Article Text

Abstract
Background Eosinophilic granulomatosis with polyangiitis (EGPA) is a rare small-vessel vasculitis most commonly presents in adults with the average age of diagnosis is being 50 years. After the long-standing prodromal phase (asthma, allergic rhinitis, nasal polyposis) patients progress to eosinophilic phase which is marked by eosinophilia and pulmonary infiltrates and then to the vasculitic phase (1,2).
Objectives Herein, we present a child in the vasculitic phase of EGPA with a severe skin involvement, who was initially diagnosed and treated for cutaneous anthrax.
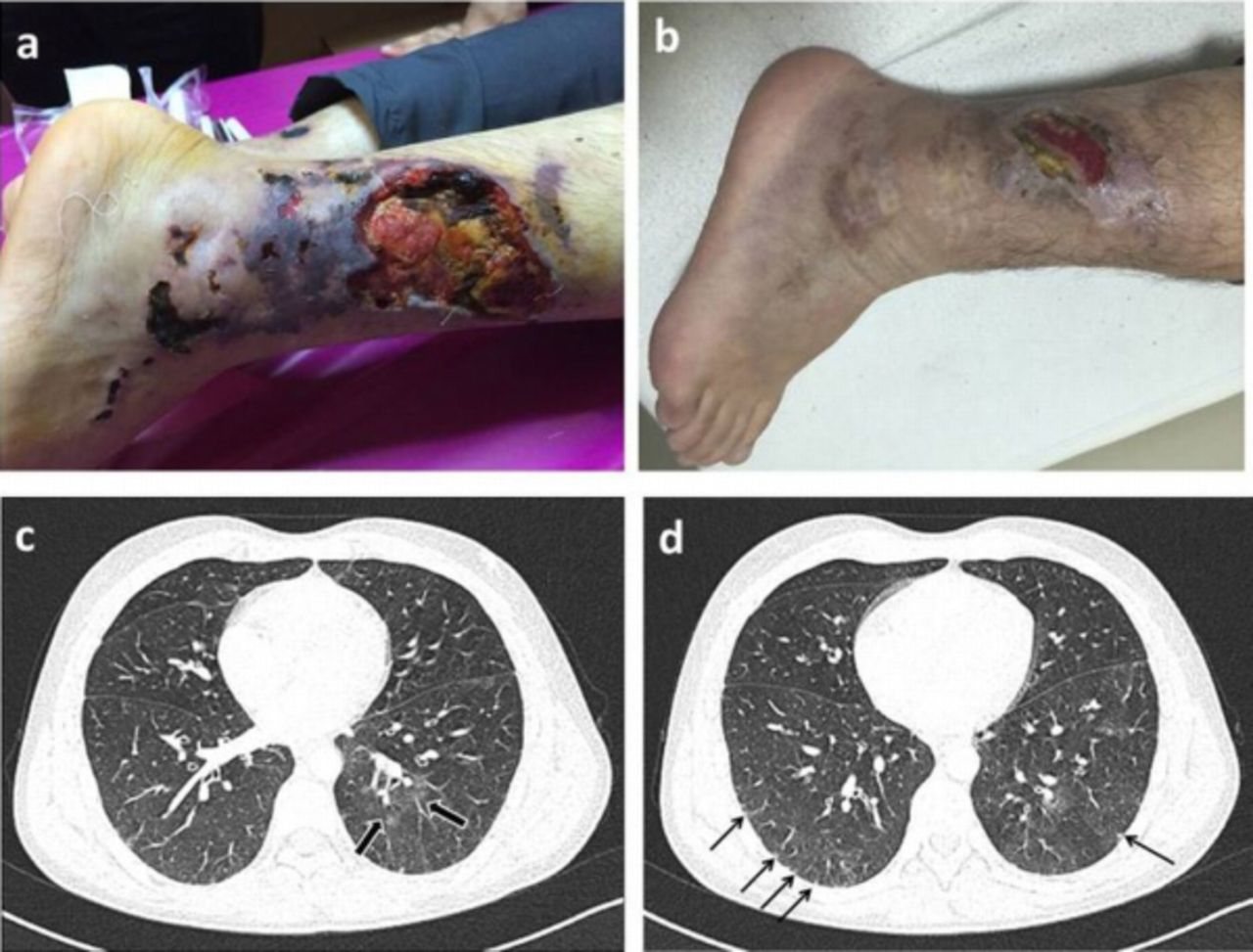
Results A 14-year-old male previously misdiagnosed as cutaneous anthrax was referred with a 2-month history of multiple wide and deep ulceronecrotic lesions in lower extremities, started after contact with animals (1a). Complete blood count (CBC) revealed anemia (hemoglobin: 8.5 g/dl, hematocrit: 26.9%), eosinophilia (4100/mm3) and thrombocytopenia (34000/mm3). Peripheral blood smear also revealed marked eosinophilia (42%). Infectious etiologies such as cutaneous anthrax, leishmaniosis, aspergillosis and nonspecific agents were excluded by gram staining, wound-blood-bone marrow cultures and serological investigations. Bone marrow aspiration was performed owing to the prominent eosinophilia, anemia and thrombocytopenia. However, the result was also pointing out eosinophilia without signs of eosinophilic leukemia. Although ANCAs were negative, the robust clinical manifestations concordant with EGPA (e.g. eosinophilia, increased Ig E level, history of asthma, vasculitic lesions) had led us to repeat the skin biopsy and search for lung involvement. Pulmonary high resolution computed tomography (HRCT) demonstrated bilateral ground glass opacity (figure 1c) and millimetric subpleural nodules (figure 1d). Skin biopsy revealed necrotizing inflammation without apparent granulomas and marked eosinophilic infiltrations in the extravascular areas. On the second day of hospitalization he developed deep vein thrombosis (DVT). A diagnosis of EGPA was established and intravenous methylprednisolone with low–molecular weight heparin were administered. Patient showed remarkable improvement of cutaneous lesions and DVT (Figure 1b).

{kind=link}
Conclusions Lack of awareness for EGPA among paediatricians as a consequence of limited childhood cases, results with diagnostic delay. Diagnosis of EGPA is challenging in the vasculitic phase and necessitates a detailed history that specifically questions the patient for asthma history. Coexistence of vasculitic lesions and eosinophilia associated with a prior history of asthma should lead to the consideration of EGPA in differential diagnosis.
Barut K, Sahin S, Kasapcopur O. Pediatric vasculitis. Curr Opin Rheum 2016;28:29–38.
Gendelman S, Zeft A, Spalding SJ. Childhood-onset eosinophilic granulomatosis with polyangiitis (formerly Churg-Strauss syndrome): a contemporary single-center cohort. J Rheumatol 2013;40:929–935.
Disclosure of Interest None declared