Article Text

Abstract
Background Estimation of the lifetime risk of joint replacement surgery is an emerging field in musculoskeletal epidemiology. While global burden of disease data are valuable for understanding disease incidence and prevalence and the relative impact of a disease on patients' lives [1], lifetime risk provides an alternative method of quantifying population disease burden and associated healthcare utilisation [2].
Objectives Our primary aim was to investigate lifetime risk of total hip (THR) and total knee (TKR) replacement surgery. As changes in the lifetime risk of joint replacement over time could be mediated by environmental, health system or patient and clinician-level factors, we also sought to describe temporal trends in incidence by relevant factors which may impact utilisation of these procedures.
Methods We analysed a population-based cohort of patients who received a primary THR or TKR in Victoria from 1999 to 2008. Hospital separations and life tables were used to estimate lifetime risk. Temporal changes in THR and TKR incidence were examined according to healthcare setting, socio-economic status and geographic location.
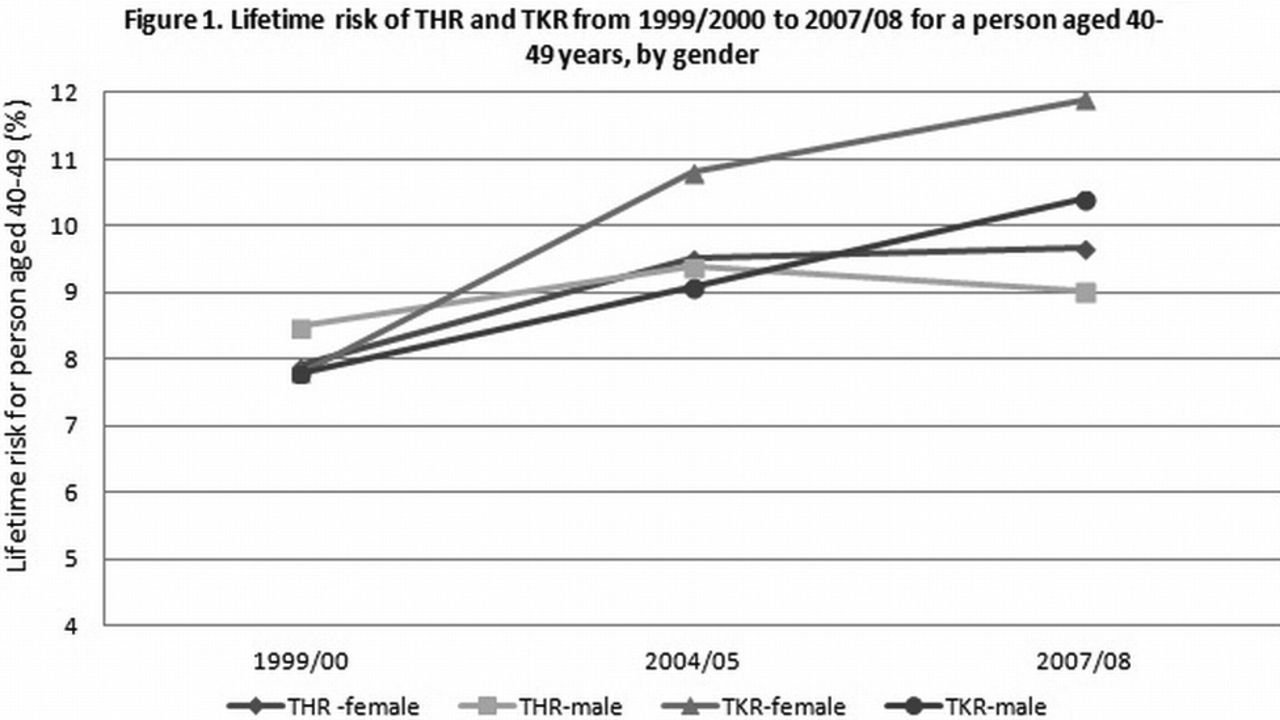
Results We identified 45,775 patients receiving a primary THR and 43,570 receiving a primary TKR over the time period. The lifetime risk by year for each procedure for a person aged 40-49 years is reported in Figure 1. There was a greater increase in the lifetime risk of TKR when compared to THR, particularly for females. We also identified an increasing number of both procedures in private hospitals (increase in THR of 0.14 per 1000 and TKR of 0.60 per 1000), for people in middle socio-economic groups (increase in THR of 0.11 per 1000 and TKR of 0.07 per 1000) and in rural areas (increase in THR of 0.24 per 1000 and TKR of 0.70 per 1000). With the exception of the increase in THRs in the middle socio-economic group, increases were more pronounced for TKRs over the time period.
{kind=link}
Conclusions The larger increase in lifetime risk of TKR over the study period could be partly attributed to the ageing population, with more people aged over 80 receiving TKRs, increased rates of sporting injuries and rising rates of obesity [3–7]. The larger increase in incidence for patients in regional areas could relate to greater previously unmet need, a higher burden of OA in rural areas related to higher rates of obesity and manual occupations and the increased provision of orthopaedic services in rural areas over the past decade. The lifetime risk of THR performed on women was found to be similar to males, despite a higher burden of hip OA. Disparities in surgery by socio-economic status and gender warrant further investigation.
References
-
Murray CJ. Bull World Health Organ 1994;72:429-45.
-
Culliford DJ, et al. Osteoarthritis Cartilage 2012;20:519-24.
-
Andrew NE, et al. Injury 2012;43:1527-33.
-
Tjoumakaris FP, et al. J Knee Surg 2012;25:403-6.
-
Hart DJ,et al. Arthritis Rheum 1999;42:17-24.
-
Grotle M, et al. BMC Musculoskelet Disord 2008;9:132.
-
Wang Y, et al. Rheumatology (Oxford) 2013 Jun;52(6):1033-41.
Disclosure of Interest : None declared
DOI 10.1136/annrheumdis-2014-eular.1058