Article Text

Abstract
Background The main therapeutic goals that can determine success of biologic treatment in systemic juvenile idiopathic arthritis (SJIA) include achieving and maintaining clinical remission, controlling disease activity and tapering corticosteroids (CS). Canakinumab (CAN) has been shown to improve several of these parameters in previous studies1. However, little is known about SJIA patients (pts) using CAN long-term.
Objectives To evaluate the efficacy, safety and long-term treatment response of CAN treatment-naïve pts with active SJIA.
Methods This was an open-label, non-comparative study (NCT00891046) of CAN-naïve SJIA pts (age ≥2 - <20 yrs) receiving CAN 4 mg/kg by s.c. q4w. Efficacy was assessed by the adapted pediatric ACR (aACR 30/50/70/90/100) responses compared to baseline (BL); inactive disease (ID) or clinical remission (ID for >6 Mo) and changes in JADAS-CRP (Juvenile Arthritis Disease Activity Score- C-reactive protein) scores over time. Safety was assessed by adverse events (AEs) and serious AEs (SAEs) reports.
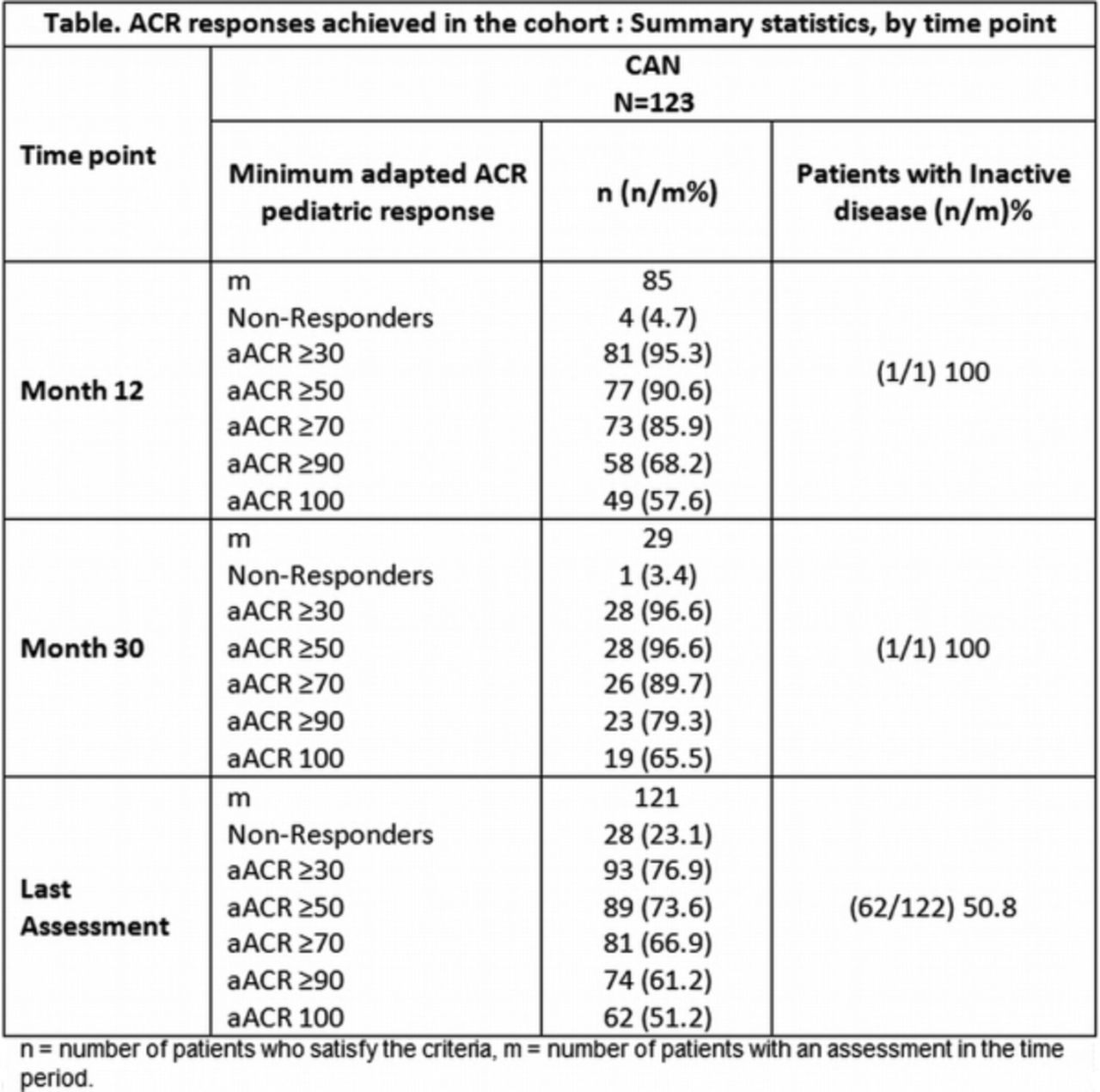
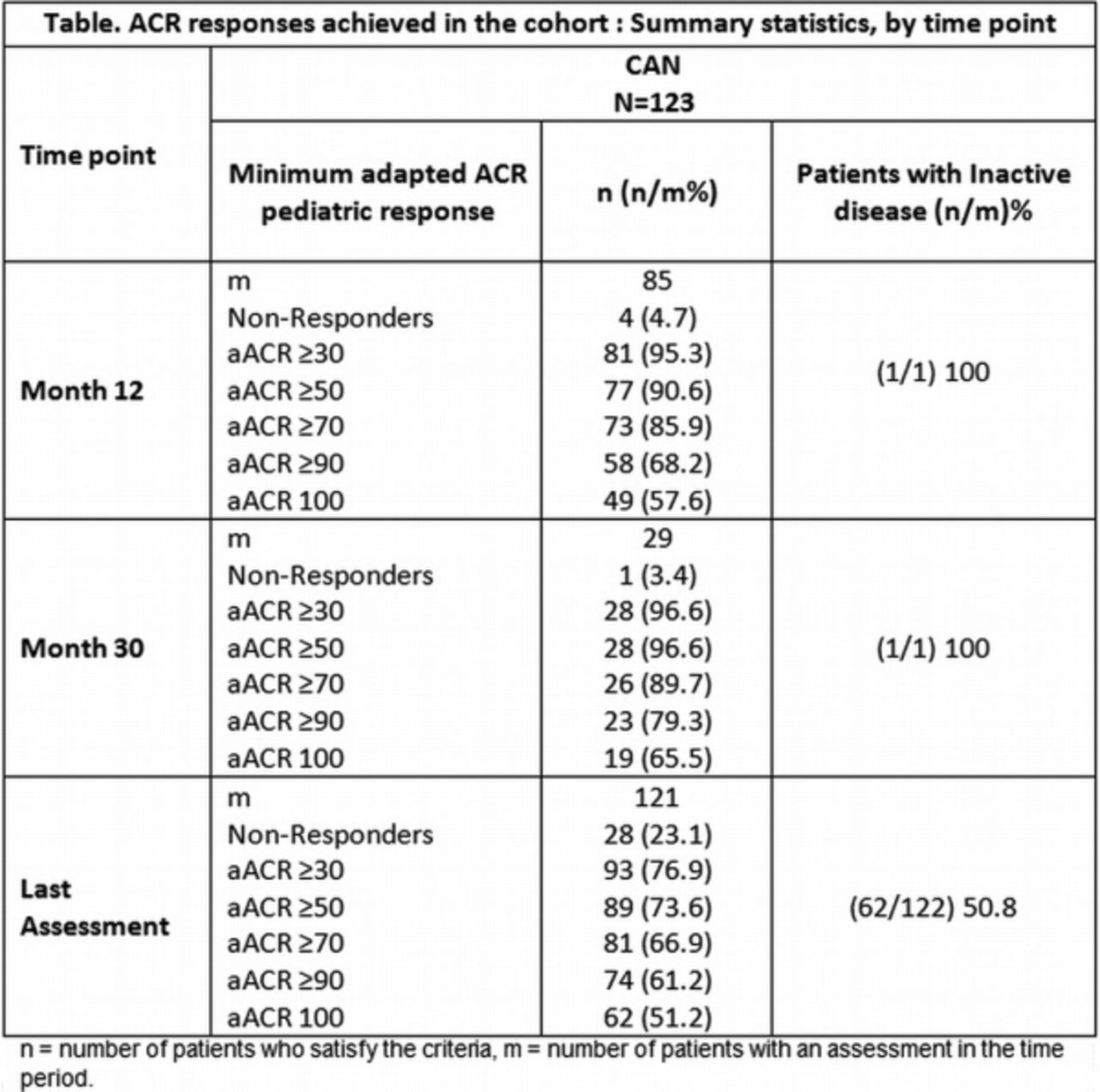
