Article Text

Abstract
Background Obesity is associated with an increased risk of psoriasis; however, its potential impact on the risk of psoriatic arthritis (PsA) remains unclear.
Objectives To evaluate the association between body mass index (BMI) and the risk of PsA among patients with psoriasis from the general population.
Methods The authors conducted a cohort study using data from The Health Improvement Network, an electronic medical records database representative of the UK general population, collected between 1995 and 2010. The exposure of interest was the first BMI measured after psoriasis diagnosis and endpoints were incident cases of physician-diagnosed PsA. The authors estimated the RR of PsA after adjusting for age, sex, and histories of trauma, smoking and alcohol consumption.
Results Among 75 395 individuals with psoriasis (43% male, mean follow-up of 5 years, and mean age of 52 years), 976 developed PsA (incidence rate, 26.5 per 10 000 person-years). The PsA incidence rates increased with increasing BMI. Compared with psoriasis patients with BMI <25 kg/m2, the RRs for developing PsA were 1.09 (0.93–1.28) for BMIs from 25.0 to 29.9, 1.22 (1.02–1.47) for BMIs from 30.0 to 34.9 and 1.48 (1.20–1.81) for BMIs ≥35.0. In our secondary analysis among all individuals, regardless of psoriasis (∼2 million), the corresponding multivariate RRs tended to be stronger (1.0, 1.17, 1.57, 1.96; p for trend <0.001).
Conclusions This general population study suggests that obesity is associated with an increased risk of incident PsA and supports the importance of weight reduction among psoriasis patients who often suffer from the metabolic syndrome and obesity.
Statistics from Altmetric.com
Introduction
Psoriatic arthritis (PsA) is a progressive and often destructive inflammatory joint disease associated with psoriasis.1,–,3 The inflammatory arthritis of PsA adds substantially to the disease burden for psoriasis patients, with frequent joint destruction associated with cartilage erosions, bone damage and joint fusion. The negative impact of psoriasis may not be limited to its cutaneous or psychosocial manifestations,4 with emerging evidence indicating that psoriasis is associated with the metabolic syndrome5 ,6 and may lead to myocardial infarction,7 hypertension and diabetes.8 Despite these lifelong burdens of PsA, its causes and risk factors are poorly understood with a lack of large-scale data.
PsA is common in patients with psoriasis, affecting about 6–10% of psoriasis patients overall and substantially more patients with more extensive skin disease (up to 40%).1,–,3 In most patients with PsA, the symptoms do not develop until years after the onset of cutaneous psoriasis. As a result, patients with psoriasis represent a unique opportunity to study individuals at very high risk of developing a chronic inflammatory arthropathy (ie, PsA).1 To determine which patients with psoriasis are at the greatest risk of developing PsA, it is essential that risk factors be identified using robust epidemiological approaches.1
The adipose tissue in obese individuals is a site of overproduction of important inflammatory cytokines such as tumour necrosis factor α, interleukin 1, IL-6 and IL-8,9 ,10 and the resulting abnormal inflammatory milieu may contribute to the pathophysiology of psoriatic conditions.10 Obesity has been found to be associated with an increased risk of psoriasis,11 but its link to the risk of PsA remains less clear. Recent cross-sectional studies have found that PsA patients have a higher body mass index (BMI) than healthy controls,12 ,13 and patients with PsA have a 61% higher odds of having obesity than psoriasis patients.13 A case series study (n=197 for PsA) reported that recalled BMI at 18 years of age was associated with an increased risk of PsA, whereas current BMI was not.14
In this study, we examined the relation between BMI and the risk of incident PsA among 75 395 individuals with psoriasis from the general population.
Methods
Study population
The Health Improvement Network (THIN) is a computerised medical record database entered by general practitioners (GP) in the UK. Data on approximately 7.3 million patients are systematically recorded and sent anonymously to THIN. Because the National Health Service in the UK requires every individual to be registered with a GP regardless of health status, THIN is a population-based cohort representative of the UK general population. The computerised information includes demographics, details from GPs' visits, diagnoses from specialists' referrals and hospital admissions, results of laboratory tests, and additional health information recorded systematically including height, weight, blood pressure, smoking and vaccinations. The Read classification is used to code specific diagnoses, and a drug dictionary based on data from the Multilex classification is used to code drugs.12 ,13 Health information is recorded on site at each practice using a computerised system with quality control procedures to maintain high data completion rates and accuracy. Thus, THIN data represent routine medical practice in a population-based setting.15
Our primary study population consisted of psoriasis patients aged 20–89 years and enrolled in THIN at any time between January 1995 and May 2010 (n=75 395). Our secondary study populations included the cohort of individuals with or without psoriasis at baseline (N=2 026 139) and that limited to patients with incident psoriasis (n=27 980). Study cohort members had to be free of PsA before entering the study and were required to have two or more years of enrolment with the GP to help ensure exclusion of prevalent PsA. An individual's start (index) date corresponded to the date of the first recorded BMI after all these eligibility criteria were met. Members of this cohort were followed until the date of one of the following endpoints: PsA diagnosis, 90th birthday, death or end of study period, whichever came first.
