Cochrane Library, PubMed and Embase are shown in online supplementary file 2.
supplementary file
All duplicates were removed from the results of the first search (figure 1). The remaining studies were screened by title and abstract by six investigators (RA, SCH, SR, MH, DPMS and MTN) for suitability. Titles and abstracts were eligible if the abstract contained clear information about the aims and objectives of the study. From this selection of abstracts, full-text articles were assessed for eligibility by the fellows (RA, SCH, SR and MH). References of included articles were manually scanned for other relevant studies. The included articles were evenly divided among the four fellows, based on their area of expertise. Each fellow read the full texts and distilled and summarised the most important results. From these results, also taking into account the ten 2009 recommendations, 10 concept recommendations were derived.

{kind=link}
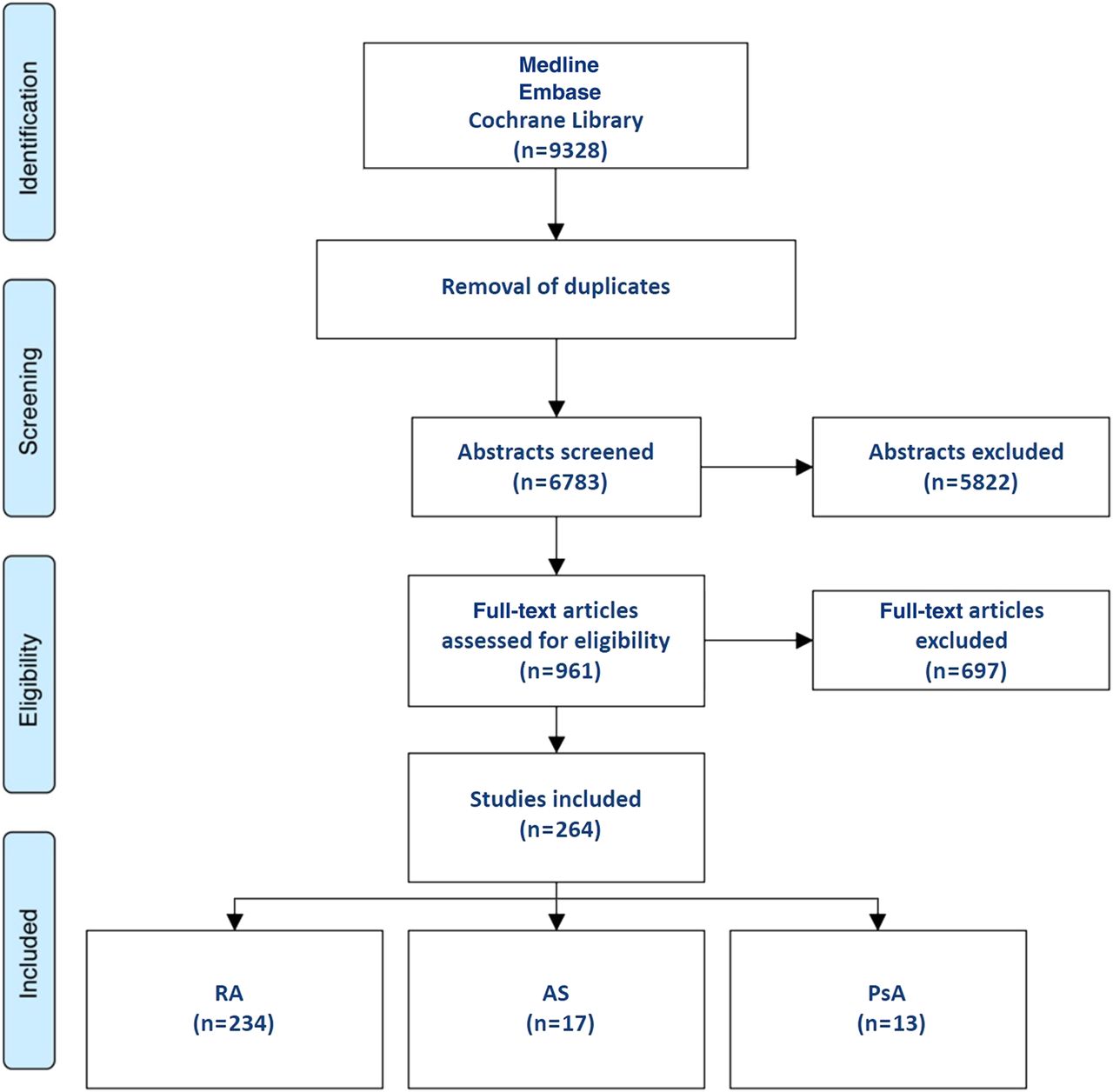
Flow chart of the search and selection process. RA, rheumatoid arthritis; AS, ankylosing spondylitis; PsA, psoriatic arthritis.
