Article Text

Abstract
Objective The primary objective of the study was to explore safety and tolerability of hyperimmune caprine serum (AIMSPRO) in established diffuse cutaneous systemic sclerosis (SSc). Secondary objectives included assessment of potential efficacy and biological activity and exploration of candidate biomarkers.
Methods This was a double-blind parallel group randomised placebo-controlled clinical trial. After informed consent 20 patients with established diffuse cutaneous SSc of greater than 3 years duration not receiving immunosuppressive therapy were randomised to receive either active (n=10) or placebo formulation (n=10) by subcutaneous twice weekly injection over 26 weeks. Clinical assessments were evaluated over 26 weeks.
Results There were no safety concerns during this study. Frequency of adverse events was not different between active and placebo groups. Mean modified Rodnan Skin Score (mRSS) fell by 1.4±4.7 units with active treatment but increased by 2.1±6.4 units on placebo when baseline values were compared with 26 weeks and responder analysis showed clinically meaningful improvement in mRSS at 26 weeks in 5 (50%) of actively treated patients compared with 1 (10%) in the control group (p=0.062). PIIINP (µg/L) showed a comparatively larger increase in the treatment group compared with the placebo group, (p=0.0118).
Conclusions These results confirm tolerability and safety of this novel biological agent in established diffuse SSc. The value of a placebo treated control group in small clinical trials evaluating skin disease in SSc is confirmed. Potential improvement in mRSS and changes in PIIINP in cases receiving active therapy suggest that this intervention may be of clinical benefit and warrants further evaluation.
- Systemic Sclerosis
- Treatment
- DMARDs (biologic)
- Autoimmune Diseases
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Systemic sclerosis (SSc) is a multisystem disease that is associated with inflammation, fibrosis and vasculopathy. It is uncommon but has high morbidity and the highest case-specific mortality of any rheumatic disorder with 50% of patients dying or developing major internal organ complications within 3 years of diagnosis.1 There are two major subsets of systemic sclerosis, limited cutaneous SSc and diffuse cutaneous SSc (dcSSc).2
Although there is understandable focus on the high burden of severe skin and internal organ involvement in early stage diffuse SSc, with less than 3 years disease duration,1 there is also substantial burden at later stages and this has been highlighted in recent cohort studies.3
Traditional models of pathogenesis have suggested that early vascular events associated with autoimmunity and inflammation lead to subsequent fibrosis. Although this is plausible and supported by preclinical mechanistic studies it is clear that a broad range of biological processes interact in SSc and that these include involvement of key profibrotic cytokines such as transforming growth factor-β and connective tissue growth factor as well as proinflammatory cytokines such as interleukin 6 (IL-6) and tumour necrosis factor (TNF)α. There is also increasing evidence of an imbalance in Th1/Th2/Th17/Treg system promoting inflammation and fibrosis and activation of B cells promoting production of autoantibodies.4 Diffuse SSc is often categorised as early-stage or established/late-stage disease and it is possible that the pathogenic factors underlying the distinct phases of the disease are different. In particular, pathogenic drivers of late-stage disease are less clear, but there is emerging evidence that persistent perturbation of immune cell function may be relevant.5 The cornerstone of management of early stage diffuse SSc is broad spectrum immunosuppression.6 Emerging data support the benefit of immunosuppression for skin and lung fibrosis in SSc, especially when given at the early stages of disease.7
Study drug
Hyperimmune caprine serum (AIMSPRO, Anti-inflammatory IMmuno -Suppressive PROduct) is a goat serum extract derivative supplied frozen and thawed to a liquid for immediate injection. It is produced in goats raised and housed at a licensed facility in Tasmania, Australia. The animals are vaccinated using detergent-inactivated HIV viral lysate. Serum is shipped frozen to the manufacturing facility in Victoria, Australia where the sera are pooled, fractionated and diafiltered to preserve various macromolecules, immunoglobulin species and low molecular weight components prior to further processing nanofiltration and vialing.
