Article Text

Abstract
Objectives To examine the safety and efficacy of 5-year administration of certolizumab pegol (CZP)+methotrexate (MTX) in patients with active rheumatoid arthritis (RA).
Methods Eligible patients from the Rheumatoid Arthritis Prevention of Structural Damage (RAPID)1 randomised controlled trial (RCT) were treated in open-label extension (OLE) with CZP 400 mg every other week (Q2W), reduced to 200 mg Q2W after ≥6 months, +MTX. Combined safety data from RCT and OLE are presented from initiation of CZP treatment to 12 wks post last visit in patients receiving ≥1 dose of CZP (Safety population, N=958). Efficacy data are presented to start of first site closure (wk 256 of CZP treatment: 52 wks in RCT+204 wks in OLE) for all patients randomised to receive CZP (intent-to-treat (ITT) population, N=783) and CZP patients who completed the 52 wk RCT and enrolled into OLE (wk 52 CZP completers, N=508). Disease Activity Score (DAS)28 (Erythrocyte Sedimentation Rate (ESR)), American College of Rheumatology Criteria (ACR) 20/50/70, Health Assessment Questionnaire – Disability Index (HAQ-DI), and patient retention (Kaplan–Meier analysis) were assessed.
Results Overall event rate per 100 patient-years (ER) of adverse events (AEs) was 290.4, most frequently: urinary tract infections (ER=7.9), nasopharyngitis (ER=7.3) and upper respiratory tract infections (ER=7.3). ER of serious AEs was 20.3 (infections=5.9, malignancies=1.2). 21 patients (2.2%) experienced an AE resulting in death (incidence rate=0.6). At wk 256 of treatment, 55.3% of the CZP ITT population were estimated to remain on treatment (68.7% if solely withdrawals due to AE or lack of efficacy were considered). In wk 52 CZP completers and CZP ITT population, DAS28 (ESR) remission rates and improvements from baseline were sustained to wk 256.
Conclusions CZP+MTX treatment provided a favourable risk-benefit profile over 5 years in patients with active RA. No new safety signals were identified.
- DMARDs (biologic)
- Rheumatoid Arthritis
- Anti-TNF
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Given the chronic nature of rheumatoid arthritis (RA), treatments must have a favourable long-term risk-benefit profile. Anti-tumor necrosis factor (anti-TNF) therapies provide a valuable option for patients.1–4
Certolizumab pegol (CZP) is a PEGylated Fc-free anti-TNF approved for adults with moderate to severe RA. In a 52-week, phase III, double-blind, randomised controlled trial (RCT), Rheumatoid Arthritis Prevention of Structural Damage (RAPID) 1,5 CZP 400 mg or 200 mg every other week (Q2W)+methotrexate (MTX) provided rapid and sustained improvements in signs and symptoms of disease and inhibition of radiographic damage in patients with active RA.
Patients who completed the RCT and those required to withdraw at week 16 due to American College of Rheumatology Criteria (ACR)20 non-response were eligible to enter an open-label extension (OLE).
An initial report, presenting 2-year data from RAPID 1 (1 year of RCT and 1 year of OLE), was published.6 Here, we present extended safety data over 6.5 years of CZP+MTX treatment, and efficacy data over 5 years (1 year of RCT and 4 years of OLE). We also report the effect of CZP dose reduction in patients who initially received CZP 400 mg Q2W in the OLE, subsequently reduced to 200 mg Q2W.
Materials and methods
Study design
The RAPID 1 OLE was conducted in 22 countries between June 2005 and September 2011. Study designs for the RAPID 1 RCT (NCT00152386)5 and OLE (NCT00175877)6 have been reported. In the RCT, patients were randomised 2:2:1 to receive either CZP 400 mg or CZP 200 mg Q2W (induction dosing: CZP 400 mg at weeks 0, 2 and 4), or placebo, with concomitant MTX. At OLE entry, patients were treated with CZP 400 mg Q2W+MTX. However, while this OLE was underway, data from two Phase III studies (RAPID 1,5 RAPID 27) demonstrated no additional benefit with CZP 400 mg Q2W versus 200 mg Q2W. Consequently, following a protocol amendment, the CZP dosage in the OLE was reduced from 400 mg to 200 mg Q2W.
