Article Text

Statistics from Altmetric.com
With interest we read the article by Hecht et al1 who studied the associations of anticitrullinated peptide antibodies (ACPA) and rheumatoid factor (RF) with bone erosions in rheumatoid arthritis (RA). The background of this study was that ACPAs directed against citrullinated vimentin induce differentiation of osteoclasts, indicating that ACPA has a direct effect on bone resorption.2 No biological data are available on whether RF also affects bone cells and, given the overlap between ACPA-positivity and RF-positivity, the authors wanted to distinguish the association between RF and bone erosions from the association between ACPA and bone erosions. In a cross-sectional study, high-resolution peripheral quantitative CT (HR-pQCT) images of metacarpophalangeal (MCP) 2–4 joints of 238 patients with RA were made and groups of patients with different combinations of autoantibodies were compared. The authors observed mainly differences in erosive burden in patients with both antibodies compared with those without antibodies. In a subgroup analysis, they also reported a higher erosive burden in ACPA+/RF+ patients compared with ACPA+/RF− patients. Based on their findings the authors suggested that RF may act as an enhancer of bone loss in ACPA-positive patients.
HR-pQCT is an interesting tool that admits measuring the three-dimensional size of erosions in detail. Conventional hands and feet radiographs have the advantage of their availability to study higher number of patients and evaluate more joints than is possible with HR-pQCT. We hypothesised that if RF acts additively on the erosive disease burden in ACPA-positive patients with RA, this should also be detectable by conventional radiographs. Therefore, we performed the present analysis to further increase the comprehension of the effects of both ACPA and RF on bone destruction in RA.
Two large European RA cohorts that both included and followed patients in the era before the widespread introduction of biologics were used. The Leiden Early Arthritis Clinic (EAC) cohort from the Netherlands included 678 patients with RA, fulfilling the 1987 American College of Rheumatology (ACR) criteria, between 1993 and 2006.3 In total, 3540 sets of radiographs of hands and feet were made with yearly intervals during 7-year follow-up and were scored by one experienced reader using the Sharp-van der Heijde scoring (SHS) method (intraclass correlation coefficient (ICC) 0.91). The second data set is the Better Anti-Rheumatic PharmacOTherapy (BARFOT) cohort.4 Here, 715 Swedish patients with early RA, fulfilling the ACR criteria and a disease duration ≤1 year, underwent radiographs of hands and feet at inclusion and after 1, 2 and 5 years (2483 sets of X-rays in total). These were SHS scored by two readers (between reader ICC for SHS at baseline and after 2 years, respectively, 0.93 and 0.94). For both cohorts only the total erosion scores were evaluated. ACPA (anti-CCP2) and RF (IgM-RF) were determined at baseline. Analyses of the erosion scores were done using multivariate normal regression analyses, adjusting for age, gender and treatment strategies, as described previously.3 ,5 ,6
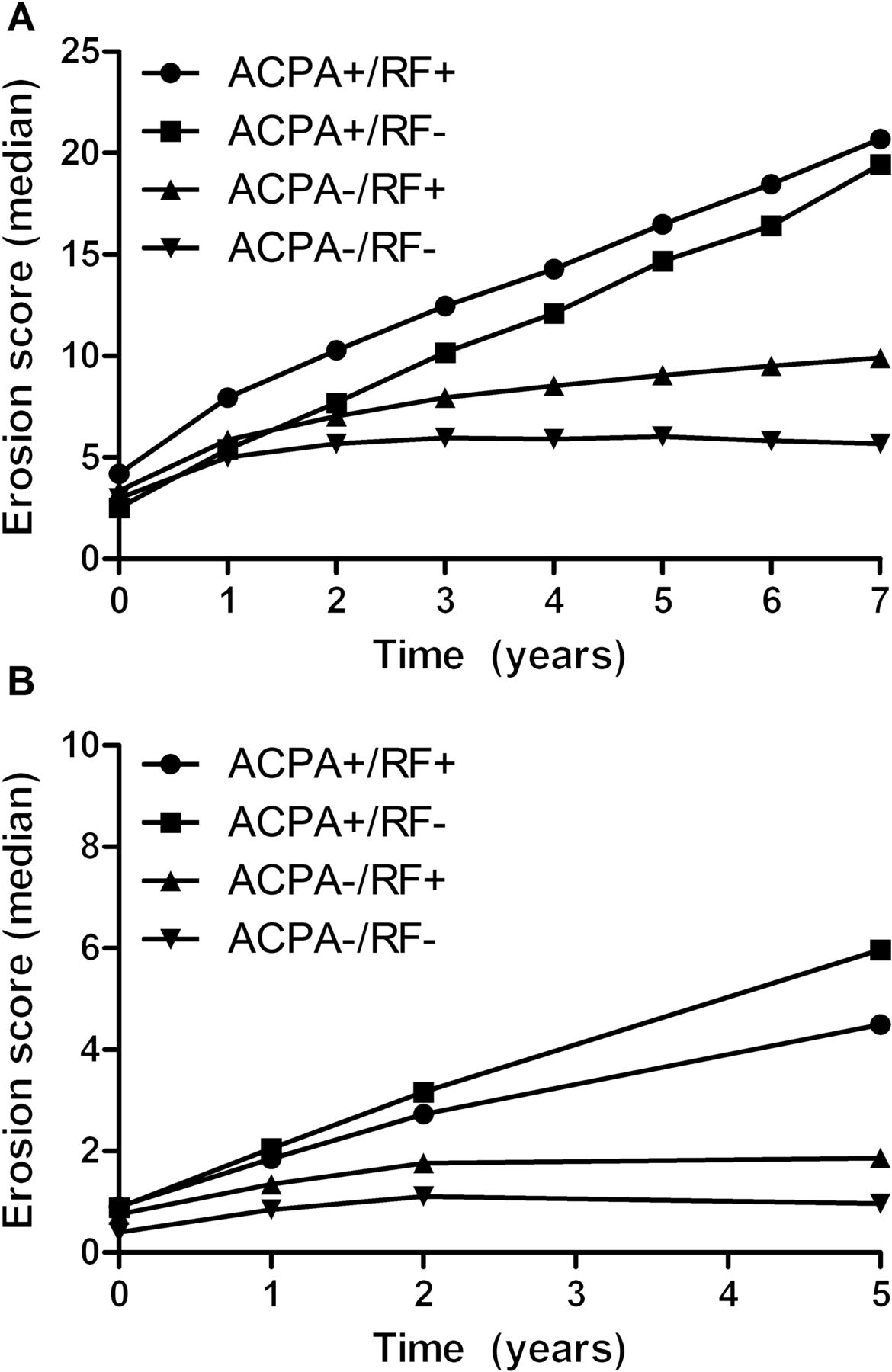