Consensus finding
The EULAR task force held a 1-day meeting with all members on 31 March 2015. During this meeting, the 10 concept recommendations were presented by the four fellows. All 10 concept recommendations were discussed and subsequently adapted or dropped, and new recommendations were formulated. The principles guiding the consensus meeting were: (1) all of the 2009 recommendations were reconsidered on the basis of new evidence, (2) any of the 2009 recommendations could be kept unchanged, be modified or be totally abandoned, (3) new recommendations could be added. After the meeting, the updated and new recommendations were graded based on the methodological strength of the underlying literature and were categorised according to the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) Working Group system.11 Thereafter, the 10 concept recommendations were sent out by email for anonymous voting. All members of the task force were asked to indicate their level of agreement (LOA) for each recommendation on a 0–10 scale (0, no agreement at all; 10, full agreement). The results on agreement were averaged and are hence presented as mean (SD).
Results
Literature search
In total, 9328 articles were identified. After removal of duplicates, 6783 articles were screened by title and abstract. In total, 961 full-text articles were assessed for eligibility by the fellows (RA, SCH, SR and MH). Ultimately, 264 articles were included (figure 1).
Overarching principles
The task force defined three overarching principles of CVD risk management in RA and other IJD (table 1).
Clinicians should be aware of the higher risk for CVD in patients with RA compared with the general population. This may also apply to AS and PsA
Acknowledging the increased CVD risk in IJD was included as a recommendation in our previous guideline of 2009. However, in view of its generic nature, this ‘recommendation’ was moved to the Overarching principles section of this paper. Since the publication of the 2009 EULAR recommendations, the evidence for an enhanced CVD risk in IJD has increased. For example, it was shown in a large Danish cohort study that the risk of myocardial infarction (MI) in patients with RA is comparable to that in patients with diabetes mellitus.2 Furthermore, in the same study the risk of MI in RA was found to be approximately 70% higher than in the general population, which corresponds with the risk of non-RA subjects who are 10 years older.2 Regarding mortality in RA, a meta-analysis including eight studies with follow-up ranging from the year 1955 to 1995 concluded that the standardised mortality rates (SMRs) in RA were elevated compared with the general population (ie, pooled SMR 1.47, 95% CI 1.19 to 1.83) and that these SMRs did not change over time.12 Data from the Norfolk Arthritis Register with follow-up until 2012 revealed comparable results with increased all-cause mortality in patients with RA compared with the general population along with stable SMRs over the past 20 years.13 New evidence strengthens the notion that the excess risk of CVD morbidity and mortality in patients with RA is related to both traditional and novel CVD risk factors. Novel risk factors include inflammation, presence of carotid plaques, anticitrullinated protein antibody (ACPA) and rheumatoid factor (RF) positivity, extra-articular RA manifestations, functional disability and hypothyroidism.14 ,15
Recent studies reveal increased SMRs in AS, ranging from 1.6 to 1.9.16–18 These studies report either death of circulatory origin or infection as the main cause of death in these patients.16–18 Compared with controls, patients with AS have an increased risk of vascular death and CVD events.19–27 Dyslipidaemia,27 increased prevalence of hypertension,19 ,21 ,22 ,28 diabetes mellitus19 ,22 ,25 and increased carotid intima media thickness (cIMT) or atherosclerotic plaques29–31 have all been reported in AS. Furthermore, an increased prevalence of (non-) atherosclerotic cardiac disease is reported in AS, such as aortic valve dysfunction and conduction disorders, but it is currently unknown whether and to what extent this affects CVD risk.32 ,33 In PsA, reported SMRs range from 0.8 to 1.6.17 ,34 ,35 Overall, patients with PsA are at an increased risk of CVD events; however, data on stroke are more conflicting.34 ,36–38 Likewise, in PsA CVD risk seems to be influenced by an increased prevalence of CVD risk factors such as hypertension37–40 and increased arterial stiffness.41–43
The rheumatologist should ensure that CVD risk management is performed in patients with RA and other IJD.
The responsibility for CVD risk management should be defined locally due to different healthcare systems and economic priorities in each country. Therefore, CVD risk management may include healthcare professionals other than rheumatologists. In clinical practice, it is not always clear who is taking responsibility for CVD risk assessment and management in patients with IJD and the task force therefore recommends that the treating rheumatologist should ensure that CVD risk assessment and management is being performed regularly, should record who is performing it and should make sure that the patient is aware of the need for regular risk assessment.
