Article Text

Abstract
Background The EULAR treatment guideline recommends rheumatologist to strive, in newly diagnosed rheumatoid arthritis (RA) patients, for remission or at least low disease activity within 3 months in order to obtain better functional and radiological outcomes. Since it takes 6-12 weeks to see the optimal effect of DMARDs, the right choice of induction DMARD therapy plays an important role in obtaining current treatment goals. Therefore it would be helpful to be able to predict DMARD response in a very early phase in order to obtain current treatment goals.
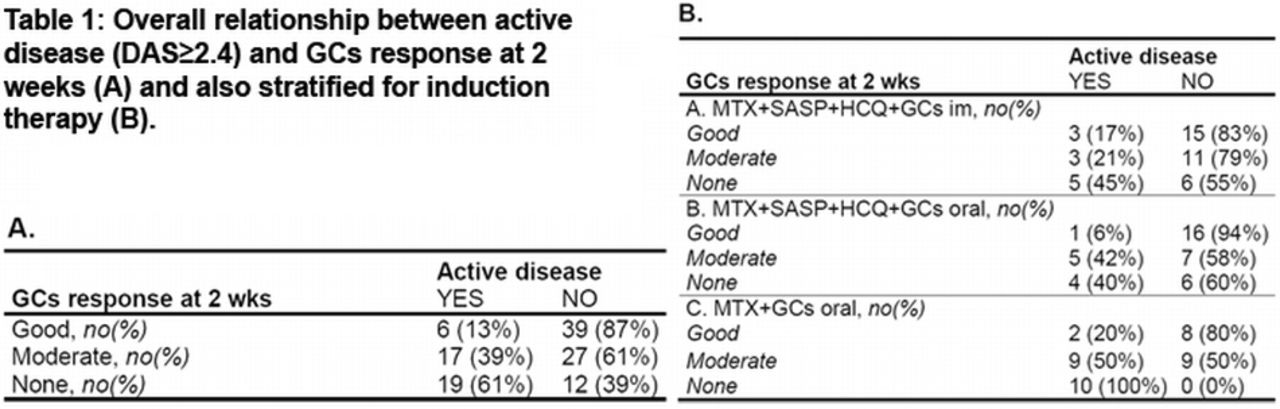
Objectives To investigate if a glucocorticoid (GC) response at 2 weeks, defined with EULAR response criteria, can predict active disease (DAS≥2.4) after 3 months of DMARD therapy.
Methods For this study data of the tREACH study, an ongoing clinical trial that evaluates different induction therapies in early RA, were used. Patients are stratified into probability tertiles (respectively low, intermediate and high) according to their likelihood of progressing to persistent arthritis based of the prediction model of Visser. The Visser algorithm and 2010 criteria for RA have similar discriminative abilities to identify patients at risk of persistent arthritis at 1 year. All patients within the high probability stratum, who had a baseline DAS>2.2 and a DAS assessment at 2 weeks after randomization, were included (n=120). In the high probability stratum patients were randomized into 3 induction therapy strategies: [A] Combination therapy (MTX 25 mg/wk + SASP 2 gr./day + HCQ 400 mg/day) with GCs im (Depomedrol 120mg), [B] Combination therapy with an oral GCs tapering scheme (starting dose 15 mg) and [C] MTX with oral GCs similar to B.
Results GCs none-responders at 2 weeks have a 10.29 (95% CI;3.34 – 31.64) folded increase for active disease after 3 months of DMARD therapy compared to a GCs good-responder. If we stratify for induction therapy odds ratios (95% CI) were 4.2 (0.75 – 23.18); 10.7 (0.98 – 115.7) and infinite for respectively treatment arm [A], [B] and [C] (table 1).
{kind=link}
Conclusions Determining GC response at 2 weeks is a useful tool for recognizing those patients who will probably have active disease (DAS≥2.4) after 3 months of DMARD therapy.
Funding Unrestricted grant from Pfizer bv. [0881-102217]
Disclosure of Interest None Declared