Article Text

Abstract
Background The Dutch cardiovascular risk management (CV-RM) guideline considers rheumatoid arthritis (RA) an independent risk factor for cardiovascular disease (CVD), for which CV-RM is necessary.
Objectives To investigate the effect of CV-RM interventions (blood pressure lowering therapy and lipid-lowering therapy) on the 10-year CV risk in patients with RA.
Methods Consecutive RA patients visiting Reade, a large outpatient rheumatology clinic, were included in this study. CV risk screening was performed at baseline, after one and two years, and included a lifestyle questionnaire, physical examination, laboratory investigations and assessment of the 10-year CV risk. The Dutch CVRM guideline classifies a risk <10% as low, between 10% and 20% as intermediate and a risk ≥20% as high (1). Patients with a history of CVD were classified as high risk. The results of the CV screening were communicated to the general practitioner, who decided whether or not to start preventive medication.
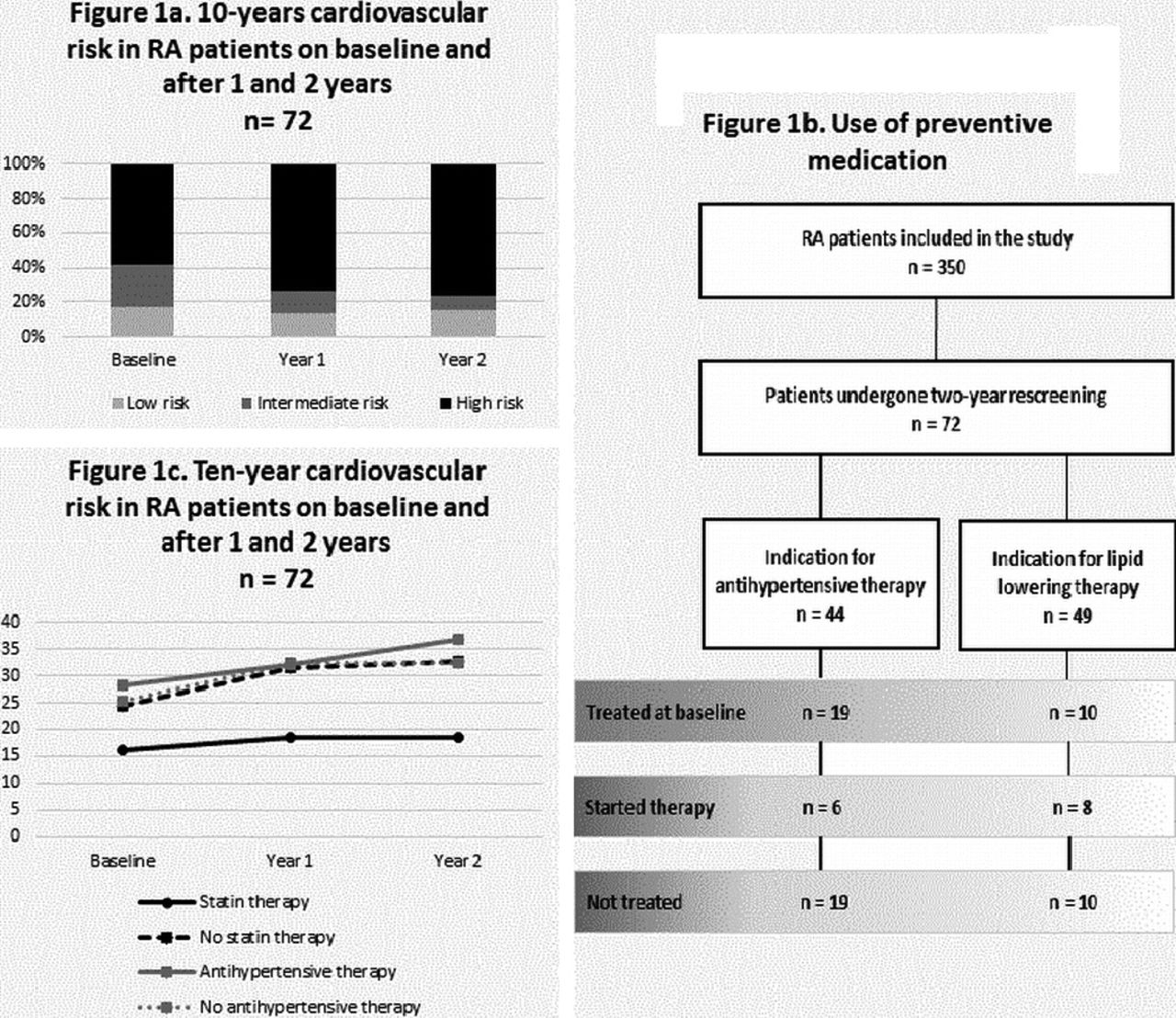
Results In total, 350 patients were included in the Amsterdam CV-RM cohort at the time of analysis. Seventy-two patients had undergone two rescreening's. Of those patients, 76% were female, the mean age at baseline was 62 years and 5 had a history of CVD. After two years, the overall 10-year risk increased significantly from 21.7% to 26.2% (p<0.01). Five new cases of CVD occurred, all in the high risk group. At baseline, 42 patients (58%) had a high CV risk, which increased to 55 (76%) at the second rescreening after correction for age (figure 1a). During follow-up a total of 44 patients had an indication to use antihypertensive therapy. However, only 25 of them used or started antihypertensives whereas in 19 patients antihypertensive therapy wasn't given at all (figure 1b). In both groups (treated versus not treated), 10-year CV risk increased. However, the increase in CV risk was lower in the group that started antihypertensive therapy in the first year (3.6% vs. 6.9%) (figure 1c). The indication for lipid lowering therapy was present in 49 patients. Eighteen used or started statins whereas 31 patients did not receive lipid lowering treatment despite having an indication. In the statin starters, the average increase in 10-year CV risk was 2.7%, versus 8.6% in patients that had an indication for statin use but did not receive lipid lowering therapy.
{kind=link}
Conclusions Despite implementing CV-RM in RA patients, we found an unexpected overall increase in 10-year CV risk. This might be a reflection of undertreatment of both hypertension and dyslipidemia as many patients who had an indication to use preventive medications do not receive adequate treatment, despite of repeated screening. Obviously, CV-RM guidelines are poorly performed in RA patients and need to be optimized.
References
Dutch Multidisciplinary Guideline “Cardiovascular risk management” (Second Revision), Huisarts Wet 2012;55:14-28.
Disclosure of Interest None declared