Results A total of 123 pts with active SJIA were enrolled of whom 70 (57%) pts had fever and 71 (57.7%) pts used CS at BL. Mean CRP was 117.8 mg/L (normal: 0–10mg/L) and, on average, pts had, 9.9 active joints and 8.9 joints with limited motion. A rapid response was observed at Day 15, 59 (51%) with aACR ≥70 responses and 27 (26%) having aACR 100 responses. These responses increased and were maintained at subsequent time points (Table). Overall, 73.0% of pts had ID on at least 1 visit. At 6th month, clinical remission was achieved in 52 (42.3%) pts and 33 (26.8%) pts had clinical remission for at least 12 consecutive months. At BL, the median JADAS10-CRP score was 22.3 (indicating high disease activity), with median changes from BL of -12.0 at Day 15 and -16.8 at last assessment indicating moderate and low disease activity, respectively. At the last assessment, 59 (48.4%) pts were rated as ID (JADAS <1); 14 (11.5%) with low active disease activity (JADAS >1 and <3.8); while 14 (11.5%) had moderate and 35 (28.7%) with high disease activity. 24 (33.8%) pts were steroid-free at last assessment. A total of 53 (43.4%) pts had at least 1 AE. Overall rate of AEs was 2.25 events/ 100 patient-days and SAEs was 0.15/ 100 patient-days. 40 (32.5%) pts had SAEs and the most commonly reported were disease flares or worsening of SJIA in 13 (10.6%) pts, macrophage activation syndrome in 6 (4.9%) pts, and pyrexia in 4 (3.3%) pts. No deaths were reported in this study.