Changes in MTX dose were permitted in OLE (if clinically indicated) but MTX discontinuation was not. DMARDs other than MTX and other biological therapies were prohibited throughout both RCT and OLE.
Informed patient consent and approval by all appropriate ethics committees were obtained for both studies.5 ,6
Patients
RAPID 1 inclusion criteria are reported in the primary publication.5 Eligible patients had active RA (ACR 1987 criteria8) of ≥6 months’ duration prior to screening and had received MTX for ≥6 months (stable dosage of ≥10 mg/week for ≥2 months prior to baseline). Exclusion criteria included diagnosis of other inflammatory arthritis or secondary non-inflammatory arthritis, prior treatment with any biologic therapy within 6 months (3 months for etanercept or anakinra), failure to respond to ≥1 prior TNF inhibitor, history of tuberculosis (TB), active or latent TB, a high risk of infection, malignancy, demyelinating disease or blood dyscrasias.
Two populations from the RAPID 1 RCT were eligible to enter the OLE: (1) CZP or placebo patients who completed the 52-week RCT and (2) CZP or placebo patients who were ACR20 non-responders at both weeks 12 and 14 in RCT, and were required to withdraw at week 16. Upon reconsenting, all patients received OL CZP 400 mg Q2W+MTX.
Safety
The primary objective of the OLE was to assess the safety of CZP+MTX treatment. Combined safety data from RCT and OLE are presented. The safety population includes all patients who received ≥1 dose of CZP in either study. Data are presented from time of first CZP exposure until last visit, or patient withdrawal plus 12-week follow-up. Adverse events (AE) and serious AEs (SAE) were assessed at every visit and classified by system organ class (SOC) and preferred term (PT) according to the MedDRA dictionary (V.9.0). Exposure-adjusted event rates (ER) and incidence rates (IR) per 100 patient-years (pt-yr) are reported. IRs are presented for AEs typically occurring in individual patients only once (eg, malignancy) with data, including exposure, censored after the first occurrence of a particular event in a patient. IRs do not account for when an individual may remain in the trial after experiencing one or more events of interest (eg, infections) and are therefore only appropriate for AEs of single incidence. As more frequent AEs can occur more than once in individual patients, for completeness, both ERs and IRs are presented for AEs occurring in individual patients more than once. The most frequent AEs (ER>7.0) and SAEs (ER>0.25) are reported.
Efficacy analyses
Secondary objectives of the OLE were assessment of the continued tolerability, efficacy and effect on physical function and health outcomes of CZP+MTX.
Efficacy data is reported for two populations: (1) Patients randomised to CZP 400 mg or 200 mg+MTX in the RAPID 1 RCT who completed the 52-week RCT and enrolled into the OLE (week 52 CZP completers), (2) All patients randomised to CZP in the RCT (CZP intent-to-treat (ITT) population).
Efficacy data are presented from baseline of the RAPID 1 RCT to 5 years CZP treatment (eg, for completers, 52 weeks of treatment in RCT followed by 204 weeks in OLE). Efficacy data beyond week 256 are not presented due to a sharp decline in patient numbers, occurring due to site closure as CZP became commercially available. Patient-reported outcomes (PRO) are presented for the week 52 CZP completer population only.
Disease Activity Score (DAS)28 (Erythrocyte Sedimentation Rate, ESR) (Low Disease Activity (LDA) ≤3.2, remission ≤2.6)9; ACR20/50/70; Health Assessment Questionnaire – Disability Index (HAQ-DI); ACR/The European League Against Rheumatism (EULAR) Boolean remission (tender joint count ≤1, swollen joint count ≤1, patient's global assessment of disease activity (Patient's Global Assessment of Disease Activity (PtGA))≤10 mm and CRP≤10 mg/L)10; PtGA (100 mm visual analogue scale (VAS)); and patient's assessment of arthritis pain (VAS) were measured every 12 weeks in the OLE. Fatigue (VAS) and health-related quality of life (HRQoL; assessed by SF-36) were measured at weeks 12, 24 and every 24 weeks in OLE. Continuous measures are presented as absolute scores and change from RCT baseline.