The use of non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids should be in accordance with treatment-specific recommendations from EULAR and the Assessment of Spondyloarthritis International Society (ASAS).44 ,45
NSAIDs and corticosteroids are commonly used for the treatment of IJD and these agents effectively lower disease activity and inflammation. However, both treatment options have been associated with an increased CVD risk.46–48 As these medications are often indispensable in tackling disease activity in patients with IJD, the task force feels that their use should be evaluated on an individual patient level. Furthermore, lowering disease activity may have beneficial effects on the CVD risk. Therefore, the task force recommends to use NSAIDs and corticosteroids according to treatment-specific guidelines.
Overarching principles and recommendations
Recommendations
In line with the 2009 guidelines, we opted to give again 10 recommendations for CVD risk management. In total, three recommendations remained unchanged, six recommendations were altered and there is one new recommendation. One of the 2009 recommendations (#1) was moved to the overarching principles as described previously. A list of the updated recommendations, including the levels of evidence with the strength of recommendation and the LOA based on voting by the task force, is shown in table 1. The recommendations follow a logical sequence, and they are not listed in sequence of importance. All recommendations are discussed in detail below.
Disease activity should be controlled optimally in order to lower CVD risk in all patients with RA, AS or PsA (unchanged, LOA 9.1 (1.3)).
In the previous recommendations from 2009, the importance of control of disease activity to lower CVD risk was emphasised. New evidence still portrays an association between higher cumulative inflammatory burden and increased CVD risk in RA.49–54 Disease duration does not seem to affect CVD risk independently.50 However, disease activity as well as the number and duration of flares over time do contribute to the risk of CVD.49–52 There is now additional evidence showing a reduction of CVD risk in patients treated with disease-modifying antirheumatic drugs (DMARDs). Reducing inflammation is important in RA for CVD risk management, but the type of treatment may be less important. Conventional synthetic DMARDs (csDMARDs), in particular methotrexate (MTX), as well as biological DMARDs (bDMARDs), such as the TNF inhibitors (TNFi), are often associated with a significant reduction in CVD risk in patients with RA.46 ,49 ,51 ,53 ,55–62 The CVD risk appears to decrease even further after long-term use.53 ,56 Reduction of disease activity after treatment with tocilizumab or rituximab (RTX) shows a beneficial effect on cIMT, a surrogate marker for CVD, and CVD risk in a limited number of studies.54 ,63–65 Beneficial effects of TNFi and MTX on arterial stiffness have also been described.43 ,66–71 One study described a reduction in aortic inflammation and stiffness measured by 18F-FDG positron emission tomography-CT after TNFi treatment in patients with RA.72
For both AS and PsA, evidence for the association between inflammation and an enhanced CVD risk is less abundant compared with RA. In view of shared pathogenic mechanisms, it is plausible that decreasing the inflammatory burden in AS and PsA will also have favourable effects on the CVD risk in these patients. Therefore, control of disease activity, as is routinely recommended, is expected to lower CVD risk for both AS and PsA.
CVD risk assessment is recommended for all patients with RA, AS or PsA at least once every 5 years and should be reconsidered following major changes in antirheumatic therapy (changed, LOA 8.8 (1.1)).
CVD risk assessment is recommended for all patients with RA, AS or PsA at least once every 5 years, so that lifestyle advice and CVD preventive treatment can be initiated when indicated. The advice to screen patients with IJD for CVD risk on a yearly basis has been changed to screening every 5 years, which is in line with the latest ESC guidelines.7 Currently, there is no evidence that annual CVD risk assessment compared with 5-year risk assessment leads to a more significant reduction in CVD mortality or morbidity in patients with IJD. Depending on the CVD risk algorithm that is used for screening, patients can be categorised as having low to moderate risk (eg, SCORE <5%), high risk (eg, SCORE ≥5% and <10%) and very high risk (eg, SCORE ≥10%).7 Once screened, patients with a low risk can be routinely screened again after 5 years. However, if the risk is intermediate rescreening may be done sooner, especially if disease progression is more rapid. Patients with a high risk or established CVD should be treated for all present CVD risk factors according to existing guidelines. A healthy lifestyle should be recommended to all persons, including patients with low and intermediate cardiovascular risk.7 CVD risk evaluation should be reconsidered after major changes in antirheumatic therapy, that is, the initiation of bDMARDs or other drugs that may cause pronounced increases in low-density lipoprotein cholesterol (LDLc) or alter other CVD risk factors, so that doctors can act accordingly.73 ,74
CVD risk assessment for patients with RA, AS or PsA should be performed according to national guidelines and the SCORE CVD risk prediction model should be used if no national guideline is available (unchanged, LOA 8.7 (2.1)).
