Article Text

Abstract
Objective To evaluate changes in baseline patient characteristics and entry criteria of randomised, controlled studies of tumour necrosis factor alpha (TNFα) inhibitors in rheumatoid arthritis (RA) patients.
Methods A systematic literature review was performed using predefined inclusion criteria to identify randomised, double-blind, controlled trials that evaluated TNFα inhibitors in adult RA patients. Entry criteria and baseline clinical characteristics were evaluated over time for methotrexate-experienced and methotrexate-naive study populations. Enrolment start date for each trial was the time metric. The anchor time was the study with the earliest identifiable enrolment start date.
Results 44 primary publications (reporting the primary study endpoint) from 1993 to 2008 met the inclusion criteria. Enrolment start dates of August 1993 and May 1997 were identified as time anchors for the 37 methotrexate-experienced studies and the seven methotrexate-naive studies, respectively. In methotrexate-experienced trials, no significant change was observed over the years included in this study in any inclusion criteria (including swollen joint counts and C-reactive protein (CRP)), but a significant decrease over time was observed in the baseline swollen joint count, CRP and total Sharp or van der Heijde modified Sharp score, but not in baseline tender joint counts. In the methotrexate-naive studies, significant decreases over the years were observed in swollen joint and tender joint inclusion criteria, but not in baseline tender joint count, baseline CRP, CRP inclusion criteria or baseline total Sharp or van der Heijde modified Sharp score.
Conclusion Inclusion criteria and baseline characteristics of RA patients enrolled in studies of TNFα inhibitors have changed, with more recent trials enrolling cohorts with lower disease activity, especially in methotrexate-experienced trials.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://ard.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
In the early 1990s, there was a paradigm shift in the treatment of patients with rheumatoid arthritis (RA).1 Before this period, patients with RA were treated employing the ‘pyramid’ approach, in which non-steroidal anti-inflammatory drugs were used first, followed by disease-modifying antirheumatic drugs (DMARD) and steroids as the disease became more severe. The paradigm shift occurred when early intensive treatment was emphasised. Around this time, researchers also discovered the importance of proinflammatory cytokines in the pathogenesis of RA,2 3 which led to the first therapeutic use of cytokine inhibition to treat patients with RA.4 Several biological agents have now been approved by regulatory authorities in many countries for the treatment of patients with RA, including abatacept, adalimumab, certolizumab, etanercept, golimumab, infliximab, rituximab and tocilizumab.
The revised approach to the treatment of patients with RA over the past decade, which included early recognition5 and early DMARD start6 and the availability of an increasing number of treatment options,7 8 would be expected to result in fewer patients with severe disease in the population.9 10 Indeed, data of recent observational studies have suggested that the severity of RA has been decreasing over time.11 12 This has implications for clinical trials designed to evaluate the efficacy and safety of new therapeutics,13 however, it is not clear if this trend is the result of the disease becoming milder or the management of the disease is improving.
The purpose of this investigation was to evaluate the changes in inclusion criteria and baseline characteristics of patients in randomised controlled studies involving tumour necrosis factor alpha (TNFα) inhibitors in patients with RA. We hypothesised that the disease activity of patients who participate in these studies has decreased over time, reflecting the larger trends in the population of patients as a whole.
Methods
A systematic literature search was conducted using MEDLINE, EMBASE and the Cochrane Library (1988 to December 2008); clinical study reports (for golimumab only, these have since been published);14 15 citation lists, published systematic reviews and health technology assessments (1988–2008); internet sites for the US Food and Drug Administration, ClinicalTrials.gov and ClinicalStudyResults.org; and abstracts presented at the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) congresses (2004–8).