The final product contains principally caprine immunoglobulins but also various small molecular weight species including cytokines. ELISA characterisation of the serum has revealed the presence of a range of components including the cytokines IL-4 and IL-10, proopiomelanocortin, arginine vasopressin, β-endorphin and corticotropin-releasing factor. Previous studies have shown that when peripheral blood mononuclear cells are isolated and incubated with serial dilutions of AIMSPRO, raw hyperimmune serum and heat-inactivated sera induced the release of IL-10 in vitro. Studies in patients with multiple sclerosis and chronic inflammatory demyelinating polyneuropathy have shown a sodium channel opening effect, which is thought to be one of several potential mechanisms of action of this novel medication.8
Patients and methods
Study design
The primary objective of this double blind, placebo controlled parallel group study was to assess safety and feasibility of using this novel agent in late-stage dcSSc. The secondary objectives were assessment of possible treatment effect (using clinical outcomes such as modified Rodnan Skin Score (mRSS), SSc Health Assessment Questionnaire Disability Index (SSc HAQ-DI) and Short Form 36 (SF-36) quality of life questionnaire) and the exploration of candidate biomarkers (such as von Willebrand factor (vWF), serum IL-2 receptor (sIL-2R), PIIINP, as well as multiplex analysis of serum and plasma). The study was approved by the local Ethics Committee. At completion of the blinded phase all subjects were offered 26 weeks of treatment with AIMSPRO on a compassionate basis and efficacy and safety end points were evaluated at 52 weeks.
Study patients
This was a single-centre double-blind placebo-controlled study conducted at the Royal Free London NHS Foundation Trust, London, UK. Eligible patients were recruited from outpatient clinics and chart reviews. We treated 10 subjects with established dcSSc using hyperimmune goat serum and compared outcome over 6 months with 10 control subjects receiving placebo. Subjects were randomised to receive 1 ml study drug or placebo subcutaneously twice weekly for 6 months. The first two doses of medication were administered in the study centre under supervision at week 0, day 0 and week 0, day 3. Subjects were followed for 26 weeks with additional safety visits occurring at weeks 2, 6, 14, 20 and a final safety visit at week 52 (6 months after the end of the double-blind phase).
The major inclusion criteria were: fulfilling the 1980 Preliminary classification criteria for systemic sclerosis.9 Clinical classification of diffuse SSc (LeRoy criteria)2 and at least 3 years duration since the first non-Raynaud's manifestation of SSc.
The exclusion criteria were: use of a putative disease-modifying drug within 1 month of screening, patients receiving previous administrations of AIMSPRO or those with a history of known allergy to animal proteins.
Concomitant medication
Throughout the study period, all medications were kept stable where possible. Medications contraindicated during the treatment phase included other investigational drugs, other biological therapies or immunosuppressive agents. Sodium channel blocking agents such as anticonvulsant medications were also contraindicated. Medications that were allowed during treatment phase included prednisolone up to 10 mg/day, and medications for treatment of Raynaud's phenomenon.
Clinical assessments
For evaluation of skin thickness, the 17-site mRSS was used, with each site assessed on a scale of 0–3 with a maximum score of 51. For individual subjects, clinically meaningful change in skin score was defined as greater than 4 skin score units and at least 20% change in overall mRSS, as described previously.10 The same assessor performed all assessments for the duration of the trial ensuring a standardised approach. Additional mRSS data from 26-week unblinded administration were also available and this provided additional opportunities for exploratory analysis of AIMSPRO in cases that had previously received placebo. Pulmonary function and echocardiogram were performed using standard techniques. All subjects completed SSc-HAQ,11 SF-36, neuropathic pain visual analogue scale (VAS) and UK functional score 12 (an 11-item 4-grade questionnaire, developed specifically to assess functional capacity in scleroderma patients) questionnaires at baseline visit, week 6 and week 26. In addition, exploratory clinical assessments such as Medical Research Council sum score (an assessment of muscle power), sniff nasal inspiratory pressure (SNIP, an assessment of respiratory muscle function) and the R-R interval (a surrogate marker of autonomic dysfunction) were performed at the same time points.
Laboratory assessments
Serum and plasma samples were taken at each visit to assess safety and for exploratory biomarker analyses. These followed the template of recent expert consensus regarding exploratory biomarker studies in SSc trials.13 Serum amino terminal propeptide of type III collagen (PIIINP), a marker of fibrosis, sIL-2R, a marker of inflammation, vWF, a marker of vasculopathy were analysed using standard ELISA assays by Quest Diagnostics, California, USA, under good clinical practice (GCP) conditions.
Adverse events
All subjects were monitored for adverse events (AEs) occurring after screening, even if they had not received study drug. Serious AEs (SAEs) occurring after the first injection and up to 6 months after the last injection were documented and reported to the sponsor and medical monitor within 24 h.