Evidence is scarce with regard to the validity of disease-specific CVD risk prediction models to accurately predict risk in individual patients with RA, and it is therefore currently recommended to perform risk evaluation according to general population guidelines. Several novel and RA disease-specific factors have been associated with an increased risk of CVD, but at present it is uncertain if these factors will meaningfully and cost-effectively improve CVD risk prediction in patients with RA.
Total cholesterol (TC) and high-density lipoprotein cholesterol (HDLc) should be used in CVD risk assessment in RA, AS and PsA and lipids should ideally be measured when disease activity is stable or in remission. Non-fasting lipids are perfectly acceptable (changed, LOA 8.8 (1.2)).
The relationship between serum lipid levels and CVD risk is non-linear and potentially paradoxical in RA. Patients with RA with highly active disease generally have lower serum TC and LDLc levels compared with the general population, while their CVD risk is elevated.73 ,75–78 As described in the 2009 recommendations, these patients also have reduced serum levels of HDLc and higher levels of triglycerides as compared with healthy controls.78–81 In general, controlling disease activity has widespread effects on the lipid profile. Treatment with TNFi and/or csDMARDs (mainly MTX) results in an overall increase of lipid components, but mostly HDLc, which improves the TC/HDLc ratio.79–93 A limited number of studies have reported beneficial effects of RTX and tocilizumab on individual lipid components.64 ,94 ,95 However, the net effect of treatment with these agents is an overall increase of individual lipid components without changes in TC/HDLc ratio.54 ,96–101 The same appears to be true for tofacitinib.100 Still, statins are effective at reducing lipid levels in tocilizumab or tofacitinib-treated patients with sustained elevations of TC and LDLc.99 ,100 As described in the 2009 recommendations, the TC/HDLc ratio is a better CVD risk predictor in RA than individual lipid components.78 ,102 From a practical point of view, both TC and HDLc can be used when using online calculators. As lipid components appear to be modifiable by disease activity and anti-inflammatory therapy, assessment of the lipid profile should preferably be done when a patient has stable disease or is in remission. Finally, measurement of TC and HDLc are perfectly acceptable in non-fasting state, as noted in the recent 2016 European Guidelines on CVD prevention in clinical practice: prevention guidelines.7
CVD risk prediction models should be adapted for patients with RA by a 1.5 multiplication factor, if this is not already included in the risk algorithm (changed, LOA 7.5 (2.2)).
The SCORE risk calculator is recommended for CVD risk prediction in the general population by the ESC guidelines.103 However, CVD risk prediction models developed for the general population do not include non-traditional CVD risk factors and hence there is a possibility of underestimation of future CVD if these models are applied in patients with RA. It is indeed reported that several CVD prediction models inaccurately predict the risk of CVD in patients with RA.8 ,104 ,105 The 2009 EULAR recommendations for CVD risk management suggested a multiplication factor of 1.5 to the calculated total CVD risk if the patient fulfilled certain disease-specific criteria (ie, disease duration of >10 years, RF or ACPA positivity and the presence of certain extra-articular manifestations).4 It has been argued that the application of this multiplication factor does not reclassify as many patients as was expected into a more appropriate risk category.9 ,106 In addition, QRESEARCH Cardiovascular Risk Algorithm (QRisk) 2, a CVD risk prediction model that includes RA as a risk factor with a multiplication factor of 1.4 for all patients with RA,107 tended to overestimate the CVD risk in patients with RA. QRISK 2 estimates the risk of fatal and non-fatal CVD combined.8 Currently, there are no alternative CVD risk prediction models with a proven accuracy and superiority for patients with IJD. Based on all recent epidemiology, this multiplication factor is still the most evidence-based way of estimating CVD risk in patients with RA. Therefore, the use of an RA-adapted risk prediction model is recommended over the use of an unadapted general population model, since there is a higher level of evidence on their predictive value. Based on this, the EULAR task force still recommends to adapt general population CVD risk algorithms (except for QRISK 2, in which the multiplication factor is intrinsic to the algorithm) with a 1.5 multiplication factor for all patients with RA. In contrast to the 2009 recommendations, the presence of certain RA-specific criteria is not mandatory anymore for the application of this multiplication factor, as evidence on the increased CVD risk in patients who are in the early stages of RA, patients with a recent RA diagnosis and patients without extra-articular manifestations.108 ,109
Screening for asymptomatic atherosclerotic plaques by use of carotid ultrasound may be considered as part of the CVD risk evaluation in patients with RA (new, LOA 5.7 (3.9)).