Databases were searched using specific search strings, which included some of the following key terms (synonyms and combinations): rheumatoid arthritis, tumour necrosis factor, tumour necrosis factor receptors, anti-tumour necrosis factor, adalimumab, etanercept, infliximab, certolizumab and golimumab. Search filters were used to identify randomised controlled trials in MEDLINE and EMBASE. Search limits (provided by Xcenda) were placed in MEDLINE and EMBASE to limit the studies to the date ranges indicated above, English language and humans (from Xcenda). The last search was conducted on 13 March 2009. Two reviewers independently inspected the titles and abstracts from the initial literature search to identify potentially relevant publications.
Predefined inclusion criteria were applied to the results of the literature search in a hierarchical manner. First, only randomised, double-blind, controlled trials were included that compared adalimumab, etanercept, certolizumab, golimumab or infliximab with any other agent, including placebo or alternative doses of the agent, in adult patients with RA. Second, only trials that were published in a peer-reviewed medical journal, available as a complete study report (for studies that had completed enrolment), or abstracts with primary endpoints that had been presented at ACR or EULAR congresses were included. Third, only trials with at least 4 weeks of follow-up and at least 25 patients were included. Single-dose studies were included if the duration of follow-up exceeded 4 weeks.
Studies were excluded if they were designed to evaluate patients with conditions other than RA (eg, juvenile RA, Crohn's disease, psoriatic arthritis or ankylosing spondylitis), had non-randomised trial designs (eg, observational studies, open-label studies, non-comparative studies, case reports, systematic reviews or health technology assessments), or were preclinical (animal) or phase I studies. Studies that pooled patients from different disease cohorts were also excluded. All publications identified as potentially relevant by at least one reviewer were retrieved. The reviewers discussed publications that were considered to be potentially relevant and came to a consensus on inclusion based on the inclusion criteria.
Data extraction
One reviewer examined all publications for duplication of study populations. After removing duplicates, the study characteristics, including study design, patient enrolment dates, baseline demographics, clinical characteristics and relevant clinical outcomes, were recorded for all studies. Publications were also identified as studies having either methotrexate-experienced or methotrexate-naive populations.
Unpublished study enrolment dates were obtained using the study identification number from follow-up publications, ClinicalTrials.gov, fda.gov, Trial Trove, Prous Integrity, Adis Clinical Trial and Adis R&D Insight. If study enrolment dates were unavailable from these resources, the publication's primary authors were contacted to obtain the information. All other missing information was noted as not available and was not reported in subsequent analyses.
Data analysis
We evaluated the inclusion criteria and baseline characteristics of the patients from studies over the years. The time point for each study was the enrolment start date. The anchor time point was the earliest enrolment start date for the first study. Time points for all other studies were measured (in months) from the anchor time point. Regression analysis was used to evaluate changes in inclusion criteria and baseline characteristics over time. The hypothesis of coincidence and equality of intercept was tested for the linear models at a significance level of α<0.05.
If baseline descriptive statistics for the total study population were not available, a weighted mean was calculated for continuous variables by multiplying the mean value for each study arm by the number of patients in the study arm, summing these values, then dividing by the total number of patients in the study.
We conducted a sensitivity analysis to account for missing enrolment dates or baseline characteristics. The mean elapsed time from enrolment start date to publication date for all studies with known values was subtracted from the publication date of studies with missing enrolment start dates to obtain an estimated enrolment start date. If the estimated enrolment start date was before the anchor enrolment start date, the anchor date was used.
Data from primary publications (those with primary endpoints) were used for subsequent analysis and study entry criteria and baseline clinical characteristics were evaluated over time for methotrexate-experienced and methotrexate-naive study populations using regression analysis.
