Article Text

Abstract
Background Lupus anticoagulant (LA), IgM and IgG anticardiolipin (ACL), and anti-beta2 glycoprotein 1 (b2GPI) Ab, positive twice 12 weeks apart, constitute laboratory diagnostic criteria of the Antiphospholipid Syndrome (APLS) in patients with or without SLE. IgA ACL and b2GPI Ab subclasses are not included in this classification.
Objectives We investigated the prevalence and contribution of various (sub)classes of APLs to thrombotic events in a multiethnic cohort of SLE patients. We further evaluated the independent contribution of a-b2GPI IgA to thrombotic events above and beyond criteria APL subclasses and clinical risk factors.
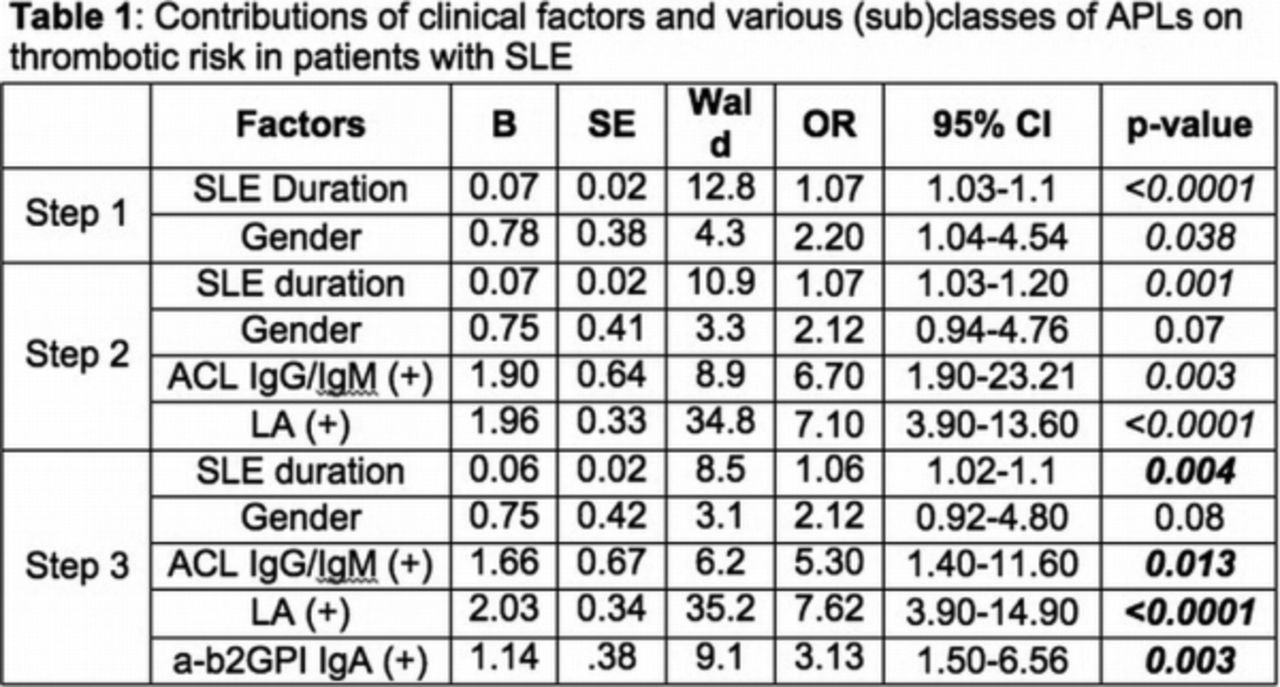
Methods A total of 401 patients (232 latinos, 109 African Americans, 25 Caucasians and 35 Asians) fulfilling ≥4 1996 criteria for SLE, and follow-up in a single center between 2008 and 2015 were included. LA was assessed with both aPTT and DRVVT. ACL and a-b2GPI subclasses were tested using commercial ELISA kits and positivity was defined according to manufacturer specifications. Logistic regression models assessed incremental thrombotic risk by higher numbers of APL Abs. Hierarchical forward stepwise regression models evaluated incremental thrombotic risk by a-b2GPI IgA, after accounting for clinical factors (step 1, table 1), and other APL (sub)classes (step 2).
Results Of 401 patients, 92 (23%) had 1 APL Ab class, 12 (3.1%) had 2, and 10 (2.7%) had 3 APLs; LA and a-b2GPI IgA were the most prevalent (14% and 13.7% respectively). Other ACL and a-b2GPI subclasses were uncommon (<2.8%). Sixty-nine (17.2%) subjects had 109 events (57 venous, 35 arterial, 14 obstetric, and 3 glomerular thrombosis); APLS was diagnosed in 34 (49.3%). Higher number of APLs yielded increased thrombotic risk compared to none [OR of 6.6, 9.9, and 27.8 for 1, 2, and 3 respectively, all with p<0.0001]; triple APL positivity bore higher event risk than single [OR=4.2, p=0.047]. In the final model (table 1), SLE duration and hypertension contributed to thrombotic risk (p<0.0001, and p=0.055 respectively), whereas age, gender, smoking, history of nephrotic syndrome, and oral contraceptives did not. Presence of ACL (IgG or IgM) and LA significantly raised risk in the entire cohort, with variation at the ethnic group level, whereas addition of a-b2GPI IgG and IgM did not; a-b2GPI IgA independently contributed an additional 3-fold risk (p=0.001), for the entire cohort, as well as all individual ethnic subgroups. Inclusion of a-b2GPI-IgA in the consensus criteria would have established an APLS diagnosis in an additional 12 subjects (+17.4%, p=0.0005).
{kind=link}
Conclusions A-b2GPI IgA and LA were the most prevalent APLs in a contemporary multiethnic cohort of SLE patients. Higher numbers of APLs yielded higher thrombotic risk, and so did triple positivity compared to single. A-b2GPI IgA presence significantly enhanced event risk above and beyond clinical factors and all other APL subclasses.
Disclosure of Interest None declared