Statistical analysis
Key measures of efficacy in this study were change in SSc HAQ-DI from baseline to week 26, change in mRSS from baseline to week 26, the change in the UK Function Score from baseline to week 26 and the change in SF-36 scales from baseline to week 26. Change in HAQ-DI and mRSS analysed as a continuous variable were the prespecified efficacy end points. Responder frequency analysis for mRSS was also included post hoc to capture clinically meaningful change in mRSS.
Inferential testing has been performed to compare groups in the change from baseline to each post-treatment visit. Two-sided p values <0.05 were considered statistically significant. A mixed models repeated measures analysis was performed on the data in the first instance. In some cases the mixed models algorithm could not converge, so a standard repeated measures analysis of variance was performed. The use of the mixed models repeated measures also allowed the calculation of probabilities for the adjusted mean change value tested against a standard value of zero, whereas the repeated measures analysis of variance does not calculate those probabilities, but does provide the 95% CI. Other analyses included a responder frequency analysis to capture individual patient data within the more variable cohort changes in mean mRSS. The unconditional z-pooled test was used to analyse responder frequency analysis, as recommended by Lydersen et al14.
Results
Study cohort
Twenty-two subjects were screened and there were two screen failures. Twenty subjects were enrolled into the study, all of whom received at least one dose of study medication. Of these, 17 completed the study and there were 3 withdrawals. None were lost to follow-up. Demographic characteristics of the cohort are summarised in table 1 and disease characteristics at baseline are outlined in table 2. These features were as expected for a cohort of subjects with established diffuse SSc.
Demographics of the study cohort
Baseline characteristics of the study cohort
Safety and adverse events
All subjects in both groups had at least one AE and AEs were frequent in both groups in keeping with the high morbidity of the disease. There were numerically more AEs in the placebo group compared with the treatment group (though it did not reach statistical significance), 154 in the placebo group and 139 in the treatment group. This supports a conclusion that the study drug was safe and well tolerated, although a larger study would be needed to explore if AEs are significantly less than for placebo. Details of AEs are provided in table 3.
Summary of adverse events (AEs)
The most commonly reported AEs were injection site reactions, cutaneous or musculoskeletal-related issues (such as skin itching, joint pains and ischaemic digital ulcers) and infections. Transient injection site reactions occurred in both groups, but were more common in the treatment group. The frequency of other AEs was similar in both groups. There were no statistically significant differences in the safety laboratory values throughout the study and no differences were noted between the groups in vital signs, physical examination, electrocardiography or echocardiography.
There were six SAEs in three patients in the placebo group and four SAEs in three patients in the treatment group. Two patients in the placebo group and one in the treatment group withdrew due to AEs or SAEs. There were no deaths during the course of the study. Details of SAEs are provided in table 4.
Summary of serious adverse events (SAEs)
Changes in skin score
We first analysed the difference from baseline score to 26 weeks as an outcome variable, and the difference between the groups using Student t test and corresponding CIs. Using this approach, analysis for the primary data shows mean mRSS fell by 1.4±4.7 units with active treatment but worsened by 2.1±6.4 units on placebo (p=0.181, unpaired t test) when baseline values were compared with 26 weeks.
Because some cases demonstrated clinically meaningful improvement in mRSS, we proceeded to post hoc analysis of responder frequency in active and placebo treated subjects. In the active treatment group one (10%) patient had at least 20% improvement from baseline in mRSS at week 6, and the number had increased to five (50.0%) at week 26. In contrast the placebo group had a greater proportion of patients (four patients; 40.0%) with response at week 6, and fewer patients (one patient; 10.0%) at week 26. The difference between groups at week 26 showed a strong trend towards statistical significance (p=0.062) by the unconditional z-pooled test, figure 1A. To extend these skin score data we undertook further analysis from an extended dataset, for patients receiving AIMSPRO on a compassionate basis for 26 weeks after completion of the double-blind phase of the study. These data are generally supportive of the trend for improvement seen in the blinded phase. Thus, skin score data were available for seven additional cases treated for 26 weeks with AIMSPRO, and from three cases that chose not to take the drug but that were observed for a further 26 weeks off treatment. For this larger patient group the change in MRSS between baseline and 26 weeks was −2.00±1.03 for those treated with AIMSPRO (n=17) and +2.39±1.64 in those not receiving active therapy (n=13). Using Student t test and corresponding CIs, this difference reached statistical significance (p=0.025), although the limitations of open label data and a post hoc analysis must be considered.
