Article Text

Statistics from Altmetric.com
There is accumulating evidence that periodontitis is linked to rheumatoid arthritis (RA) and that this may be due to the pathogen Porphyromonas gingivalis possessing a peptidyl arginine deiminase (PPAD). This apparently unique bacterial enzyme is capable of producing citrullinated bacterial or host proteins which could break tolerance leading to the generation of autoantibodies in RA.1 We have previously shown that PPAD is autocitrullinated and there is an increased antibody response to PPAD in RA, which was due to reactions with autocitrullinated epitopes on the PPAD molecule.2 We were therefore interested to read the article by Konig et al3 in which they confirm our findings that full-length recombinant PPAD is autocitrullinated, but showed that a truncated and secreted form of PPAD purified from supernatants of P. gingivalis cultures was not autocitrullinated. From this they concluded that autocitrullination was a feature of cloning, which would not occur in nature. However, growing bacteria in culture is not natural either. In vivo, at the site of infection, bacteria would be lysed by the immune response and bacterial proteins, including PPAD, potentially citrullinated by PPAD itself, or by host deiminases such as PAD2, and exposed to the immune system.
The bulk of Konig et al's report was devoted to their finding that there was no citrulline-specific antibody response to their form of autocitrullinated full-length PPAD in patients with RA. This was in complete contrast to our own finding of raised antibody levels to autocitrullinated PPAD in 25% of patients with RA. The reason for this discrepancy is unknown, though it is well known that citrullinated antigens in the form of whole proteins do not perform reproducibly in ELISA assays. Accordingly, in our original study we went on to test antibodies to synthetic peptides spanning the length of PPAD with all arginines substituted with citrullines.2 We found antibodies to three immunodominant citrulline-specific epitopes (designated CPP3, CPP5 and CPP8) with diagnostic sensitivities ranging from 15% to 40% in RA sera.
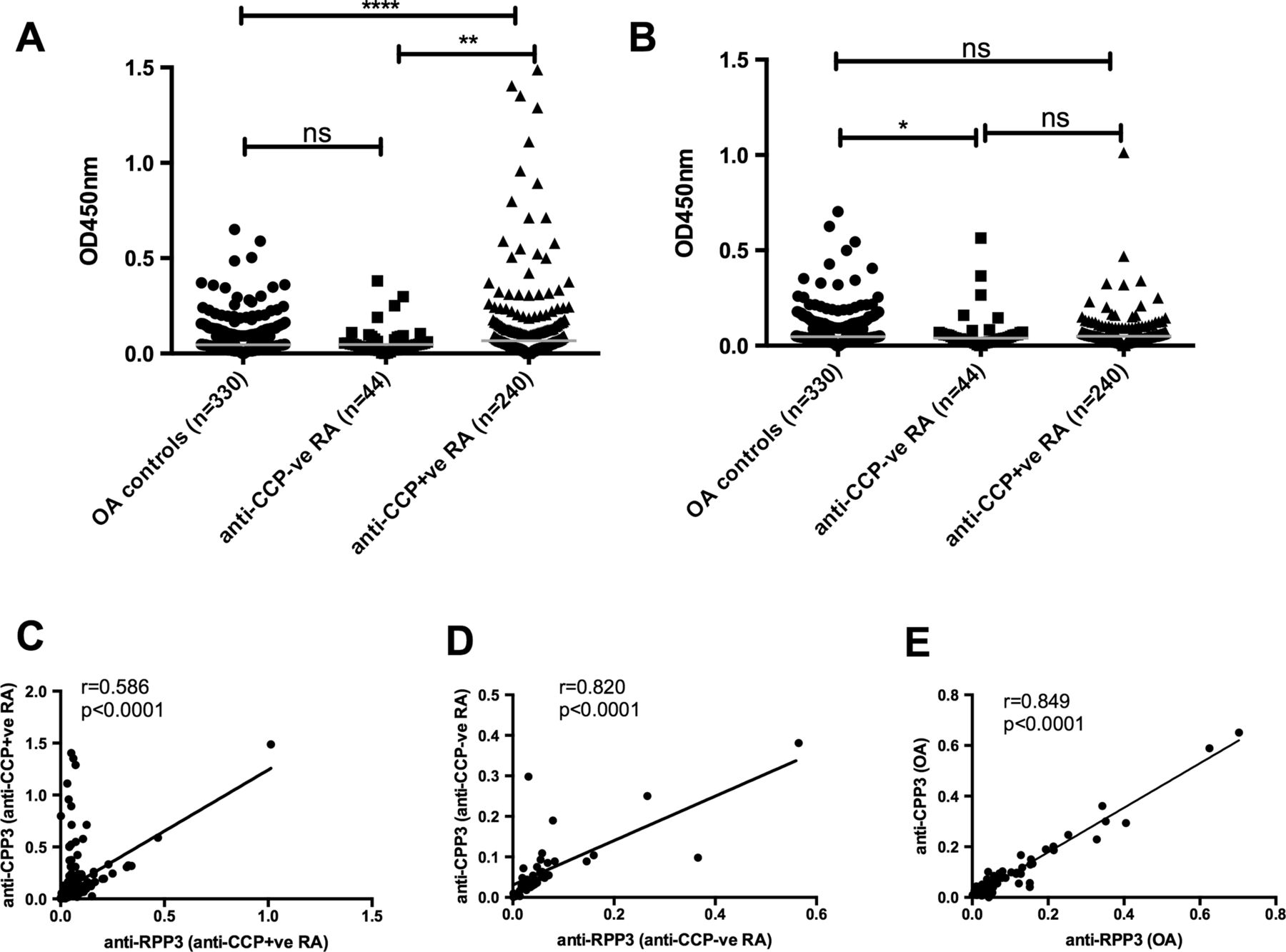
In the current study, we examined 284 serum samples from patients with well documented RA compared with 330 osteoarthritis (OA) controls from a previously published cohort,4 using the CPP3 (CAKTDSYWT-Cit-DYTGWFAMYDC) peptide, with a citrulline at position R129, together with its corresponding arginine-containing control peptide (RPP3). Importantly, this specific residue was demonstrated by mass spectrometry to be autocitrullinated in Konig et al's study. Antibodies to CPP3 were significantly elevated in the anti-cyclic citrullinated peptide antibody (anti-CCP) positive RA serum samples with no significant increase in antibody levels to the control peptide (figure 1A, B). By