The presence of carotid plaques is associated with poor CVD-free survival and is strongly linked to future acute coronary syndrome (ACS) in patients with RA, with a rate of ACS of 1.1 (95% CI 0.6 to 1.7) per 100 person-years (pyrs) for patients with RA with no carotid plaques and 4.3 (95% CI 2.9 to 6.3) per 100 pyrs for those with bilateral plaques.66 ,110 RA-specific factors contribute to the presence of carotid atherosclerosis in addition to traditional CVD risk factors.111 Disease duration and disease activity have been shown to be associated with plaque size and vulnerability in patients with RA.112 ,113 The most recent ESC Guidelines on CVD prevention in clinical practice recommend considering screening for carotid artery atherosclerosis in patients with moderate CVD risk (class: IIa, level of evidence: B, GRADE: strong).7 Autoimmune diseases like RA, systemic lupus erythematosus and psoriasis were acknowledged as diseases with increased CVD risk.7 Due to the high pretest probability for detection of carotid artery plaques by use of ultrasound in patients with RA, and the clinical consequence of indication for statin treatment if a carotid plaque is present, this procedure could be of additional value for CVD risk evaluation. Ultrasound of the carotid arteries to identify atherosclerosis has been shown to reclassify a considerable proportion of patients with RA into a more appropriate CVD risk group in accordance with current guidelines.114
Lifestyle recommendations should emphasise the benefits of a healthy diet, regular exercise and smoking cessation (changed, LOA 9.8 (0.3)).
Since the 2009 recommendations, no new strong evidence has emerged on the role of smoking on CVD risk in IJD and hence this recommendation remains unchanged. Thus, patients should be advised to stop smoking and directed towards the locally defined evidence-based smoking cessation programmes, even if they have failed previously. The 2009 recommendations did not discuss diet or exercise, but it was mentioned in the research agenda.4 Research on the role of exercise in RA management has advanced considerably since 2009. Physical inactivity is common in patients with RA, and has been associated with an adverse CVD risk profile.115–117 There is accumulating data that structured exercise therapy has beneficial CVD effects in patients with RA, at least in the short and medium term.118–120 Exercise has been shown to reduce long-term inflammation in epidemiological studies conducted in the general population and increased physical activity was associated with lower levels of C reactive protein (CRP).121 This has also been demonstrated in a study with patients with RA in which a 6-month exercise programme lowered CRP levels, probably related to a reduction in body fat.118 Moreover, improvements in both microvascular and macrovascular function were found after 3 months of exercise in RA.120 To date, no studies have shown any adverse effects as a result of exercise.119 Hence, in RA, high-intensity exercise is not contraindicated and should be encouraged in those already accustomed to activity. Physical activity that is enjoyable is more likely to be sustained.
A Mediterranean diet is characterised by a high consumption of fruit, vegetables, legumes and cereals, and contains less red meat and more fish compared with common Western diets. Olive oil or vegetable oil is the primary source of fat intake. This diet has been shown to be associated with a reduced incidence of major CVD events in the general population.122 In RA, the positive effect of a Mediterranean diet may be mediated by the effect of this diet on disease activity.123 However, there is no specific evidence available on the effect of dietary modifications on CVD risk in patients with IJD. Therefore, we recommend national guidelines regarding a healthy diet as part of a healthy lifestyle as discussed below.
An important issue remaining is how lifestyle interventions should be advocated to patients with IJD. Studies in this field demonstrate that if information is provided, this should be linked to behavioural education.124 A randomised controlled trial in patients with RA evaluated the effect of cognitive behavioural patient education with regard to modifiable CVD risk factors in people with RA: patients receiving this intervention had more knowledge, and improved behavioural intentions, however, actual behaviour did not differ between groups.125 Obviously, this area is in need of more research.
CVD risk management should be carried out according to national guidelines in RA, AS or PsA, antihypertensives and statins may be used as in the general population (changed, LOA 9.2 (1.3)).
Hypertension is a major modifiable risk factor contributing to increased CVD risk in IJD.126–128 Several mechanisms may lead to the development of hypertension, including the use of certain antirheumatic drugs such as corticosteroids, NSAIDs, ciclosporin and leflunomide.129–132 It is important to realise that hypertension seems to be both underdiagnosed and undertreated in patients with RA.127 For the management of hypertension and hyperlipidaemia, there is no evidence that treatment thresholds should differ in patients with IJD compared with the general population. In the past years, no new evidence has emerged that ACE inhibitors and angiotensin II (ATII) receptor blockers should be the preferred treatment choice for hypertension in patients with RA. Therefore, the previous treatment preferences for ACE inhibitors and ATII receptor blockers have been omitted.