Results
A total of 2333 abstracts/manuscripts from MEDLINE, EMBASE, the Cochrane Library and other sources (bibliographies from health technology assessments, review articles, etc.) were identified. Duplicate and extraneous publications from each source were removed using Reference Manager, leaving 1407 unique manuscripts for etanercept (n=411), adalimumab (n=412), infliximab (n=537), certolizumab (n=38) and golimumab (n=9). Figure 1 shows the results of the filtering process in which publications were selected for inclusion in the analysis. Of the 1407 unique publications obtained during the medical literature database search, 1256 were excluded because they were not double-blind, randomised, controlled studies, did not include the intervention of interest, did not include the population of interest, had less than 4 weeks of follow-up (n=4) or had a sample size of fewer than 25 patients. The remaining 151 publications were retrieved for detailed evaluation. A total of 1435 abstracts were identified during the ACR and EULAR congress search. Of these, 1388 abstracts were excluded because they did not provide sufficient information, had results that were subsequently published in the peer-reviewed literature and included in the medical literature database search, were not double-blind, randomised, controlled studies; or did not evaluate anti-TNFα agents in RA. The remaining 47 abstracts were retrieved for more detailed evaluation.

Results of literature search and process of eliminating publications. *two clinical study reports that were included for golimumab. These studies have since been published.14 15 ACR, American College of Rheumatology; DB, double blind; EULAR, European League Against Rheumatism; RCT, randomised controlled trial; TNF, Tumour necrosis factor.
Studies of anti-TNFα agents
A total of 88 double-blind, randomised, controlled studies of anti-TNFα agents met the inclusion criteria. From these, 44 primary publications were identified that reported the results of a priori primary study endpoints, including eight adalimumab studies, four certolizumab studies, 17 etanercept studies, five golimumab studies and 10 infliximab studies (table 1). Of the primary studies, 37 were conducted in methotrexate-experienced patient populations and seven were conducted in methotrexate-naive patient populations. From these, five studies were identified that provided x-ray data for methotrexate-experienced patients and five studies provided x-ray data for patients who were methotrexate-naive. Time anchors were Elliott et al16 (enrolment start date August 1993) for methotrexate-experienced studies, and Bathon et al22 (enrolment start date May 1997) for methotrexate-naive studies.
Characteristics of primary publications for biological anti-TNFα agents
Table 2 summarises the changes in inclusion criteria and baseline characteristics over time for anti-TNFα studies in methotrexate-experienced and methotrexate-naive patient populations.
