Article Text

Abstract
Background The head-to-head AMPLE (Abatacept versus Adalimumab Comparison In Biologic-Naïve RA Subjects With Background Methotrexate) study demonstrated comparable efficacy for SC abatacept and adalimumab in patients with RA.1 Anti-citrullinated protein antibodies (ACPA) are a known biomarker for RA and disease progression,2,3 but their predictive value for treatment outcomes is not well understood. Such information may serve as a predictor of treatment response in RA.
Objectives To examine the effect of abatacept and adalimumab on patient-reported outcomes (PROs) in patients grouped by baseline quartiles of anti-cyclic citrullinated peptide-2 (anti-CCP2; a surrogate for ACPA) antibody titre.
Methods The AMPLE study has been described.1 In this post hoc analysis of the AMPLE study, anti-CCP2–immunoglobulin (Ig) G titres in patient samples collected at baseline were determined by anti-CCP2 ELISA.4 PROs were assessed in anti-CCP2-positive patients divided into quartiles 1–4 based on increasing baseline titres. PROs analysed included: Patient Global Assessment (PGA), pain, fatigue, and SF-36 physical (PCS) and mental component summary (MCS) scores. Mean change from baseline was calculated with adjustment by analysis of covariance, with treatment as a factor; baseline values and DAS28 (CRP) stratification were covariates.
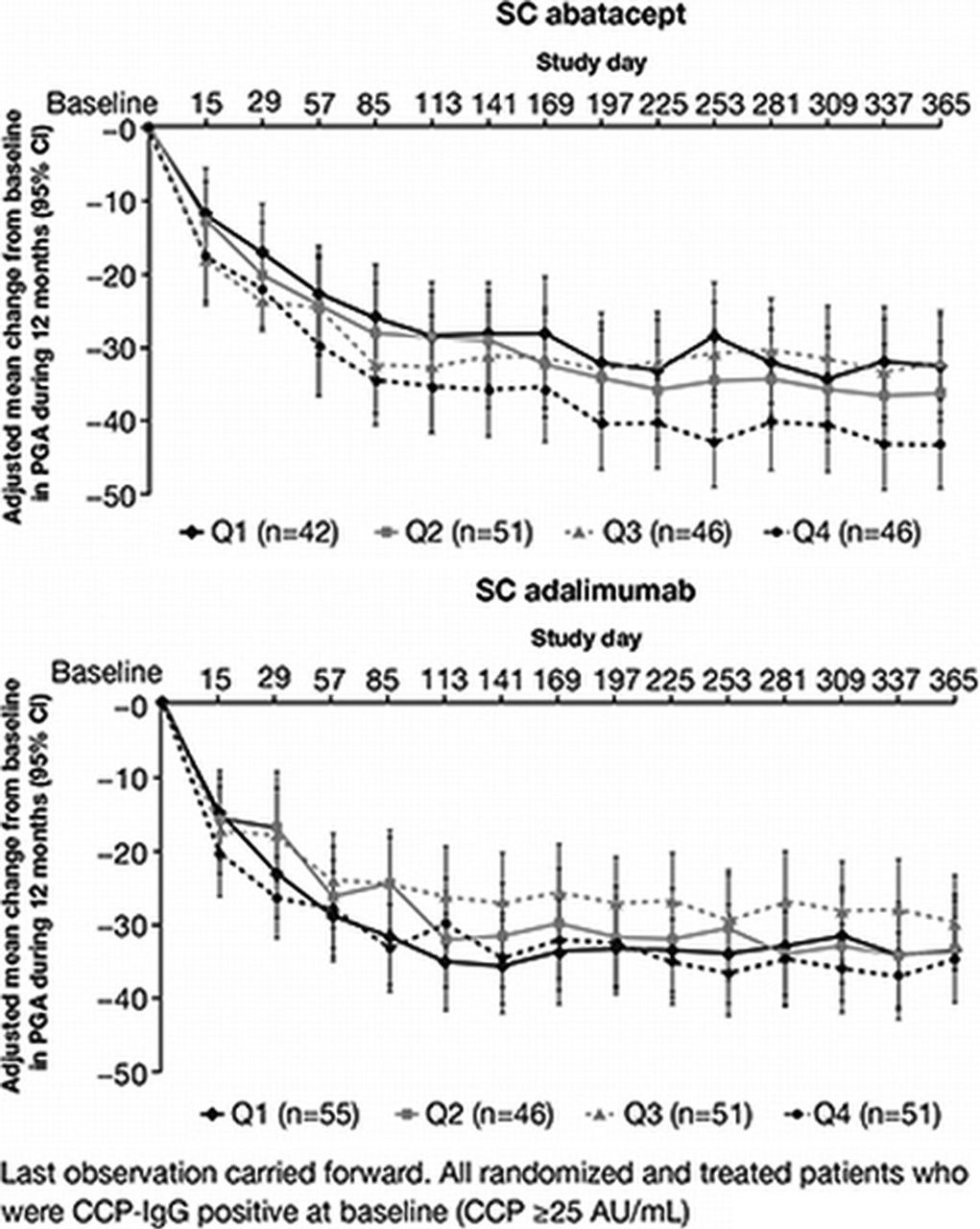
Results There were 97 patients per quartile. Quartile limits were (AU/mL): Q1=28–235; Q2=236–609; Q3=613–1046; Q4=1060–4894. The number of patients per treatment group in each quartile were (abatacept, adalimumab): Q1=42, 55; Q2=51, 46; Q3=46, 51; Q4=46, 51. Higher anti-CCP2 antibody titre at baseline was associated with numerically better treatment response, as assessed by PGA, pain and SF-36 PCS for abatacept: mean changes from baseline were greater for Q4 than Q1–3 in patients receiving abatacept; such differences were not as pronounced with adalimumab. No consistent differences were evident in fatigue and SF-36 MCS based on quartile for abatacept; however, lower baseline anti-CCP2 titre (Q1) was associated with better responses in the adalimumab group for these PROs.