The dose reduction population subset includes all RAPID 1 week 52 CZP 400 mg and 200 mg completers who received CZP 400 mg Q2W+MTX for ≥6 months in the OLE and had the CZP dose reduced to 200 mg Q2W. Dose reduction data are presented over 204 weeks of CZP exposure following dose reduction.
Statistical analyses
Dichotomous data were imputed by modified non-responder imputation (mNRI), whereby missing data due to patient withdrawal secondary to an AE, lack of efficacy or use of rescue medication were imputed by NRI; if dichotomous data were missing for reasons other than these, last observation carried forward (LOCF) imputation was applied. If no suitable LOCF value existed, NRI was used. Missing continuous data were imputed by LOCF. Observed ACR20/50/70 data are also presented.
Kaplan–Meier analysis was used to estimate patient retention in CZP ITT patients who withdrew for any reason, and who withdrew due to AE or lack of efficacy. Patients withdrawing for other reasons were censored at time of withdrawal. Patients who did not withdraw were censored at their last scheduled visit.
Results
Baseline demographics and patient disposition
Patients in week 52 CZP completer, CZP ITT and dose reduction populations had high disease activity at baseline (mean DAS28 (ESR) for CZP completer, ITT and dose reduction populations; table 1).
Baseline demographics and patient characteristics for week 52 CZP completers, the CZP ITT population and the dose-reduction population at the baseline of the RAPID 1 study
Of 783 patients randomised to receive CZP (400 mg or 200 mg)+MTX in the RAPID 1 RCT, 529 (67.6%) completed 52 weeks and 508 (64.9%) reconsented to OLE treatment (week 52 CZP completers) (figure 1A). Of the week 52 CZP completers, 283 (55.7%) remained in the study at week 256 of CZP treatment. 81 (15.9%) had withdrawn from the OLE due to AEs or lack of efficacy by this time point; the remaining patients withdrew for reasons including subject decision, loss to follow-up and protocol non-compliance.

(A) Patient disposition in the Rheumatoid Arthritis Prevention of Structural Damage 1 (RAPID 1) randomised controlled trial and open-label extension and (B) Kaplan–Meier plot of time to withdrawal† for any reason, and due to lack of efficacy or adverse effect from start of feeder study for the certolizumab pegol (CZP) intent-to-treat (ITT) population (N=783). *Withdrew from the study at week 16 per protocol; efficacy populations (CZP ITT patients and CZP completers) are highlighted. †Time to withdrawal is measured from the point at which a patient is first treated with CZP.
The retention rate for the CZP ITT population after 5 years of CZP treatment (accounting for withdrawals for any reason), was 55.3% (estimated by Kaplan–Meier survival analysis). If only withdrawals due to adverse events or lack of efficacy were considered (ie, patients withdrawing for other reasons were censored at time of discontinuation), the estimated retention rate at week 256 was 68.7% of the CZP ITT population (figure 1B).
In the OLE, the mean treatment duration on the 400 mg dose was 595 days, and on the 200 mg dose (following dose reduction) was 938 days.