Changes in inclusion criteria and baseline characteristics over time for methotrexate-experienced and methotrexate-naive populations
In the studies with methotrexate-experienced populations, no significant difference over time was observed in any inclusion criteria (tender or swollen joint counts or C-reactive protein (CRP; figure 2). However, significant decreases (or trends) over time were observed in baseline swollen joint count (p=0.06, R2=0.17; figure 2B) and CRP (p=0.03, R2=0.27; figure 2F), but not in baseline tender joint counts (figure 2D). Sensitivity analyses confirmed the findings in the base case for each measurement.

Results for entry criteria and actual mean baseline values in methotrexate-experienced patients over time. CRP, C-reactive protein; SJC, swollen joint count; TJC, tender joint count.
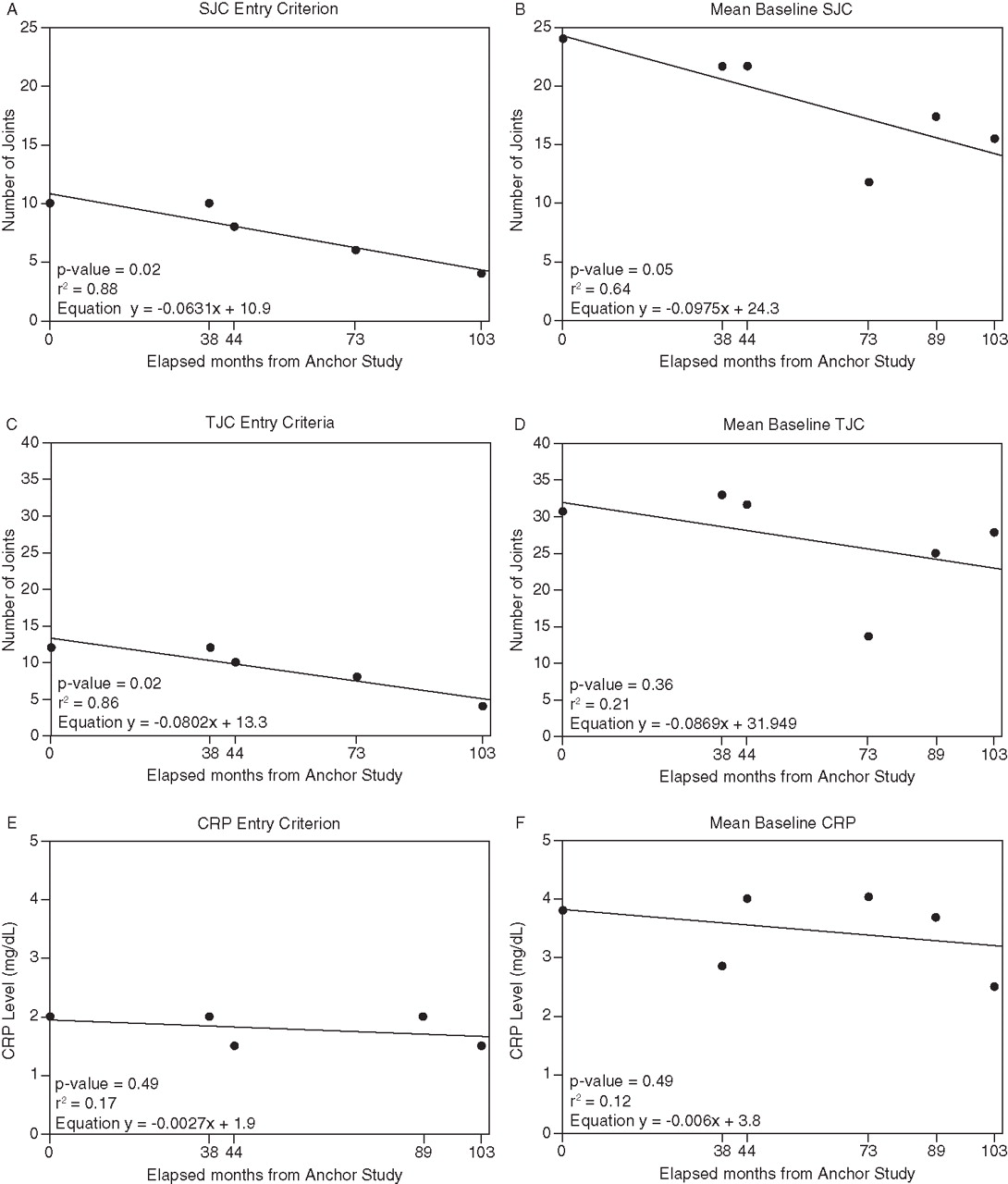
In the studies with methotrexate-naive populations, significant decreases over time were observed in swollen joint inclusion criteria (p=0.02, R2=0.88; figure 3A) and mean baseline swollen joint count (p=0.05, R2= 0.64; figure 3B) and tender joint inclusion criteria (p=0.02, R2=0.86; figure 3C), but not in baseline tender joint count, CRP or CRP inclusion criteria (figure 3D–F). Sensitivity analyses were unnecessary because enrolment start dates were available for all methotrexate-naive studies.

Results for entry criteria and actual mean baseline values in methotrexate-naive patients over time. CRP, C-reactive protein; SJC, swollen joint count; TJC, tender joint count.
In the five studies of methotrexate-experienced patients that included x-ray data, the mean baseline Sharp or van der Heijde modified Sharp score decreased significantly over time (p=0.01, R2=0.93; figure 4A). Indeed, numerically this difference was quite dramatic, accounting for more than a 50% reduction over approximately 10 years. There was no significant decline in the mean baseline van der Heijde modified Sharp score in the studies of methotrexate-naive patients (p=0.90, R2=0.01; figure 4B). Annual radiographic progression (another measure of disease severity) for each of these studies was estimated by dividing the mean baseline Sharp or van der Heijde modified Sharp score by the mean disease duration. This estimated progression was then compared with the actual progression observed in the control (methotrexate±placebo) group for each of the trials at 52 weeks. Comparisons were made for methotrexate-experienced and methotrexate-naive studies separately (figure 5A,B). While the annualised progression rates did not show a consistent pattern over the years, the actual progression observed over 1 year in the control groups was much lower than the estimated annualised progression rate for the more recent trials. The annualised progression rate, which predicted progression rate very well in control groups in older trials like ATTRACT and others,57,–,60 does not seem to predict the progression rate in the control groups at all in the more recent trials.