Ascertainment of psoriasis and PsA
Validity of THIN Read codes for psoriasis has been documented based on a sample of 4900 psoriasis patients.16 With a 95% response rate in a GP survey for clinical confirmation of psoriasis, the Read codes for psoriasis in THIN showed a positive predictive value (PPV) of 90% of clinical confirmation. Therefore, we defined psoriasis based on its Read code in THIN.
Although validity of PsA Read codes has not been assessed in THIN, the positive predictive value (PPV) of a single code for PsA has been reported to be over 90% in another electronic medical record database.17 The use of diagnostic codes plus disease-modifying antirheumatic drug data definitions only slightly and significantly improved the specificity for each diagnosis, but at the cost of a dramatic reduction in sensitivity.17 Therefore, we defined PsA based on its Read diagnostic code in this study.
Assessment of exposure and covariates
Demographics, lifestyle factors and history of trauma were collected from the database before the index date. THIN lifestyle exposure variables have been collected prospectively and successfully used in previous analyses by confirming anticipated associations such as those among alcohol, BMI and gout;18 smoking and lung cancer;19 smoking, obesity and myocardial infarction;20 and alcohol and paroxysmal atrial fibrillation.21 Our exposure of interest was BMI, defined as the patient's body mass in kilograms divided by the square of his or her height in metres. We analysed the impact of the first recorded BMI after all these eligibility criteria were met (eg, the first BMI recorded after psoriasis diagnosis in our primary study cohort). We repeated our analysis using updated BMI as a time-varying exposure. History of trauma was included as a covariate as well, as this has also been reported to be associated with PsA.22 ,23
Statistical analysis
We calculated the eligible person-time of follow-up and incidence rates according to four BMI categories: <25, 25–29.9, 30–34.9 and ≥35 kg/m2, corresponding to the WHO's classification of normal weight, overweight, obese class I and obese class II or III, respectively.24 We used a Cox proportional hazards model to compute the multivariate RR for incident PsA adjusting for sex, age, smoking status (never/past/current), alcohol use (six categories) and history of trauma.
We repeated our analysis in the THIN population by additionally including those without psoriasis status (n=1 950 744). In this analysis, we examined the impact of including the diagnosis of psoriasis in the model, as BMI is a known risk factor for psoriasis and, thus, can act as a potential causal intermediate. We also repeated the analysis limited to patients with incident psoriasis (n=27 980). This allowed us to examine the potential impact of psoriasis duration on varying risks of PsA. For all RRs, we calculated 95% CIs. All p values are two-sided. All statistical analyses were performed using SAS software, V.9.2 (SAS Institute, Cary, North Carolina, USA).
Results
Our primary analysis included 75 395 psoriasis patients for a combined follow-up time of 368 302 person-years, during which 976 cases of incident PsA were diagnosed. The incidence rate of PsA in this population was 26.5 per 10 000 person-years. Table 1 summarises the baseline characteristics of the study cohort according to BMI.
Baseline characteristics according to body mass index for 75 395 patients with psoriasis
There were fewer men overall, which was most notable in the highest and lowest BMI categories. Lower BMI categories tended to have more current smokers and fewer past smokers. Other variables were similarly distributed across BMI categories.
