Article Text

Abstract
Background Several clinically relevant and validated assessment tools are currently used in psoriatic arthritis (PsA), but most have limitations when applied in usual care situations (eg, requirements for formal joint counts and laboratory tests). Easy-to-use composite indices are needed to assess PsA at initial and follow-up visits in the clinical practice setting. Currently used in other chronic rheumatic conditions, RAPID3 is a simple composite index of 3 measures (ie, physical function, pain, and patient global assessment) that can be calculated in 5-10 seconds (vs 114 seconds for DAS28) based on a patient self-report questionnaire completed in the waiting room.1
Objectives To assess the performance of RAPID3 vs DAS28 and other commonly used instruments in patients with PsA.
Methods Trial data from PRESTA2 (baseline [BL] only) and PREPARE3 (BL + wk 24) were analyzed. Correlations between RAPID3 and DAS28-CRP, CDAI, CPDAI, and DAPSA were analyzed using intraclass correlation coefficients (ICC; 95% CI). Treatment effect sizes were calculated for change from baseline to week 24 (PRESTA) and agreement in disease activity classifications compared at BL (PREPARE+PRESTA).
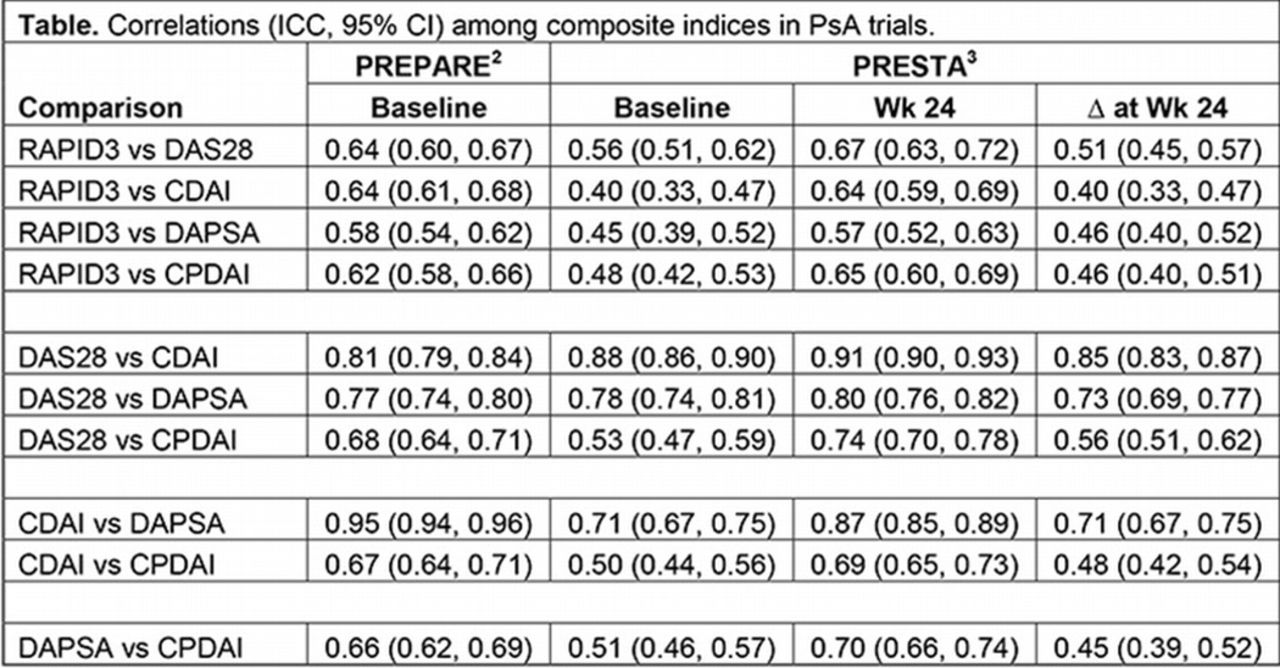
Results A moderate degree of correlation was found between RAPID3 and other composite indices (table). In PRESTA, RAPID3 was most closely correlated with DAS28-CRP (ICC, 0.56, 0.67, and 0.51 at BL, wk 24, Δ at wk 24) and CPDAI (0.48, 0.65, 0.46). DAS28-CRP was the most sensitive tool in detecting treatment changes from BL to wk 24 in PRESTA (effect size, -1.75), and DAPSA the least sensitive (-0.94); RAPID3 showed moderate sensitivity (-1.33). Many patients who met criteria for high, moderate, low, and near-remission disease activity categories for RAPID3 satisfied criteria for similar categories for DAS28-ESR (38%, PREPARE; 51%, PRESTA) and CDAI (52%; 59%) at BL.
{kind=link}
Conclusions In clinical trials of PsA, the performance of RAPID3 proved to be satisfactory relative to other composite indices. Although additional research is needed, RAPID3 may provide a practical tool for use in the routine clinical care of this condition.
References
Pincus T, et al. Bull NYU Hosp Jt Dis. 2009;67:211-25.
Sterry W, et al. BMJ. 2010;340:c147.
Mease PJ, et al. J Am Acad Dermatol. 2013;69:729-35.
Disclosure of Interest S. M. Reddy: None declared, J. U. Scher Grant/research support from: NIH, Arthritis Foundation, Consultant for: Janssen, Celgene, Novartis, Abbvie, A. Szumski Consultant for: Pfizer Inc, M.-A. Hsu Shareholder of: Pfizer Inc, Employee of: Pfizer Inc, L. Marshall Shareholder of: Pfizer Inc, Employee of: Pfizer Inc, H. Jones Shareholder of: Pfizer Inc, Employee of: Pfizer Inc, Y. Yazici Grant/research support from: BMS, Celgene, Genentech, Consultant for: BMS, Celgene, genentech, Employee of: Samumed