Safety
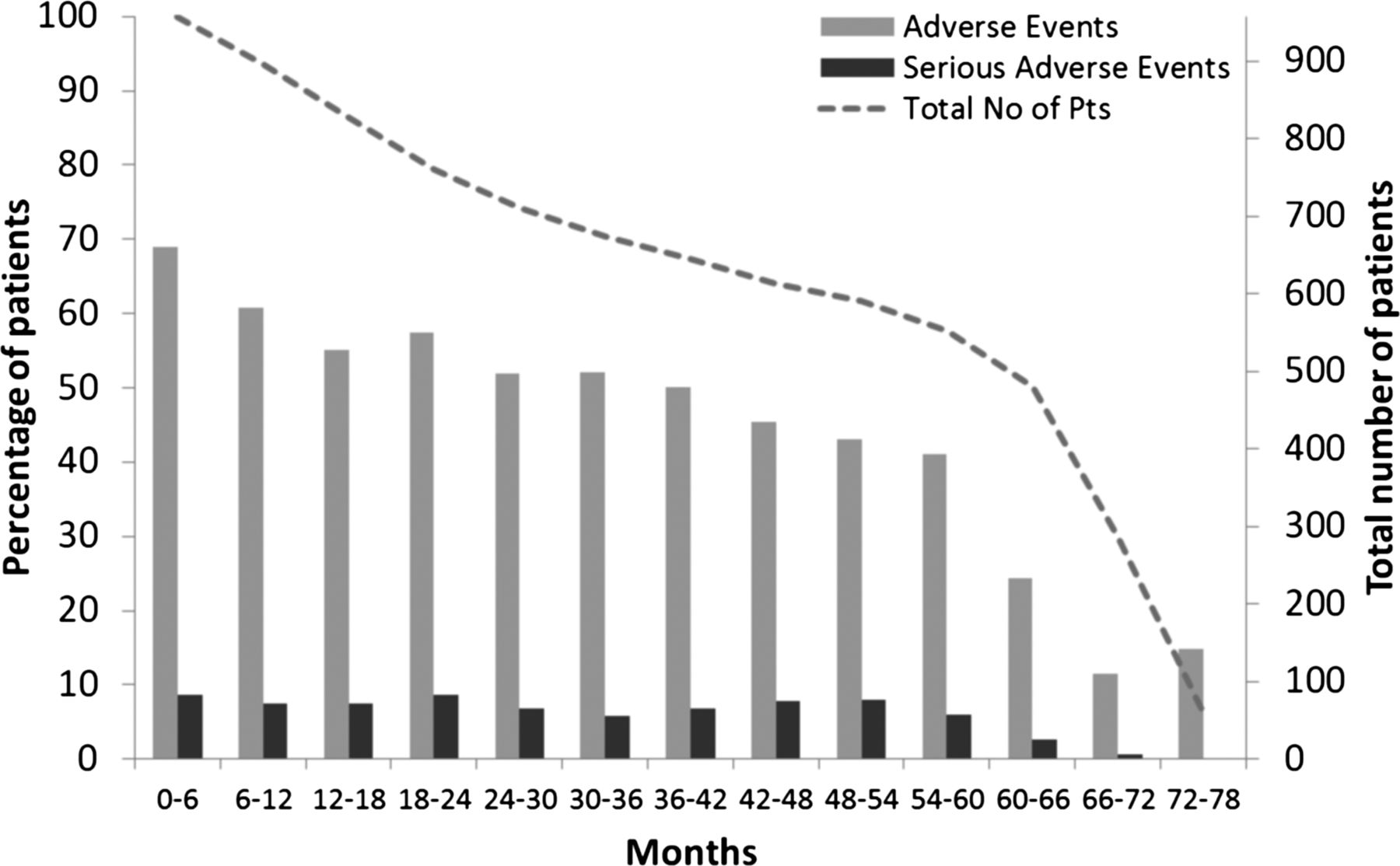
Total exposure to CZP (including 12-week safety follow-up) was 3,732 pt-yrs, with 93.8% of the 958 patients who received CZP reporting AEs during RAPID 1 RCT or OLE (ER=290.4) (table 2). Most (86.6%) were mild to moderate in nature. The most frequent AEs were urinary tract infections, nasopharyngitis and upper respiratory tract infections (table 2). AEs resulted in deaths in 21 patients (2.2%) (IR=0.6), including 5 deaths due to malignancies, 5 to cardiovascular events and 3 to infections. AEs leading to death were considered by the investigator to be related to study medication in 6 patients: 1 patient each with hepatic cirrhosis, pneumonia, malignancy, stage IV gastric cancer, and disseminated TB, and 1 patient with pyrexia, colon cancer, and metastases to liver and lung. SAEs were reported in 399 patients (41.6%), (ER=20.3). The IR for TB infections, including suspected TB, was 0.6. 39 patients experienced SAEs in the SOC neoplasms (including cysts, benign and malignant tumours); excluding non-melanoma skin cancer, 23 of these were considered malignancies following medical review. The most frequent serious malignancies by PT were basal cell carcinoma (N=4, IR=0.1) and breast cancer (N=3, IR=0.1). No cases of demyelinating disease were reported. AE incidence did not increase over time, and SAE incidence remained approximately constant over the majority of the treatment period (figure 2).