The frequency of patients positive for RF, ACPA or both is presented in table 1, and frequencies were similar in both groups. In accordance with Hecht et al, we compared the four serostatus groups with the ACPA−/RF− group as reference, here, for the erosion scores by SHS. Within the EAC cohort, all three seropositive groups had higher erosive progression rates: ACPA−/RF+ β=1.07; ACPA+/RF− β=1.15; and ACPA+/RF+ β=1.13, all p<0.001 (figure 1A). A β of 1.15 indicated a 1.15 higher estimated rate of erosive destruction per year, which equals 1.15^7=166% more severe joint erosion score after 7 years. When comparing the ACPA+/RF+ and ACPA+/RF− groups, hence evaluating the effect of RF in ACPA-positive patients, we observed no difference (p=0.33). Similar results were obtained when the analyses were performed on the BARFOT cohort. Compared with the ACPA−/RF− patients, ACPA−/RF+ patients had higher erosion scores at all points in time (p=0.017). The presence of ACPA+/RF− and ACPA+/RF+ both showed more severe erosive progression than ACPA−/RF− (β=1.23 and β=1.17, respectively, both p<0.001; figure 1B). Also here, when comparing the ACPA+/RF− with ACPA+/RF+ patients, no significant differences were observed (p=0.12).
Patient characteristics
{kind=link}
Erosion scores, assessed by the Sharp-van der Heijde method (SHS), during the disease course according to the presence of anticitrullinated peptide antibodies (ACPA), rheumatoid factor (RF) or both in patients with RA from the Leiden Early Arthritis Clinic (EAC) (A) and Better Anti-Rheumatic PharmacOTherapy (BARFOT) (B) cohorts. Presented are predicted median erosion scores (by the multivariate normal regression model, controlled for age, sex and treatment strategy), scored using the SHS in 678 patients with RA over 7 years from the Leiden EAC (A) and in 715 patients with RA over 5 years from the BARFOT (B) cohort. The erosion scores between the ACPA+/RF+ and ACPA+/RF− groups did not differ either within the Leiden EAC (p=0.33) or the BARFOT (p=0.12) cohort.
In conclusion, when evaluating in total 1393 patients with RA and 6023 sets of radiographs, we did not find that RF gives an additive effect on bone erosions in ACPA-positive patients. In contrast with the report by Hecht et al, we demonstrated that RF in ACPA-negative patients was associated with more severe erosive disease. The results from our two cohorts followed longitudinally are remarkably similar. Although it is tempting to speculate on an immune-enhancing effect of RF, more observational studies are needed to further unravel the association of RF with erosive disease in both ACPA-positive and ACPA-negative RA.
Footnotes
Contributors All authors contributed to the study design, acquisition of data, analysis and interpretation of data and manuscript preparation.
Funding This work was supported by a Vidi-grant of the Netherlands Organisation for Scientific Research, BTCURE and Masterswitch, the Swedish Rheumatism Association and the regional agreement on medical training and clinical research (ALF) between Stockholm County Council and Karolinska Institutet.
Competing interests None.
Patient consent Obtained.
Ethics approval Local ethical committees approved the study.
Provenance and peer review Not commissioned; internally peer reviewed.
Linked Articles
- Electronic pages
- Clinical and epidemiological research