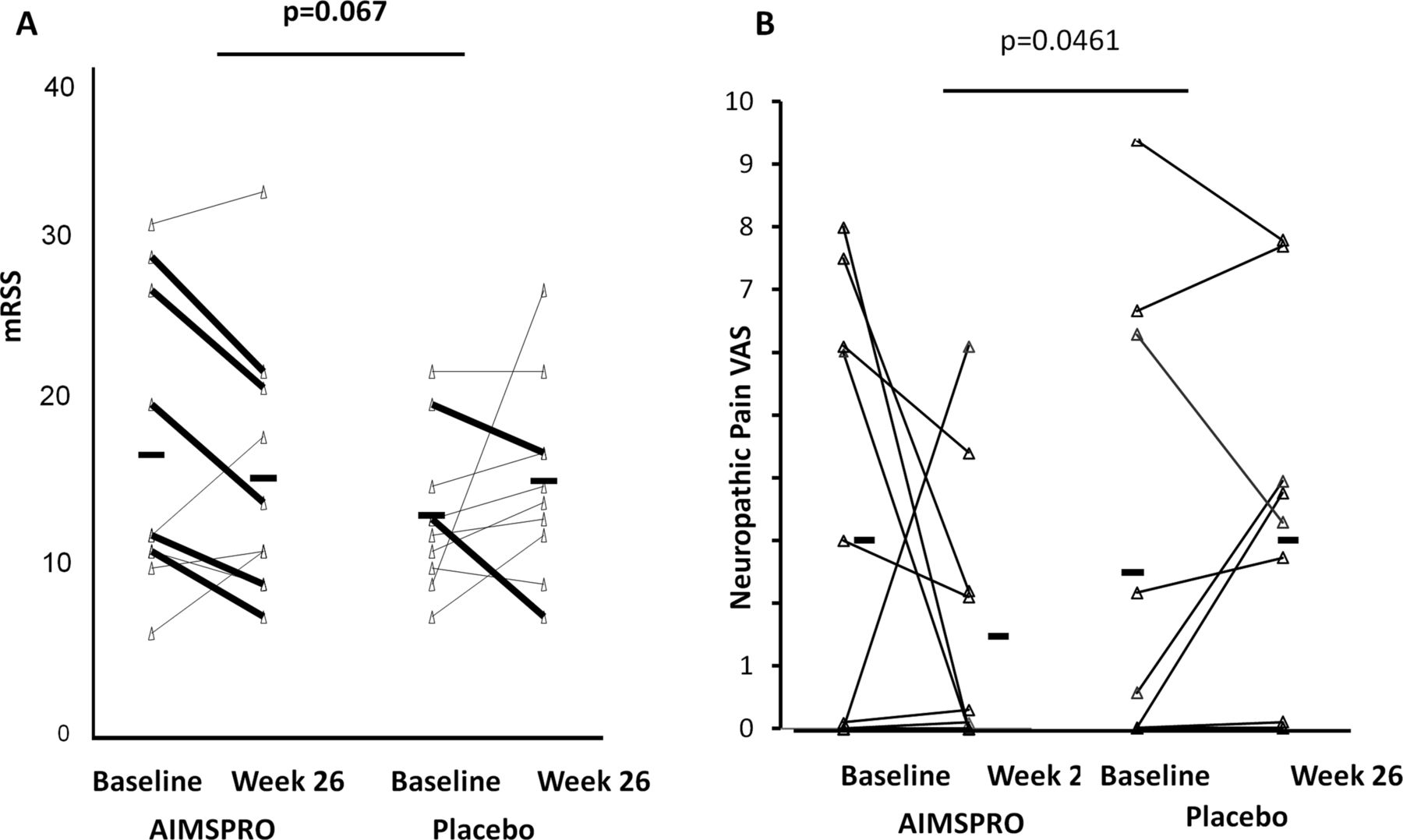
Improvement in modified Rodnan Skin Score (mRSS) and in neuropathic pain visual analogue scale (VAS) from baseline to week 26 in active treatment arm. (A) There was an increase in mean mRSS in the placebo treated subjects and improvement in those receiving active therapy. This did not reach statistical significance but changes were driven by the larger number of cases on active treatment that showed clinically meaningful improvement in mRSS during the trial (>4 skin score units and 20% of baseline mRSS). The lines marked in bold show cases with significant improvement on active treatment or placebo. Responder frequency analysis showed a strong trend in favour of active treatment (p=0.062). (B) Neuropathic pain VAS showed a significant difference between groups at week 26 with an improvement in the treatment group and no significant change in the placebo group.