Summary of adverse events in all patients treated with CZP in the RAPID 1 RCT and OLE (safety population)

Percentage of patients experiencing adverse events (AEs) and serious AEs over each 6-month period from the start of the feeder study (safety population; N=958). Note, sharp decline in patient numbers from month 60 is due to per protocol site closure in countries where certolizumab pegol became commercially available.
Efficacy
Improvements in DAS28 (ESR) from RAPID 1 were maintained to 5 years (figure 3A). Mean DAS28 (ESR) at RAPID 1 RCT baseline was 6.92 for both week 52 CZP completers and CZP ITT population, decreasing to 3.58 and 3.98 respectively, after 52 weeks of CZP treatment and sustained to 3.43 and 3.83 after 256 weeks. Mean DAS28 (ESR) change from RAPID 1 RCT baseline at week 52 of treatment was –3.32 and –2.91 for the week 52 CZP completers and CZP ITT population, respectively, and at week 256 was –3.49 and –3.08.

{kind=link}
{kind=link}
{kind=link}
Efficacy variables for week 52 certolizumab pegol (CZP) completers (N=508) and CZP intent-to-treat population (N=783). (A) Mean Disease Activity Score (DAS)28 (Erythrocyte Sedimentation Rate, ESR); (B) American College of Rheumatology Criteria (ACR)20, ACR50 and ACR70 response rates); (C) Mean Health Assessment Questionnaire – Disability Index (HAQ-DI). Efficacy variables in patients following dose reduction from CZP 400 mg Q2W to CZP 200 mg Q2W (N=436). (D) Mean DAS28 (ESR); (E) ACR20, ACR50 and ACR70 response rates. *This analysis is presented as weeks following dose-reduction visit. (‘week 0’ is defined as the final efficacy assessment visit where a patient received CZP 400 mg dose.) Total number of patients reflects imputed population. Note, sharp decline in patient numbers from week 144 following dose reduction is due to per protocol site closure in countries where CZP became commercially available.
Rapid improvements in ACR response rates in the RAPID 1 RCT were maintained until week 256 of CZP treatment (figure 3B), with ACR20/50/70 response rates in the week 52 CZP completer population of 74.4%, 57.3% and 39.6%. Observed ACR20/50/70 response rates at week 256 for the CZP completer population were 88.3% (242/274 patients), 69.0% (189/274) and 43.4% (119/274). Analysis of the CZP ITT population gave a more conservative estimate of efficacy, with ACR20/50/70 response rates of 59.0%, 43.7% and 28.8%, at week 256.
Significant improvements in physical function observed in RAPID 1 were maintained to week 256 of CZP treatment (figure 3C). For week 52 CZP completers and CZP ITT population, respectively, the mean change in HAQ-DI from feeder study baseline at week 52 was –0.76 and –0.64 and at week 256 was –0.77 and –0.66.
After 52 weeks of CZP treatment, 24.4% (n=124) and 18.6% (n=145) of week 52 CZP completers and CZP ITT patients achieved DAS28 (ESR) remission; 41.9% and 33.5% achieved LDA. At week 256, 25.2% (n=128) and 20.3% (n=158), respectively, achieved DAS28 (ESR) remission and 48.7% and 39.9% achieved LDA. Furthermore, 15.9% of week 52 CZP completers (n=81) and 11.7% of CZP ITT patients (n=91) achieved ACR/EULAR Boolean remission after 52 weeks of CZP treatment. By week 256 of CZP treatment, this increased to 21.1% (n=107) and 15.9% (n=124), respectively.
At OLE entry (week 52), mean change from RCT baseline in pain (VAS) for week 52 CZP completers was −39.6; at week 256 it was −38.3. The mean change from baseline in PtGA for week 52 CZP completers was −40.6 at week 52 and −38.1 at week 256. For week 52 CZP completers, the mean fatigue scores at weeks 52 and 256 of treatment were 3.2 and 3.5 respectively. (Patient-reported outcome data for the CZP ITT population is included in the online supplementary table S1).
