Article Text

Abstract
Background Achieving sustained remission in Rheumatoid Arthritis (RA) is more important than achieving point remission, albeit more challenging, and likely to have greater impact on long-term outcomes of disease such as orthopaedic surgery (OS).
Objectives To examine baseline predictors and OS, a surrogate marker of joint destruction, in RA patients with sustained disease activity score (DAS) remission over the first 3 years (3yrRem).
Methods Using a single mode of data collection, 1465 DMARD naïve patients were recruited into the Early RA Study (ERAS, 9 centres, 1986-1998) & 1236 patients into the Early RA Network (ERAN, 23 centres, 2002-2012). Standard clinical, radiological & laboratory measures were performed yearly for a maximum 25 & 10yrs (median 10 & 3yrs respectively). 3yrRem was defined as persisting DAS of ≤3.2 at 6 months (following treatment-onset), 1, 2 & 3 yrs. In-patient hospital episodes were recorded yearly, including OS. Major OS (M-OS) included large total joint replacements (mainly hips/knees) & intermediate OS (I-OS) included hand/foot surgery. Source data of all OS included clinical datasets (patient reports & medical records from 1986) & national data from Hospital Episode Statistics & the National Joint Registry. Length of follow up was based on the National Death Registry. Treatment regimens followed guidelines of the era, mainly conventional DMARDs, +/− steroids & latterly biologics.
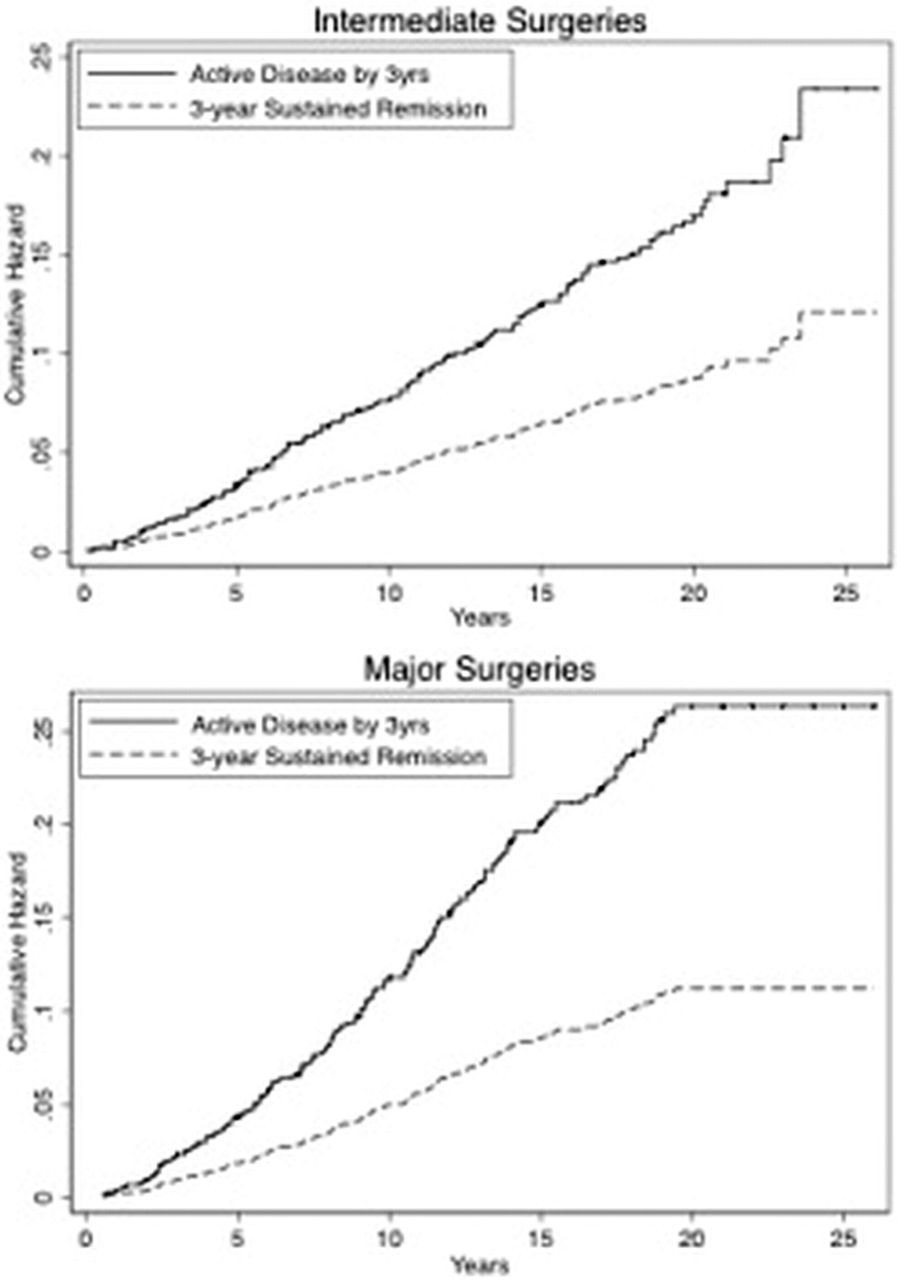
Results Out of 2701 patients, 154 (5.7%) were in 3yrRem following onset of treatment. In Logistic regression analysis, baseline DAS was the single clinical/laboratory predictor (OR 0.60, p<0.001) for achieving 3yrRem, along with male gender (OR 2.57, p<0.001). In Cox regression models controlling for age at disease-onset, gender as well as baseline clinical/laboratory variables, the likelihood of having M-OS was more than halved if in the 3yrRem group (HR 0.43, p<0.05). There was a similar trend for I-OS, although non-significant (p=0.07), suggesting that those in sustained remission also had a lower risk of this surgery. Fig1 shows the cumulative hazard for M-OS & I-OS in those with 3yrRem versus those with active disease. Male gender, body mass index (BMI), erythrocyte sedimentation rate (ESR), erosions & haemoglobin (HB) at baseline were all significant predictors of I-OS, while age at disease-onset, BMI, erosions & HB were all significant predictors of M-OS (p<0.05).

{kind=link}
Cumulative hazard plots of intermediate (a) and major (b) surgery by DAS category.
Conclusions Baseline DAS was the single predictive clinical/laboratory variable for achieving 3yrRem, along with male gender. The results highlight the importance of early DAS remission with early & intensive medical intervention to increase the likelihood of sustained remission in later years. Patients achieving 3yrRem had significantly lower incidence of M-OS compared to those with active disease. Possible explanations for differences seen between M-OS and I-OS include the effect of secondary degenerative joint pathology with older age; ongoing subclinical joint inflammation; joint destruction despite apparent remission. The findings have several implications including the most appropriate timing for treatment withdrawal for those in remission.
Disclosure of Interest : None declared
DOI 10.1136/annrheumdis-2014-eular.4414