Other outcomes
Mean±SD for HAQ-DI at baseline was 1.2±0.07 for the active group and 1.6±0.63 for the placebo group and at 26 weeks it was 1.2±0.98 for the active group and 1.6±0.55 for the placebo group(p=0.47). There was no statistically significant difference between the groups for any of the other parameters of SSc HAQ (including patient global VAS), physician global VAS (p=0.35) or the UK functional score (p=0.52).
In the eight domains of SF-36, the only domain to show some change was Role Physical, which showed a worsening in the placebo group and maintenance or stabilisation in the treatment group between baseline and week 26, with a trend to significance between the groups (p=0.07). The Medical Research Council sum score, SNIP and R–R interval did not show any statistically significant differences between the treatment groups. Neuropathic pain VAS showed a significant difference between groups at week 26 with an improvement in the treatment group and no change in the placebo group, p=0.0461, figure 1B.
Lung function indices showed a trend of benefit for active treatment compared with the placebo group for those variables that reflect respiratory effort (forced vital capacity and forced expiratory volume in one second). However when background disease was taken into account, there was no significant difference between the two treatment groups. Carbon monoxide transfer factor and total lung capacity did not change during the study.
Serum biomarkers
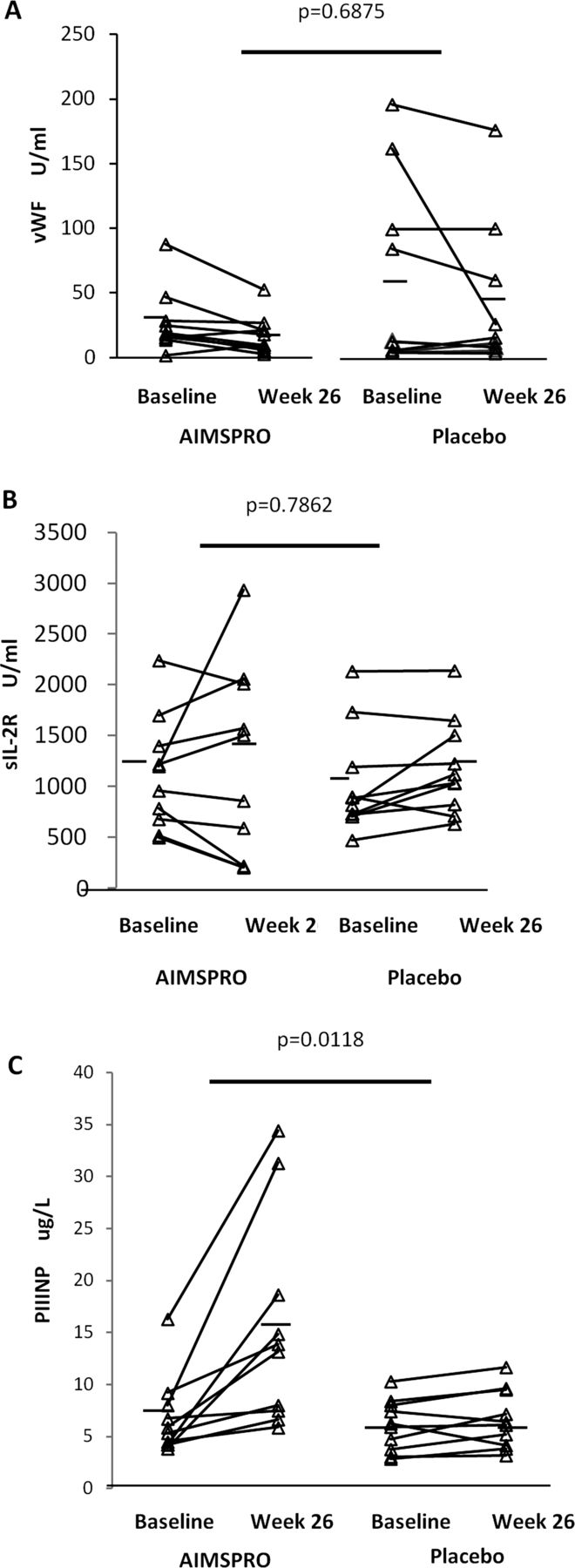
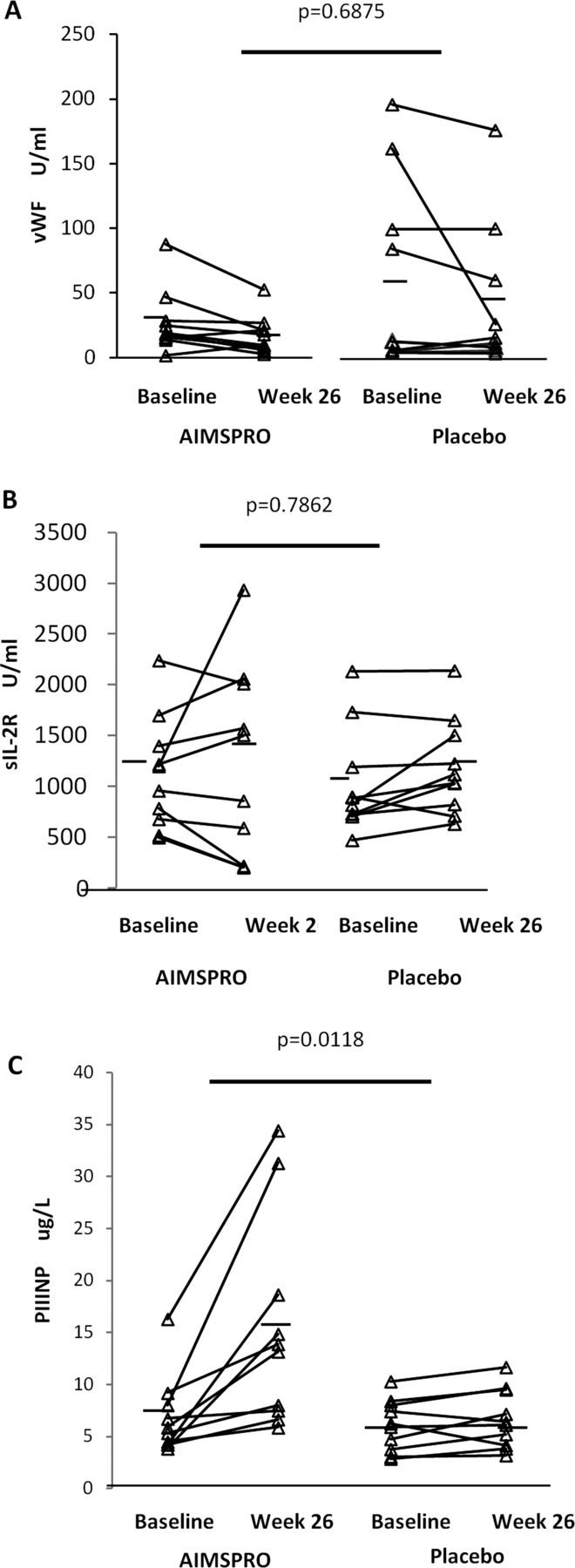
There were no statistically significant changes in vWF and sIL-2R between the two groups comparing baseline to week 26. However, PIIINP (µg/L) showed a comparatively larger increase in the treatment group compared with the placebo group; treatment group baseline 6.9±3.8, 26 weeks 15.4±10.1, placebo group baseline 5.3±2.4, 26 weeks 5.6±2.7, p=0.0118, figure 2.