{kind=link}
Conclusions A pattern of more robust improvement was observed for patients receiving abatacept, but not adalimumab, among the highest anti-CCP2 quartiles with respect to several PROs: PGA, pain, and SF-36 PCS scores. These findings are consistent with those on clinical parameters, where greater changes in DAS28 (CRP) and HAQ-DI scores were observed for patients in the highest anti-CCP2 titre quartile receiving abatacept but not adalimumab.
References
Schiff M, et al. Ann Rheum Dis 2014;73:86–94.
Verpoort KN, et al. Arthritis Rheum 2006;54:3799–808.
van der Woude D, et al. Ann Rheum Dis 2010;69:1554–61
Anti-CCP2 ELISA, Euro Diagnostica. http://www.eurodiagnostica.com/upload/files/fileLibrary/ProductSheet_CCPlus_Screen120504.pdf. Accessed 15 Jan 2015
Disclosure of Interest J. Sokolove Grant/research support from: Bristol-Myers Squibb, M. Schiff Grant/research support from: UCB, Consultant for: AbbVie, Amgen, Antares, Bristol-Myers Squibb, Eli Lilly, Horizon, Johnson and Johnson, Novartis, Novo Nordisk, Pfizer, Roche, UCB, Speakers bureau: AbbVie, R. Fleischmann Grant/research support from: AbbVie, Amgen, Astellas, AstraZeneca, Bristol-Myers Squibb, Celgene, Dynavax, Genzyme, Janssen, Eli Lilly, Merck, Novartis, Pfizer, Roche, sanofi-aventis, UCB, Xoma, Consultant for: AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Celgene, Janssen, Eli Lilly, Pfizer, Roche, sanofi-aventis, UCB, M. E. Weinblatt Grant/research support from: Bristol-Myers Squibb, Crescendo Bioscience, UCB, Consultant for: Bristol-Myers Squibb, Crescendo Bioscience, UCB, AbbVie, Roche, Janssen, Pfizer, Lilly, Amgen, V. Strand: None declared, S. E. Connolly Shareholder of: Bristol-Myers Squibb, Employee of: Bristol-Myers Squibb, M. A. Maldonado Shareholder of: Bristol-Myers Squibb, Employee of: Bristol-Myers Squibb, S. Patel Shareholder of: Bristol-Myers Squibb, Employee of: Bristol-Myers Squibb, E. Alemao Shareholder of: Bristol-Myers Squibb, Employee of: Bristol-Myers Squibb, W. H. Robinson: None declared