Since the 2009 recommendations, several studies have assessed the efficacy of statins in patients with RA. Statins appeared to be at least as effective in reducing cholesterol levels, atherosclerotic burden and CVD morbidity and mortality, and they do not have more adverse reactions in patients with RA when compared with non-RA controls.77 ,133–139 In addition, statins have anti-inflammatory properties that may result in an even greater CVD risk reduction when combined with anti-inflammatory therapy in RA, but studies on this effect are scarce.140–142 A few preclinical studies found unfavourable effects of statins on RTX efficacy in patients with haematological malignancies.143 ,144 However, several clinical studies showed no significant differences in outcome between statin users and non-users receiving RTX treatment for a haematological malignancy.145–148 Clinical trials investigating this issue in RA are scarce. Three clinical studies in RA found no adverse effect of statins on RTX efficacy.149–151 Only one observational study reported a significant difference in disease activity 6 months after first RTX treatment in statin users as compared with non-users, but this finding was borderline significant (p=0.049) in a small sample size of statin-exposed patients (n=23 exposed vs n=164 non-exposed).152 Obviously, further research is necessary to address this issue properly.
Prescription of NSAIDs in RA and PsA should be given with caution, especially for patients with documented CVD or in the presence of CVD risk factors (changed, LOA 8.9 (2.1)).
The 2009 recommendations advocate that NSAIDs should be used with caution in this population or may even be contraindicated.4 ,153 ,154 Since the publication of the former recommendations, new evidence has emerged on the role of cyclooxygenase-2 inhibitors (COXIBs) and non-selective NSAIDs in CVD risk. A recent meta-analysis concluded that, overall, both non-selective NSAIDs and COXIBs have adverse effects on CVD outcomes in patients with RA and PsA.46 However, the increased CVD risk was mainly observed for rofecoxib, which was withdrawn from the market in 2004. There is evidence that NSAIDs might increase CVD risk in RA to a lesser extent in comparison to the general population than was previously thought.48 Hence, there is no evidence to be stricter with NSAID treatment in patients with RA than what is recommended in the national guidelines for patients with no RA. Safety data regarding the use of NSAIDs in patients with IJD and prevalent CVD comorbidities are lacking. Naproxen seems to have the safest CVD risk profile.46 ,48 In general, diclofenac is contraindicated in patients with established congestive heart failure (NYHA class II–IV), ischaemic heart disease, peripheral arterial disease or cerebrovascular disease, and new evidence supports similar restrictions for ibuprofen use.153 ,154
For patients with AS, NSAIDs are recommended as first-line drug treatment by the ASAS/EULAR group in the recommendations for the management of pain and stiffness in patients with AS, and an individual clinical evaluation regarding NSAIDs use in patients with AS with established CVD is therefore needed.155
Corticosteroids: for prolonged treatment, the glucocorticoid dosage should be kept to a minimum, and a glucocorticoid taper should be attempted in case of remission or low disease activity; the reasons to continue glucocorticoid therapy should be regularly checked (unchanged, LOA 9.5 (0.7)).
Corticosteroids rapidly and effectively reduce inflammation in RA, but they have also been associated with an increased CVD risk, although the literature shows conflicting results. Since the 2009 recommendations, new studies have found a dose-dependent and duration-dependent increase in CVD risk associated with corticosteroid use in RA.47 ,156 ,157 A relatively high daily dose (ie, already starting from 8 to 15 mg/day), a high cumulative dose and a longer exposure to corticosteroids (in years) appear to be associated with a higher CVD risk.47 ,156–158 Some authors argued that this increased CVD risk was confounded by indication, as it was no longer significant after correction for disease activity.53 ,159–161 On the contrary, other studies that had corrected for disease activity still found a (cumulative) dose-dependent and duration-dependent increase in CVD-related morbidity and mortality in patients with RA.47 ,156 However, this does not mean that confounding by indication has been completely addressed and this is a major limitation of all safety studies on corticosteroids. There is no conclusive evidence about the long-term effects of corticosteroids, particularly in low daily dosage, on safety outcomes including CVD events in RA. In patients with active disease, the benefit of reducing high-grade inflammation may counteract the adverse CVD effects of corticosteroid use by reduction of inflammation and by improving mobility. In other words, steroids may help to abrogate the harmful effect of inflammation on the cardiovascular system, but they will still carry their own adverse effects on CVD risk. Altogether, from a CVD prevention point of view, the lowest effective dose of corticosteroids should be prescribed for the shortest possible duration in the treatment of active IJD. This recommendation is in line with the EULAR recommendations on management of glucocorticoid therapy.44
Discussion
The 2015 update of the 2009 EULAR recommendations for CVD risk management in IJD comprises 3 overarching principles and 10 recommendations. The first overarching principle reinforces and extends the evidence of an increased CVD risk in IJD. The second principle indicates the responsibility of the rheumatologist for coordinating CVD risk management in patients with IJD, whereas the last principle aims to put this recommendation update more in line with other (EULAR) recommendations.