{kind=link}
{kind=link}
Graphical representation of change from baseline to week 26 for candidate serum biomarkers. There were no statistically significant changes in von Willebrand factor (vWF; A) or sIL-2R (panel B) between baseline and end of study. However, PIIINP (C) showed significant increase in the active treatment arm compared with the placebo group. This novel observation may reflect increased connective tissue remodelling in late-stage SSc cases receiving active treatment as it occurs in the context of improvement in average skin score.
Discussion
The primary objective of this study was to show safety and feasibility of using this novel agent in dcSSc, a complex multisystem autoimmune disease. The results of our study confirm that this drug is safe and well tolerated. AEs were frequent and there were more AEs and SAEs in the placebo group, but this was not statistically significant. None of the SAEs was deemed to be due to the study medication. Late stage disease was chosen because it provides a robust platform for safety analysis through the likely burden of disease and facilitated a placebo-controlled study design. The secondary objective was to explore potential efficacy. For skin score, a responder analysis showed significant benefit in the active treatment arm and a trend for improvement in mean skin score during the blinded phase of the study, and significant improvement when those receiving open label active therapy after the placebo controlled phase, analysed after unblinding. These data are reminiscent of improvement in skin score that was also observed in the treatment group in patients with late stage dcSSc in the oral collagen trial,5 another novel immunomodulatory therapy.
