Article Text

Statistics from Altmetric.com
Patients with rheumatoid arthritis (RA) are at an increased risk for cardiovascular disease. In order to lower this risk, statins are used in clinical practice in addition to biologics.1 Rituximab, an anti-CD20 antibody approved for the treatment of RA, induces B-cell apoptosis by crosslinking and redistributing CD20 to cholesterol-rich lipid rafts.2 Statins have been shown in vitro to induce conformational changes on the CD20 epitope, potentially influencing the apoptotic effect of rituximab.3
There are conflicting reports about the effect of statins on the clinical efficacy of rituximab in RA.4–⇓6 We investigated the impact of statin coadministration on rituximab efficacy in patients from a global clinical trial programme in RA.
This was a retrospective, pooled, observed case analysis from four placebo-controlled phase II/III randomised clinical trials (DANCER, REFLEX, SERENE and IMAGE)7–10 in patients with moderate-to-severe active RA. All patients received concomitant methotrexate 10−25 mg/week at a stable dose and were permitted to receive stable background doses of oral corticosteroids (prednisolone ≤10 mg/day or equivalent) and non-steroidal anti-inflammatory drugs throughout. Efficacy responses (change in Disease Activity Score 28 using erythrocyte sedimentation rate (DAS28-ESR) from baseline, American College of Rheumatology 20% or 50% (ACR20/50) response) and and peripheral blood CD19+ B-cell counts at 24 weeks following one course of rituximab were compared between patients who received concomitant statins for ≥8 weeks (‘statins’, STY) and those who received statins for <8 weeks or not at all (‘no statins’, STN). Differences in outcome measures between STN and STY groups were tested using either an analysis of covariance model for continuous variables or logistic regression for categorical variables, adjusted for potential confounders such as age, treatment group, sex, RA duration, rheumatoid factor (RF) status and baseline DAS28-ESR. An analysis evaluating placebo-adjusted means of the results was also performed.
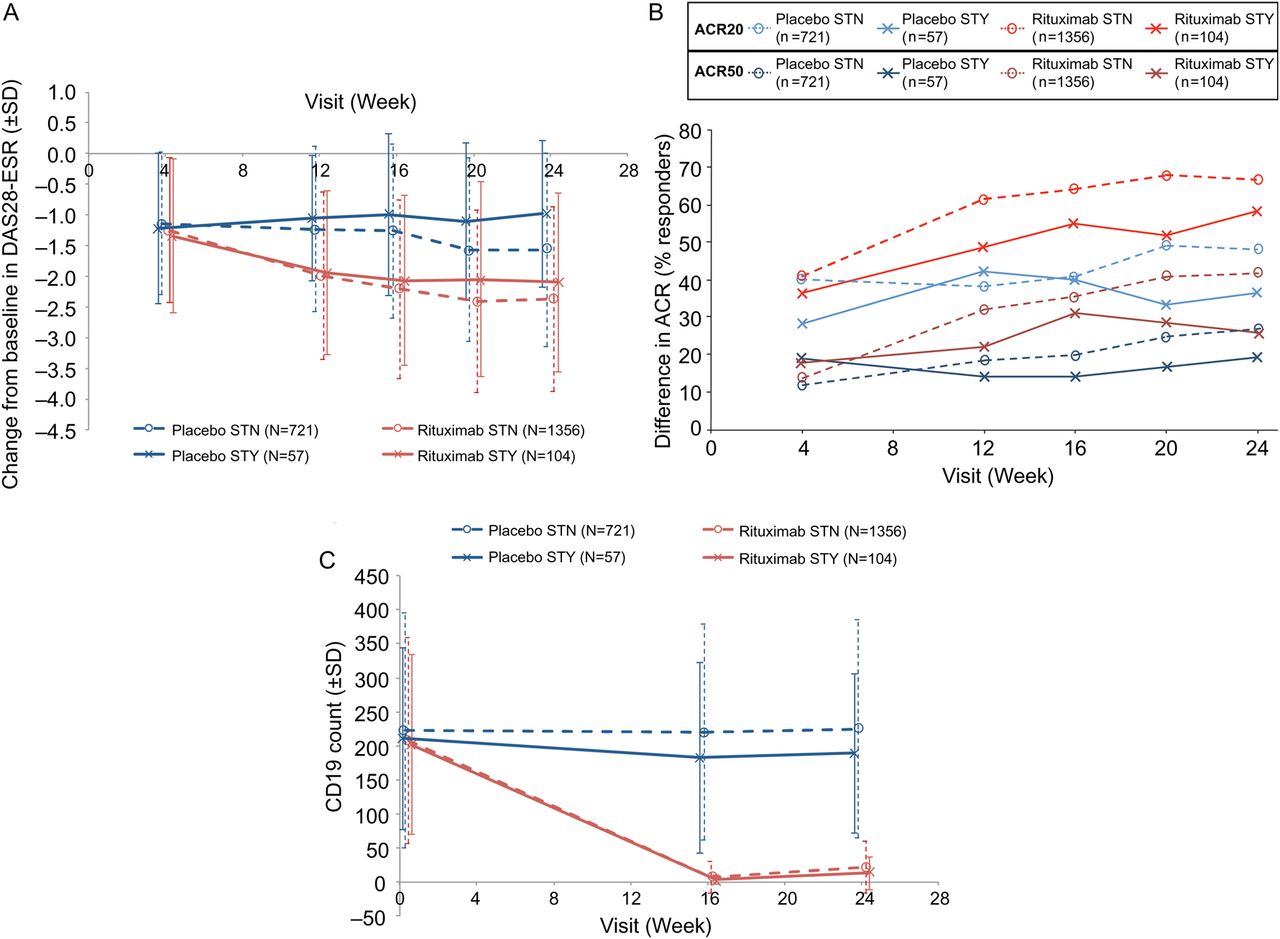
During the 24-week placebo-controlled period, 104 (7.1%) of the 1460 rituximab-treated and 57 (7.3%) of the 778 placebo-treated patients received concomitant statins. STY patients were 10 years older, were more frequently men, had longer RA disease duration, were less frequently RF or anti-cyclic citrullinated peptide (anti-CCP) antibody positive and received more prior therapies than STN patients (table 1). At week 24, rituximab-treated STN patients demonstrated a greater mean (±SD) decrease from baseline in DAS28-ESR (−2.37±1.51) than STY patients (−2.10±1.46); this was consistent with values observed in the placebo-treated STY and STN groups (figure 1A). These differences between STY and STN groups were not statistically significant. In both treatment groups, fewer STY patients achieved ACR20/50 responses at week 24 than STN patients (figure 1B). Placebo-adjusted mean difference for change in DAS28-ESR from baseline (−0.09 (95% CI −0.65 to 0.47), p=0.7640) and placebo-adjusted ORs for ACR20 (1.094 (95% CI 0.49 to 2.45), p=0.8266) and ACR50 (0.775 (95% CI 0.30 to 2.00), p=0.5977) responses between statin groups confirmed there was insufficient evidence of a statin’s effect on efficacy measures. CD19 counts were numerically, but not significantly, lower in STY patients than in STN patients at each visit (figure 1C).