Improvements in patients’ HRQoL (by SF-36) reported in RAPID 111 were maintained in the OLE for the week 52 CZP completers (mean change from RCT baseline at week 256 of treatment: Mental Component Summary, 5.4; Physical Component Summary, 9.3) (SF-36 data for the CZP ITT population is included in the online supplementary table S1).
Analysis on the dose-reduction population (N=436) indicated that improvements in DAS28 (ESR) and ACR response rates were maintained over 192 weeks following CZP dose reduction (figure 3D,E).
Discussion
In the RAPID 1 study, CZP+MTX treatment led to rapid improvements in disease activity and inhibition of structural damage up to 52 weeks in patients with active RA.5 The 2-year data from RAPID 1 and OLE reports that, at week 100, 72.4% and 77.3% of week 52 CZP 200 mg and 400 mg completers, respectively, did not have radiographic progression, as defined by a change from baseline in van der Heijde modified total Sharp score (mTSS)≤0.5.6 This publication represents the final report of the longest-term data from the RAPID 1 study and its OLE to date, and allows for an assessment of the risk-benefit profile of CZP+MTX treatment over 5 years.
Retention rates in long-term clinical trials provide an indication of the long-term efficacy and tolerability of therapies, and hence are of particular importance in chronic conditions. In this study, patient retention rates were relatively high, highlighting the favourable long-term tolerability profile of CZP, and patient satisfaction with treatment. Retention rates in this study were similar to those observed in other long-term anti-TNF studies.12 ,13 However, as clinical trials represent a highly selected patient population that is closely monitored, care must be taken when comparing retention rates from OLE trials to real-life data, such as registries. The safety profile of CZP remained in line with that observed during the RCT and the rate of AEs decreased over time. There was no increase in the overall rate of serious infections with continued exposure to CZP (IR=4.6) compared to that observed in the first and second years of CZP treatment in this study (IRs=7.3 and 5.4 between 0–12 and 12–24 months, respectively).6 The IRs of SAEs and serious infections were comparable to those observed in other long-term TNF inhibitor studies,14–16 although direct comparison is difficult due to differences in study populations and methods of recording AEs. The incidence of malignancies did not increase with additional CZP exposure, and was in line with that expected in the general population.17 Long-term CZP treatment was not associated with a change in the type or severity of AEs, and no new safety signals were identified.
Improvements in signs and symptoms, physical function, HRQoL and PROs observed over 52 weeks in the RAPID 1 trial were sustained throughout 5 years. Despite high baseline disease activity, the proportion of week 52 CZP completers achieving DAS28 (ESR) remission in the study was maintained at approximately one quarter (OLE entry: 24.4%; week 256: 25.2%). Furthermore, measurable improvements in the rigorous ACR/EULAR Boolean remission criteria10 were observed. However, the mean DAS28 (ESR) score plateaued at approximately 4, an effect previously observed with biologic therapies in established RA, indicating that despite clear benefits with CZP treatment, remission is not achieved in all patients.
Patients in the CZP ITT population also displayed long-term reduction in signs and symptoms of disease in the OLE. The difference in outcomes between this population and the completer population was greater for ACR response rates than DAS28 (ESR) and HAQ-DI, suggesting that disease state measures may be of more use when assessing efficacy in long-term studies.
Dose reduction analysis indicated that the registered dose of CZP 200 mg Q2W+MTX provides sustained clinical efficacy for over 3 years of treatment.
The patient population and imputation methodology applied in long-terms studies can have a considerable impact on the reported data, and hence on inferences about efficacy. An independent taskforce has highlighted the need for an unbiased, consistent and scientifically valid approach.18 The analysis of selected patients, who have tolerated and responded to treatment, while providing information on likely outcomes of patients who continue long-term treatment, can introduce a bias. The ITT population, based on all patients, should also be presented.18 In line with these recommendations we have presented data analysed both the CZP RCT completer and ITT populations. As would be expected, ACR response rates and measures of remission are lower in the latter population although, even with this more conservative approach, one fifth of patients achieved DAS28 (ESR) remission after 5 years of CZP treatment.