The biological basis for any treatment effect from AIMSPRO is unclear at this stage and may be complex. However, data suggest a direct immunomodulatory effect that includes modulation of serum levels of relevant cytokines such as IL-10 (SH, personal communication). Previous studies have suggested that modulation of IL-10 activity may be one of the relevant effects of this agent and we confirmed that levels of IL-10 were significantly reduced at 6 weeks after starting AIMSPRO compared with placebo (data not shown). In addition, AIMSPRO contains immunoglobulins and this may be relevant in that there are some reports suggesting that immunoglobulins may be of benefit in cases of SSc.15
Other interesting results include an improvement in neuropathic pain VAS in the treatment group which is in keeping with the potential sodium channel effect of this treatment. Pain is a major morbidity in SSc and is consistently ranked highly as a patient reported outcome and component of the SSc-HAQ. The aetiology of pain is multifactorial and related to tissue ischaemia, musculoskeletal inflammation and possibly intermittent release of neuropathic mediators: hence the benefit observed with AIMSPRO is interesting and potentially clinically important.
Though there was substantial functional disability in the patients as evidenced by HAQ-DI baseline scores, there was no significant change in HAQ-DI between groups from baseline to 26 weeks, which was similar to other trials.5 ,16 ,17 A recent meta-analysis of seven scleroderma trials did show a downward trend in HAQ-DI at 6 months but the change in HAQ-DI was not significant at 12 months. However, all of the trials in this meta-analysis were conducted in patients with early disease.18
The study cohort was not recruited to evaluate lung function and although the changes are interesting, they need to be interpreted with caution. Lung function data show a trend to improvement in forced vital capacity and forced expiratory volume in one second in the active arm. The main changes are in components of the lung function that involve patient effort, raising the possibility that muscle weakness may be one explanation, though the SNIP data and total lung capacity did not show any changes between groups. Two subjects in the placebo group deteriorated compared with one in the treatment group. All three had pre-existing lung disease and one of the subjects in the placebo group had to be withdrawn due to worsening lung disease necessitating further immunosuppression. The Quinapril in Scleroderma (QUINS) trial also showed a trend to improvement in the active treatment group, the mechanism of this was unknown but was not due to differences in immunosuppression.19
Biomarker analysis shows no changes for vWF or sIL-2R, but there are interesting changes in PIIINP with a significant increase at 26 weeks in the treatment group compared with the control group. The mechanism for this is unknown as PIIINP has previously been proposed as a marker of fibrotic burden and is used to monitor potential hepatic fibrosis in cases of psoriasis treated with methotrexate. It is noteworthy that baseline values in both groups are in keeping with other studies.16 ,17 ,20 However, the CAT-192 trial showed no change between groups at end of study and the Infliximab trial showed a decrease in values from baseline to end of study. The conflicting results may be explained by the differences in disease duration of subjects in these two studies and our study subjects. These data warrant further prospective evaluation in a larger cohort.
Strengths of this study are a double-blind design with a placebo group enabling safety assessment and comparison between groups for efficacy signals; the same assessor for mRSS throughout the trial, and a relatively uniform patient group in late-stage disease, reducing the natural variability between presentations seen in early inflammatory disease. Our study has advantages over an open label design used elsewhere that makes a potential efficacy signal difficult to detect.16 ,21
In conclusion, we report a pilot study confirming safety and tolerability of AIMSPRO in established dcSSc. Our data also suggest possible efficacy based upon improvement in mRSS in some patients, beneficial effect on pain and trend for improvement in other variables. Changes in serum PIIINP are of interest and warrant further investigation and replication in a larger cohort.
References
Footnotes
Handling editor Tore K Kvien
Eudract No. 2007-003122-24 ClinTrials.gov No. NCT00769028
-
Correction notice This article has been corrected since it was published Online First. The article has been made open access.
-
Contributors All authors were involved in data acquisition, design, analysis and writing of the manuscript and approved the final submitted version.
-
Funding This study was sponsored and funded by Daval International.
-
Competing interests SH, DM are employees of Daval International. JV is consultant to Daval International. CPD, NPQ have no competing interests.
-
Ethics approval Royal Free Hospital and Medical School Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.