Baseline demographics and disease characteristics of rituximab-treated and placebo-treated patients with RA

{kind=link}
(A) Effect of concomitant statins on change from baseline in DAS28-ESR in rituximab-treated and placebo-treated patients with RA over a 24-week period; (B) Effect of concomitant statins on change from baseline in ACR20 and ACR50 response ratesa in rituximab-treated and placebo-treated patients with RA over a 24-week period; (C) Effect of concomitant statins on change from baseline in peripheral blood CD19+ B-cell levels in rituximab-treated and placebo-treated patients with RA over a 24-week period. Observed data with no imputation made for missing data. Rituximab treatment group is pooled rituximab doses; data used are four pooled studies to week 24.aACR20 and ACR50 response rates calculated to original baseline. ACR20, American College of Rheumatology 20% improvement criteria; ACR50, American College of Rheumatology 50% improvement criteria; DAS28-ESR, Disease Activity Score 28 using erythrocyte sedimentation rate; PBO, placebo; RA, rheumatoid arthritis; RTX, rituximab; STN, no statins; STY, statins.
Smaller reductions in DAS28-ESR and ACR20/50 responses were seen in the STY patients compared with the STN patients in both treatment groups that were not statistically significant. Placebo-adjusted tests showed that statin use did not significantly alter the treatment difference between rituximab and placebo. STY patients had longer disease duration and received more prior treatments, which may explain the lower ACR and DAS-28 responses in both the rituximab and the placebo groups. In contrast to previously published studies that reported on fewer than 30 patients,4–⇓6 this is the first report from a large placebo-controlled dataset to assess the effect of statins on efficacy of rituximab. These findings suggest that concomitant use of statins did not significantly alter patient response to rituximab treatment over a 24-week placebo-controlled period.
Footnotes
-
Contributors All authors made substantial contributions to the conception of the work, the analysis and interpretation of the data, and drafting and revising the manuscript. All authors have approved of the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
-
Funding This study was funded by F Hoffmann-La Roche Ltd and Genentech (A Member of the Roche Group). F Hoffmann-La Roche Ltd provided support for third-party writing assistance for this manuscript.
-
Competing interests PBL, SL and EWH are Roche employees; AJ is a Genentech employee.
-
Patient consent Obtained.
-
Ethics approval All participating sites received approval from their governing institutional review boards.
-
Provenance and peer review Not commissioned; externally peer reviewed.