plotting the correlation between antibodies to CPP3 and RPP3, it can be clearly seen that approximately 15% of the anti-CCP positive RA serum samples react preferentially with citrulline-containing epitopes, as indicated by the points above the regression line (figure 1C). This citrulline-specific reactivity was not seen with the anti-CCP negative serum samples or with the OA controls (figure 1D, E). Similar findings of a citrulline-specific antibody response to CPP3 were found in a Swedish study of 200 patients with RA and 100 controls, presented at the 2013 American College of Rheumatology meeting.5 These results are in contrast to the findings of Konig et al who showed an almost perfect correlation between binding to autocitrullinated whole PPAD and the uncitrullinated mutant control in RA.
{kind=link}
Antibodies to citrullinated peptidyl arginine deiminase (PPAD) peptide (CPP3) and uncitrullinated PPAD peptide (RPP3) in serum of patients with rheumatoid arthritis (RA) and controls with osteoarthritis (OA). Antibodies to (A) CPP3 and (B) RPP3 in OA controls, anti-CCP negative RA and anti-CCP positive RA. The grey lines indicate median reactivity for each group. Mann-Whitney U test was used to calculate p values for differences between the groups (n.s.=no significant difference, *p<0.05 and **p<0.01, ***p<0.001). (C) Spearman correlation of anti-CPP3 and anti-RPP3 in anti-CCP positive RA, (D) in anti-CCP negative RA and (E) in OA controls.
Therefore we argue that it is premature to claim that: “PPAD autocitrullination is not the underlying mechanism linking periodontitis to RA”.3 The ELISA used by Konig et al was clearly not detecting antibodies to citrullinated epitopes on PPAD, and importantly, their results were not confirmed using peptide ELISAs. We suggest that PPAD remains a credible candidate for inducing an antibody response to citrullinated proteins in RA—be it through autocitrullination, citrullination by human PAD enzymes, or citrullination of other bacterial and/or human proteins.
Footnotes
Contributors A-MQ: study design, acquisition, analysis and interpretation of data, manuscript preparation. KL: study design, interpretation of data, manuscript preparation. JP: study design, interpretation of data, manuscript preparation. TRM: study design, data acquisition, interpretation of data, manuscript preparation. PJV: study design, analysis and interpretation of data, manuscript preparation. All authors have read and approved the final manuscript. PJV had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Competing interests None.
Ethics approval The Institutional Review Boards at the participating rheumatology, orthopaedic and primary care clinics in four US Veterans Affairs Medical Centres and a single academic coordinating centre.
Provenance and peer review Not commissioned; internally peer reviewed.