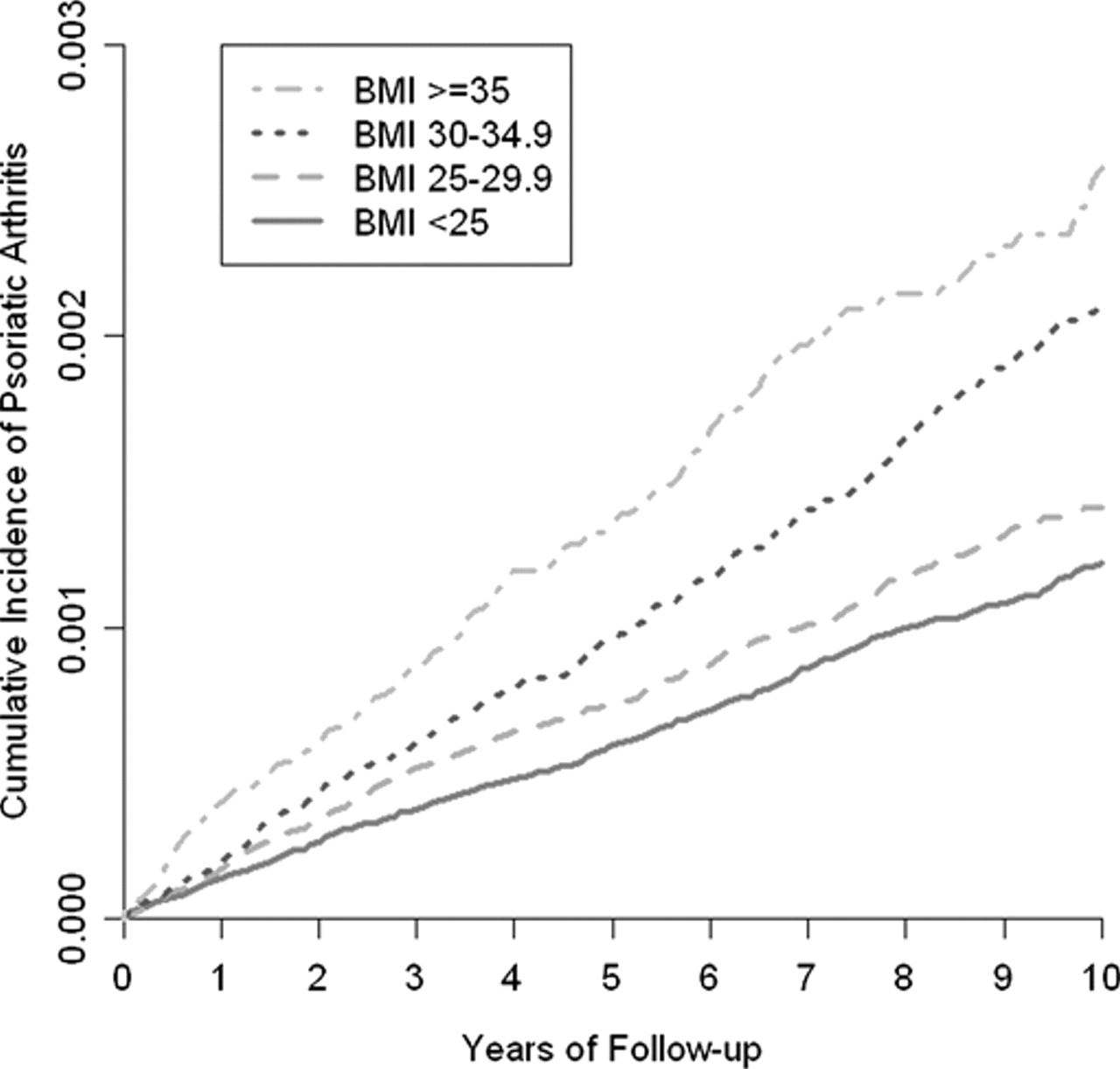
Higher categories of BMI were associated with an increased incidence of PsA (p for trend <0.001) (table 2 and figure 1). Compared with psoriasis patients with BMIs <25, those with BMIs of 25–29.9, 30.0–34.9 and ≥35.0 had age- and sex-adjusted RRs of 1.1, 1.24 and 1.52, respectively (p for trend <0.001). After adjusting for age, sex, smoking, alcohol consumption and history of trauma, these RRs were slightly attenuated but remained significant (p for trend <0.001) (table 2). When we repeated our analysis using updated BMI as a time-varying exposure, our results did not change materially (p for trend <0.001).

Time to psoriatic arthritis according to body mass index (BMI) category among patients with psoriasis (N=75 395).
RR of incident psoriatic arthritis by body mass index among patients with psoriasis
When we repeated the analysis by additionally including those without psoriasis status (n=1 950 744), higher categories of BMI were associated with an increased risk of PsA (p for trend <0.001) (table 3 and figure 2). Compared with individuals with BMIs <25, those with BMIs of 25–29.9, 30.0–34.9 and ≥35.0 had age- and sex-adjusted RRs of 1.17, 1.60 and 2.01, respectively, (p for trend <0.001), which were larger than those in our primary analyses. Further adjustment for the history of psoriasis in this secondary analysis modestly attenuated the association (1.0, 1.12, 1.46, 1.75; p for trend <0.001). When we limited our analysis to 27 980 patients with incident psoriasis, the RR for the highest BMI category was 1.65 (p for trend, 0.005).
{kind=link}
{kind=link}
Time to psoriatic arthritis according to body mass index (BMI) category in all eligible adults (N=2 026 139) with or without psoriasis at baseline.
RR for incident psoriatic arthritis by body mass index in the general population
Discussion
Our primary objective was to evaluate the association between BMI and the risk of PsA among patients with psoriasis from the general population. We found that increasing BMI among patients with psoriasis was associated with an increasing risk of incident PsA, demonstrating a dose-response relation. When we examined the risk in all eligible individuals regardless of psoriasis status, the magnitude of association became larger. These associations were independent of other potential confounders such as age, sex, trauma, smoking and alcohol intake. These data provide the first general population-based evidence that obesity is associated with an increased risk of developing PsA among psoriasis patients as well as in the general population.
