Article Text

Abstract
Background The ASAS definition of a positive MRI of the sacroiliac joints (MRI-SI+) for the classification of axial spondyloarthritis (axSpA) patients (pts) includes inflammatory lesions only1,2. The role of structural lesions (SL) on MRI-SI in classifying pts is unclear1.
Objectives To explore the potential role of SL on MRI-SI in classifying axSpA pts.
Methods Pts with back pain (≥3 months, ≤2 years, onset <45 years) from the 5 centers in the SPondyloArthritis Caught Early (SPACE)-cohort were included. Pts underwent MRI-SI. MRIs-SI were scored by 3 well-calibrated readers independently for ankylosis, sclerosis, erosions, and fatty lesions (FL) (T1-weighted images; STIR viewed simultaneously). Erosions, sclerosis and FL were defined according to the MORPHO definition3 (≥1 lesion on ≥2 consecutive slices or ≥2 lesion on 1 slice). Ankylosis was defined as ≥1 lesion on ≥1 slice. Lesions were considered present if 2/3 readers agreed. MRI was considered positive for several (combinations of) SL (MRI-SI-s+) using cut-offs based on the acceptance of ≤5% false-positives in pts without SpA. Pts are considered as possible axSpA if not fulfilling the ASAS axSpA criteria3, but if ≥1 specific SpA-feature (high LR+) or ≥2 less specific SpA-features are present4. We classified possible axSpA pts using MRI-SI-s+ instead of MRI-SI+ and calculated the LR product with LR+ 9.0 for MRI-SI-s+ as if MRI-SI+4. Based on the LR product the probability of having axSpA was calculated4.
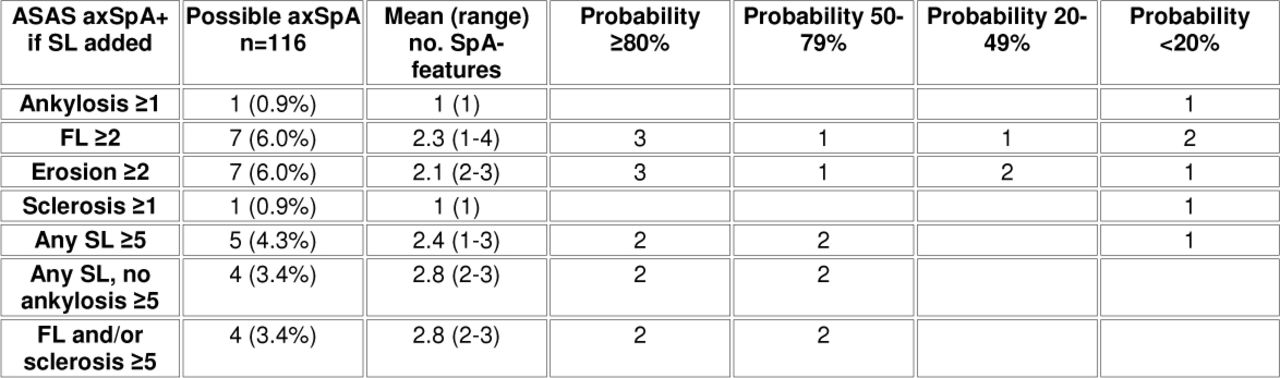
Results Only possible axSpA pts with MRI-SI data were included (n=116). Depending on the used MRI-SI-s+ definition, 1% (ankylosis ≥1) to 6% (erosions ≥2 or FL ≥2) of the possible axSpA pts could be classified as axSpA (table). Combining the various definitions of MRI-SI-s+ results in 14 additional pts (12.1%) classified as axSpA (5 pts with probability ≥80%); 5 pts fulfilled 4 of the proposed MRI-SI-s+ definitions. In pts with a high number of SpA-features, using MRI-SI-s+ to calculate the LR product results in a probability ≥80%, making an axSpA diagnosis very likely. However, in pts with only 1 or a few SpA-features, the probability remains <80%.
{kind=link}
Conclusions These explorative data point out that SL on MRI might play a role in classifying possible axSpA pts. However, only few additional pts are classified as axSpA with a high probability while the same number of pts with a low probability would (falsely) be classified if SL would be added to the definition of a positive MRI. Further studies are needed to define the best type/combination and cut-off of SL.
References
Rudwaleit ARD 2009;68:1520-7
Rudwaleit ARD 2009;68:777-83
Weber A&R 2010;62:3048-58
Rudwaleit ARD 2004;63:535-43
Disclosure of Interest None Declared