CVD risk assessment in IJD
Presently, the enhanced CVD risk in RA, but also in AS and PsA, is widely acknowledged. Thus far, fully validated RA-specific CVD risk prediction models that both improve on general population models and are cost-effective are lacking, although multiple attempts have been made.8 ,105 ,162 Some even question the need for a disease-specific CVD risk prediction model for RA, although existing models inaccurately estimate the CVD risk in these patients.8 ,9 In 2009, this led to the addition of a 1.5 multiplication factor for the calculated CVD risk in patients with RA if certain disease characteristics were present.4 Meanwhile, alternative approaches have also been advocated, for example, to increase the age of a patient with RA by 15 years163 or adding a multiplication factor of 1.4.3 Currently, it is unknown what approach would be most appropriate. In the light of this, the task force opted to retain the 1.5 multiplication factor to correct for the increased CVD risk in patients with RA compared with the general population. However, considering that the CVD risk is already increased in early disease or at disease onset and in patients without extra-articular manifestations, the three disease-specific criteria for the application of this multiplication factor were removed. This makes the estimation of CVD risk in patients with RA easier and therefore more feasible for daily clinical practice. As no conclusive evidence has emerged regarding the precise CVD risk in patients with AS and PsA, the task force opted not to include a multiplication factor for these diseases. In line with the ESC Guidelines, the recommendation to perform CVD risk assessment was extended to once every 5 years for patients found to be at low-to-moderate cardiovascular risk as there is no evidence that CVD risk assessment every year for IJD reduces CVD risk more than screening every 5 years.164 In patients with an intermediate risk for CVD, screening should be performed more often. Patients at high to very high cardiovascular risk should promptly be treated for existing CVD risk factors. The new recommendation (#6) includes the option of screening for carotid plaques in patients with RA as a tool for CVD risk assessment, because carotid plaques are associated with future ACS in patients with RA. Whether routine screening of the carotid arteries is possible in daily clinical practice will depend on local availability. The LOA of 5.7 (3.9) for recommendation #6 possibly indicates the absence of evidence for routine screening of the carotid arteries in general.
CVD risk reduction in IJD
Just as in the 2009 recommendations, the importance of optimal anti-inflammatory therapy for CVD risk reduction in RA is emphasised in this update. There is accumulating evidence that decreasing the inflammatory burden in RA translates into a lower CVD risk. As inflammation is related to CVD risk in all IJD, we extrapolated this recommendation to AS and PsA, although further evidence for these types of IJD would be valuable. Equally important is the treatment of traditional CVD risk factors that are present in these patients according to national guidelines.128 However, awareness of some issues when performing risk estimation and management in patients with IJD is important. Active disease of IJD is associated with reduced lipid levels that increase (ie, normalise) during effective anti-inflammatory treatment. Biologics have the most pronounced lipid increasing effect, which has led to mandatory lipid assessment during treatment with tocilizumab.100 However, it is also important to realise that the anti-atherogenic properties of HDLc improve during biologic treatment.94 ,95 Therefore, it is important to assess the net effect of lipid modulation by biologics. Currently, the effect of these changes on CVD outcomes is not known. In addition, awareness of possible adverse effects of certain medications such as NSAIDs and corticosteroids has been emphasised. Except for smoking cessation, lifestyle recommendations were not given in our previous guideline. Since then accumulating data demonstrate that regular physical activity has beneficial CVD effects in patients with RA and hence this has been incorporated in the updated recommendations. In addition, favourable CVD effects have also been observed with a Mediterranean diet, although a formal study in patients with IJD has not yet been conducted. As it is not likely that the effect of diet would be different in patients with IJD than in the general population, we also added this in our lifestyle recommendation.