A recent cross-sectional study reported that PsA patients have a higher BMI than psoriasis patients.13 Another study based on psoriasis patients recruited consecutively from the dermatology clinic of the University of Utah reported an independent association with recalled BMI at age 18, but no such associations with current BMI among psoriasis patients.14 However, as the current BMI data in that study were measured after the study recruitment when PsA status was determined, they reflect adiposity levels after the onset of PsA (as opposed to BMI before the onset of PsA). Furthermore, because the recalled BMI data at age 18 do not take into account BMI changes that occurred from age 18 leading up to and following the development and diagnosis of psoriasis, its utility for predicting the future risk of PsA based on adiposity status of psoriasis patients is unclear. Our results filled this knowledge gap by examining the relation between BMI after psoriasis diagnosis (and before PsA onset) and the risk of PsA.
Potential explanations for this increased risk for PsA among obese psoriasis patients include the inflammatory load associated with adiposity, contributing further to that associated with their underlying psoriatic condition. Obesity is associated with an overproduction of inflammatory cytokines including IL-1, IL-6, IL-8 and tumour necrosis factor α, and there is a correlation between the level of adiposity and the measured peripheral levels of associated inflammatory cytokines.9 ,10 Randomised trial data showing beneficial additive effects of weight loss25 and case reports of psoriasis clearing with reducing obesity26,–,28 suggest that this inflammatory milieu provided by the overabundance of adipose tissue may be important in the pathogenesis of psoriatic conditions. An alternative speculation for the increased risk observed here could be that mechanical wear, secondary to obesity, could trigger PsA in load-bearing joints, with subsequent spread of the inflammatory arthritis to other joints.
Our findings may have practical implications for the management of psoriasis patients, as PsA is common in these patients, affecting about 6–10% of psoriasis patients overall and substantially more patients with extensive skin disease (up to 40%).1,–,3 Thus, a modifiable risk factor, such as obesity, requires a relatively small number needed to treat among psoriasis patients compared with the general population context with a lower background risk of developing PsA. Although a randomised trial would be needed to definitively establish the usefulness of weight reduction in reducing the risk of PsA, this type of study may be difficult to perform, given the large number of psoriasis patients and trial durations necessary for sufficient cases of PsA to occur, the high costs and anticipated ethical issues. Meanwhile, as weight reduction in obese individuals has multiple health benefits, including reduced cardiovascular and mortality risks, these benefits appear all the more relevant for obese psoriasis patients to help prevent their excess risk of PsA along with co-morbidity and mortality complications.
The strengths and limitations of our study deserve comment. This study was performed using a large UK general practice database; therefore, findings are likely to be applicable to the general population. While the designs of previous studies on the topic made it difficult to establish the temporal relations between BMI and the risk of PsA, our study design, including the time-point of exposure measurement and the incident case outcome analysis, enabled us to establish temporal relations between these factors.13 ,14 Uncertainty surrounding diagnostic accuracy is a potential concern in studies that identify cases from administrative databases. However, our databases are actually electronic medical records used for patients' care, thus the overall accuracy is expected to be higher, as reflected in many validation studies of important outcomes.16 ,29,–,33 As is well reflected in the high PPV estimates for a psoriasis code in THIN (90%),16 and for a PsA code in another electronic medical record database (>90%),17 our cohort definition (psoriasis patients) and outcome (PsA) belong to this group of ‘specific’ diagnoses, likely due to the characteristic skin lesions of psoriasis and the clinical context in which PsA is diagnosed. PsA is among those specific diagnoses that are usually first made or confirmed by rheumatologists (unlike rheumatoid arthritis (RA)).17 This is likely because both referring physicians and patients are not as familiar with this diagnosis as they are with other common types of arthritis (eg, RA or osteoarthritis) and there are no widely available blood tests that flag the diagnosis of PsA (eg, rheumatoid factor or anticyclic citrullinated protein for RA).
In conclusion, this general population study suggests that obesity is associated with an increased risk of incident PsA and supports the importance of weight reduction among psoriasis patients who often suffer from the metabolic syndrome and obesity.
References
Footnotes
-
Funding This work was supported in part by grants from the NIAMS (P60AR047785) and Boston University School of Medicine. The funding sources had no role in the design, conduct or reporting of the study, or in the decision to submit the manuscript for publication.
-
Competing interests None.
-
Ethical approval The current study was approved by the NHS Research Ethics Committee (09/H0305/75).
-
Provenance and peer review Not commissioned; externally peer reviewed.