Article Text

Statistics from Altmetric.com
Tumour necrosis factor inhibitor (TNFi) treatment in patients with rheumatoid arthritis is more effective when combined with methotrexate (MTX).1–3 However, little is known about which MTX dose to use. With great interest, we read the article by Burmester et al4 on the efficacy and safety of ascending MTX doses with adalimumab. This randomised double-blind study showed comparable results for adalimumab with 10 and 20 mg MTX, in MTX naive patients. Because of the potential side effects, it is often preferred to use MTX doses as low as possible. Therefore, the following questions arise: what happens in daily practice with MTX plus adalimumab, where most patients are not MTX naive when starting TNFi, and are the results the same for etanercept and infliximab?
Data were collected within the Dutch RhEumatoid Arthritis Monitoring (DREAM) registry between 2003 and 2012. Patients starting their first TNFi in combination with MTX were included in the study. Treatment effectiveness was analysed using disease activity score in 28 joints (DAS28) and health assessment questionnaire disability index (HAQ-DI) with linear mixed models for 1 year and long-term drug survival was analysed using Cox regression. Both were corrected for confounders.
Of the 1331 patients in the DREAM cohort starting TNFi plus MTX (551 adalimumab, 610 etanercept, 154 infliximab and 16 others), 430 started with adalimumab and had complete data. MTX should be started at 10–15 mg weekly, which can be increased to 20–25 mg. In daily practice, these four MTX doses are most frequently used starting TNFi and therefore analysed (n=371). The patient characteristics are presented in table 1.
Adalimumab and methotrexate (MTX) data divided into four groups at start of adalimumab (Ada)
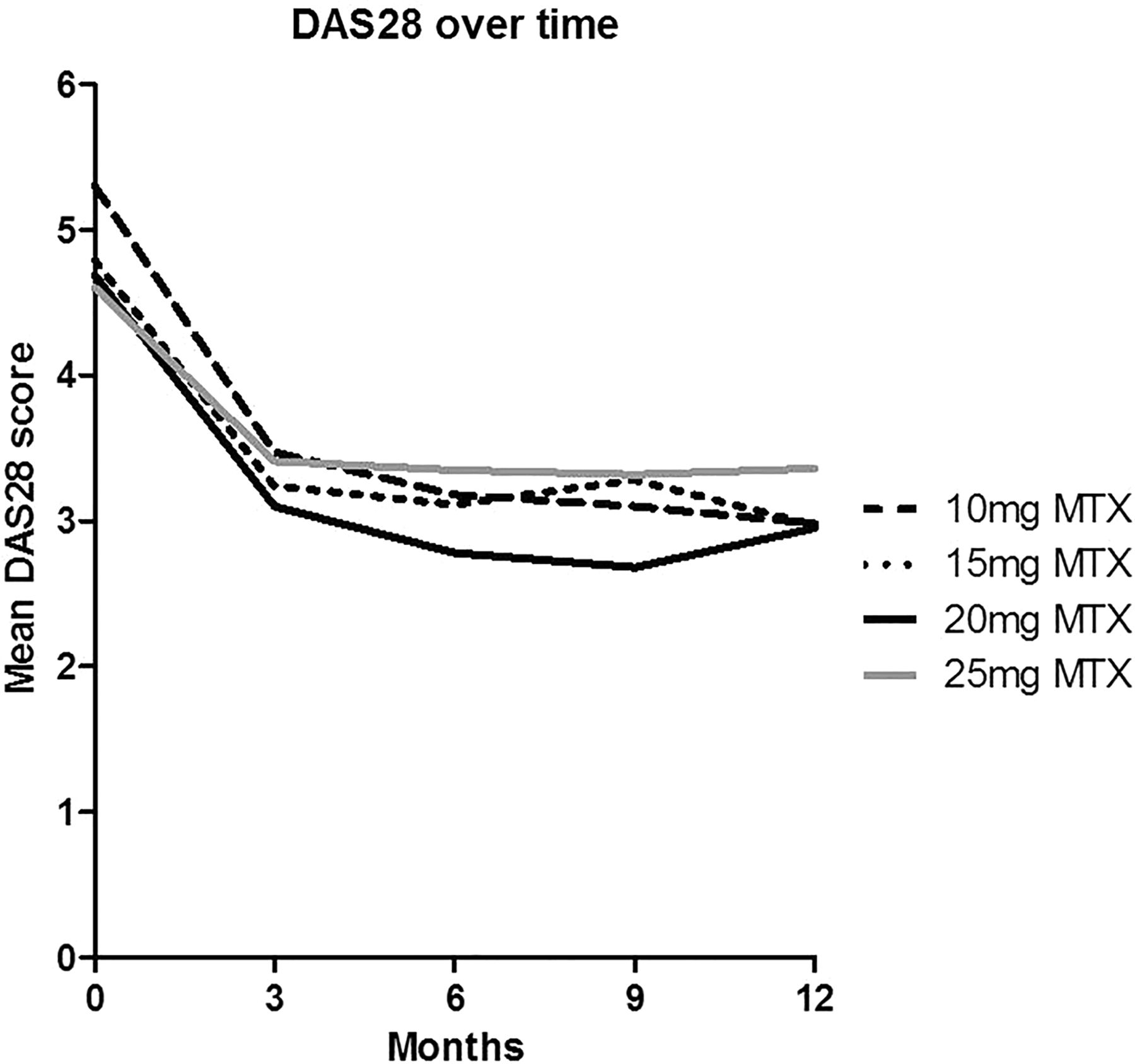
There were no significant differences between the MTX dose groups in DAS28 scores over time, except that the 25 mg MTX group had a worse DAS28 over time than the 15 mg (β=−0.29; 95% CI=−0.53 to −0.05) and 20 mg (β=−0.54; 95% CI=−0.80 to −0.28) MTX group (see figure 1). The HAQ-DI over time presented the same trend. There are significant differences in the 9-year TNFi drug survival between the groups: 25 mg MTX had a significantly worse drug survival than 10, 15 and 20 mg MTX.
{kind=link}
Mean DAS28 over time. DAS28, disease activity score in 28 joints; MTX, methotrexate.
Next to adalimumab, etanercept and infliximab are often used in daily practice in combination with 10, 15, 20 or 25 mg MTX (n=396 and n=92, respectively). There were no significant differences in DAS28 over time. However, also in these groups, there were significant differences in drug survival: 25 mg MTX had worse long-term drug survival than 10, 15 and 20 mg MTX.
Focussing on the 10 and 20 mg MTX groups in combination with adalimumab (studied by Burmester et al), there are also no significant differences between these groups in daily practice. The same was found for etanercept and infliximab. However, patients who start with adalimumab while on 25 mg MTX, which is common in daily practice, have a significantly worse DAS28 over time and drug survival of the TNFi. This could be a more severe group of patients that can tolerate 25 mg MTX but still have moderate to high disease activity. In conclusion, our data partly support the findings of Burmester et al and suggest that patients in the 10 and 15 mg group do not need a higher MTX dose at start with a TNFi treatment.
Footnotes
-
Contributors All authors are responsible for the work presented in this manuscript. They were involved in at least one of the following: conception and design, acquisition of data, statistical analysis and interpretation of data. All authors were involved in drafting the manuscript and revising the manuscript critically for important intellectual content and have given final approval of the version to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval According to Dutch regulations, the DREAM register does not require ethics approval because no additional data – other than data used for monitoring daily practice – are collected.
-
Provenance and peer review Not commissioned; internally peer reviewed.