{kind=link}
Conclusions In this long-term study, CAN treatment was associated with rapid response and sustained therapeutic effect over the long-term in the naïve pts with active SJIA. The safety profile is consistent with other CAN studies.
Ruperto et al. N Engl J Med. 2012;367:2396–406.
Disclosure of Interest N. Ruperto Grant/research support from: BMS, GlaxoSmithKline (GSK), Hoffman-La Roche, Janssen, Novartis, Pfizer, Sanofi Aventis, Schwarz Biosciences, Sobi and Merck Serono funded The Gaslini Hospital for the research activities of the hospital in a fully independent manner besides any commitment with third parties, Consultant for: AbbVie, Amgen, Biogenidec, Alter, AstraZeneca, Baxalta Biosimilars, Boehringer, BMS, Celgene, CrescendoBio, EMD Serono, Hoffman-La Roche, Janssen, MedImmune, Medac, Novartis, Novo Nordisk, Pfizer, Sanofi Aventis, Servier, Takeda, UCB Biosciences GmbH, Speakers bureau: AbbVie, Amgen, Biogenidec, Alter, AstraZeneca, Baxalta Biosimilars, Boehringer, BMS, Celgene, CrescendoBio, EMD Serono, Hoffman-La Roche, Janssen, MedImmune, Medac, Novartis, Novo Nordisk, Pfizer, Sanofi Aventis, Servier, Takeda, UCB Biosciences GmbH, H. Brunner Consultant for: Novartis, Genentech/Roche, BMS, Pfizer, Astrazeneca, Jannsen, Tekada, Biogen, BAXALTA, Speakers bureau: Novartis, Genentech/Roche, P. Quartier Grant/research support from: Abbvie, Novartis, Pfizer, Roche, Consultant for: Abbvie, Novartis, Sobi, Speakers bureau: Abbvie, BMS, Novartis, Pfizer, Roche, Sobi, T. Constantin Consultant for: Pfizer, Abbvie, Roche, Novartis, Bristol-Myers Squibb, Speakers bureau: Pfizer, Abbvie, Roche, Novartis, Bristol-Myers Squibb, E. Alexeeva Grant/research support from: Roche, Abbott, Pfizer, Centocor, Novartis, Speakers bureau: Roche, Pfizer, I. Kone-Paut Grant/research support from: Grant/research support to my institution: SOBI, Roche, Novartis, Consultant for: Novartis, SOBI, Pfizer, CHUGAI, Abbvie, K. Marzan Grant/research support from: Novartis and Abbvie, N. Wulffraat Grant/research support from: Sobi, AbbVie, Consultant for: Novartis, Pfizer, R. Schneider Consultant for: Novartis, Roche, Sobi, S. Padeh: None declared, V. Chasnyk: None declared, C. Wouters Grant/research support from: Unrestricted grant support GSK, Novartis, Roche, J. Kuemmerle-Deschner Grant/research support from: Novartis, Consultant for: Novartis, SOBI, Baxalta, T. Kallinich Speakers bureau: Novartis, B. Lauwerys: None declared, E. Haddad Grant/research support from: Unrestricted Institutional Educational Fund, E. Nasonov: None declared, M. Trachana Grant/research support from: Pfizer, O. Vougiouka Grant/research support from: Novartis, K. Leon Employee of: Novartis, A. Speziale Employee of: Novartis, K. Lheritier Employee of: Novartis, A. Martini Grant/research support from: Abbott, Bristol Myers and Squibb, Francesco Angelini S.P.A., Glaxo Smith &
Kline, Janssen Biotech Inc Novartis,Pfizer Inc,Roche,Sanofi Aventis and Schwarz
Biosciences GmbH funded Gaslini Institute for the PRINTO research activities, Consultant for: Bristol Myers and Squibb, Janssen Biotech Inc,Glaxo Smith & Kline, Novartis,
Pfizer Inc, Roche, Sanofi Aventis and Schwarz Biosciences GmbH Biosciences GmbH funded Gaslini Institute for the PRINTO research activities, D. Lovell Grant/research support from: National Institutes of Health, NIAMS, Consultant for: Astra-Zeneca, Bristol Meyers Squibb, AbbVee, Pfizer, Roche, Novartis, UBC, Forest Research Institute, Horizon, Johnson & Johnson, Biogen, Takeda, Genentech, Glaxo Smith Kline, Boehringer Ingelheim, Celgene, Jannsen, Speakers bureau: Genentech