Long-term comparison of interventions is often complicated by publications which contain either no imputation13 ,15 or no details of imputation methodology.12 ,19 By contrast with other long-term studies which report observed13 ,15 or LOCF20 dichotomous data, this publication applies mNRI to missing dichotomous data. A study comparing long-term observed, LOCF and NRI efficacy data clearly demonstrated the conservative nature of NRI,21 with a further report suggesting that LOCF can lead to unreasonably high estimates of success in long-term analyses, depending on the reasons for patient withdrawal.22 A comparison of observed and NRI data in this study unambiguously demonstrated the more conservative nature of NRI.
Conclusions
CZP+MTX had a favourable risk-benefit profile over 5 years of treatment in active RA patients. The long-term safety profile was in line with that previously reported, with no increase in AEs and SAEs, and no new safety signals. The efficacy of CZP in reducing the signs and symptoms of RA and improving physical function was maintained over 5 years. The efficacy of CZP was not affected by dose reduction from 400 mg to 200 mg Q2W.
Acknowledgments
The authors acknowledge Marine Champsaur, PhD, UCB Pharma, Brussels, Belgium, for publication management and Costello Medical Consulting for editorial and administrative support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Handling editor Tore K Kvien
-
Funding This manuscript has been funded by UCB Pharma.
-
Competing interests E Keystone has received grant/research support from: Abbott, Amgen, AstraZeneca, BMS, F Hoffmann-La Roche, Janssen, Lilly, Novartis, Pfizer, UCB Pharma; consultancy fees from: Abbott, AstraZeneca, Biotest, BMS, F Hoffmann-La Roche, Genetech, Janssen, Lilly, Merck, Nycomed, Pfizer, UCB Pharma; and speaker honoraria from: Abbott, Amgen, AstraZeneca, BMS Canada, F Hoffmann-La Roche, Janssen, Pfizer, UCB Pharma. R Landewé has received grant/research support from: Abbott, Amgen, Centocor, Novartis, Pfizer, Roche, Schering-Plough, UCB Pharma, Wyeth; consultancy fees from: Abbott, Ablynx, Amgen, AstraZeneca, BMS, Centocor, GSK, Novartis, Merck, Pfizer, Roche, Schering-Plough, UCB Pharma, Wyeth; and speaker honoraria from: Abbott, Amgen, BMS, Centocor, Merck, Pfizer, Roche, Schering-Plough, UCB Pharma, Wyeth. R van Vollenhoven has received grant/research support from: Abbott, BMS, GSK, MSD, Pfizer, Roche, UCB Pharma; and consultancy fees from: Abbott, BMS, GSK, MSD, Pfizer, Roche, UCB Pharma. B Combe has received grant/research support from: Merck, Pfizer, Roche-Chugai; consultancy fees from: Merck, Pfizer, Roche-Chugai, UCB Pharma, BMS, Celgene, Lilly, Novartis; and speaker honoraria from: Merck, Pfizer, Roche-Chugai, UCB Pharma, BMS, Celgene, Lilly, Novartis. V Strand has received consultancy fees from UCB Pharma. P Mease has received grant/research support from: Abbott, Amgen, BiogenIdec, BMS, Celgene, Janssen, Lilly, Novartis, Pfizer, UCB Pharma; consultancy fees from: Abbott, Amgen, BiogenIdec, BMS, Celgene, Janssen, Lilly, Novartis, Pfizer, UCB Pharma; and speaker honoraria from: Abbott, Amgen, BiogenIdec, BMS, Celgene, Janssen, Lilly, Novartis, Pfizer, UCB Pharma; L Shaughnessy and B VanLunen are employees of UCB Pharma; D van der Heijde has received consultancy fees from: AbbVie, Amgen, AstraZeneca, Augurex, BMS, Celgene, Centocor, Chugai, Covagen, Daiichi, Eli-Lilly, GSK, Janssen Biologics, Merck, Novartis, Novo-Nordisk, Otsuka, Pfizer, Roche, Sanofi-Aventis, Schering-Plough, UCB Pharma, Vertex; and is owner of Imaging Rheumatology bv.
-
Ethics approval National and Regional Ethics Committee or Institutional Review Board (Global Study).
-
Provenance and peer review Not commissioned; externally peer reviewed.