Conclusion
In general, the LOA for the recommendations was (very) high, except for recommendations #5 (LOA 7.5) and #6 (LOA 5.7). As in 2009, the level of evidence was moderate for most of the recommendations. Several important questions which arose during the development of these recommendations remain unanswered. These questions have been put on the research agenda (box 1). The 2015/2016 update of the EULAR recommendations for CVD risk management in patients with RA and other forms of IJD confirms and further extends the evidence of an increased CVD risk in the whole spectrum of IJD and reinforces the need for proper CVD risk management in these patients. As these updated recommendations are based on a pan-European consensus, it is hoped that they will facilitate CVD risk management in daily clinical practice, ultimately leading to a decreased CVD burden in our patients.
Research agenda
Can we make adjustments to the current CVD risk models to improve estimation of CVD risk in patients with IJD?
How high is the CVD risk in patients with spondyloarthropathies or non-radiographic axial SpA compared with the general population?
What is the benefit/risk ratio of intensive anti-inflammatory therapy on CVD risk in patients with IJD?
Is the increased CVD risk in patients with spondyloarthropathies independent of traditional risk factors and what is the association between CVD risk and inflammation in spondyloarthropathies?
Is there an increased prevalence of cardiac abnormalities, including aortic valve dysfunction and conduction disorders in patients with spondyloarthropathies and how does this affect overall CVD risk?
How does treatment with NSAIDs affect the CVD risk in patients with IJD, in particular patients with AS?
Should we treat patients with AS continuously or intermittently with NSAIDs from a CVD point of view?
Should treatment targets for blood pressure and lipids be different in patients with IJD from the general population?
What is the effect of different modes of action of antirheumatic drugs on CVD risk?
What is the relationship between residual disease activity and CVD risk in patients with RA on stable DMARD therapy?
Is there additional value in measuring lipid subparticles in patients with IJD for estimation of CVD risk?
What is the added value of ultrasound of the carotid arteries to measure cIMT and reveal presence of atherosclerotic plaques in patients with IJD regarding CVD risk estimation and in which (sub) population should we conduct this?
What is the additional value of novel biomarkers for CVD risk prediction?
What is the best technique for implementing lifestyle changes and education in patients with IJD?
Health economics. Are interventions cost-effective in terms of reducing the number of fatal and non-fatal CVD events?
Is the prevalence of venous thrombotic events in patients with IJD increased? If so, what are the underlying mechanisms?
AS, ankylosing spondylitis; CVD, cardiovascular disease; DMARD, disease-modifying antirheumatoid drug; IJD, inflammatory joint disorder; cIMT, carotid intima media thickness; NSAID, non-steroidal anti-inflammatory drug; PsA, psoriatic arthritis; RA, rheumatoid arthritis; SpA, spondyloarthropathy.
Acknowledgments
We thank Johannes C.F. Ket, MSc and Linda J. Schoonmade, MSc, Medical Information Specialists, Medical Library, VU University Amsterdam, for their contribution to the systematic literature searches.
References
Footnotes
Handling editor Hans WJ Bijlsma
RA, SCH, SR and MH are co-first authors.
DPMS and MTN are senior authors.
Contributors All authors participated in the activities of the EULAR task force and have provided important contributions to the manuscript.
Funding European League Against Rheumatism.
Competing interests All the participants in this initiative have disclosed any conflicts of interest. FA has received personal remuneration from BMS, Pfizer, MSD. IBM has received research funding or honoraria from AbbVie, BMS, Pfizer, Janssen, Novartis, Celgene, MSD, UCB and Roche. LJ has received consultancy fees or speaker honoraria from AbbVie, Actavis, Celgene, Novartis and Pfizer. GDK has received honoraria for lectures or advisory boards or hospitality from Pfizer, AbbVie, Novartis, UCB, Genesis, Roche, BMS, GSK, Eli Lilly and AstraZeneca. TKK has received fees for speaking and/or consulting from AbbVie, Biogen, BMS, Boehringer Ingelheim, Celgene, Celltrion, Eli Lilly, Epirus, Hospira, Merck-Serono, MSD, Novartis, Orion Pharma, Pfizer, Roche, Sandoz and UCB and received research funding to Diakonhjemmet Hospital from AbbVie, BMS, MSD, Pfizer, Roche and UCB. NS has consulted for Roche, Amgen, Sanofi, AstraZeneca and received grant funding from Roche. SWJ has received speaker honoraria from MSD and Pfizer. MTN has received research funding or speaking/consultancy honoraria from Abbvie, Pfizer, Merck, Roche, BMS, UCB, Eli Lilly and Janssen.
Provenance and peer review Not commissioned; externally peer reviewed.