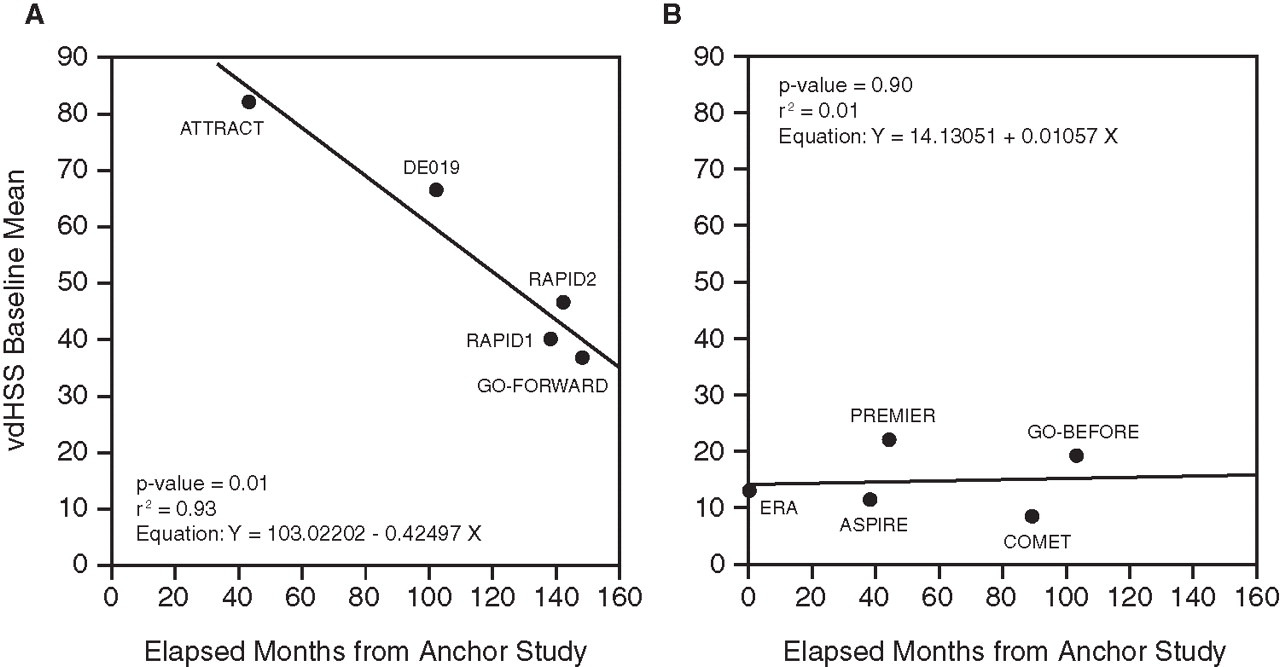
Results for change in mean baseline total Sharp or van der Heijde modified Sharp score over time (months elapsed since anchor study) for (A) Methotrexate-experienced (anchor study 1993) and (B) Methotrexate-naive (anchor study 1997) patients. vdHSS, van der Heijde Sharp score.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Estimated yearly progression versus actual radiographic progression at week 52 in methotrexate (MTX)-experienced (*actual 1 year values in the RAPID2 and GO–FORWARD study were measured at week 24 and extrapolated (doubled) to 1 year) and methotrexate-naive studies (*actual radiographic progression (at 1 year) was measured at week 54 in the ASPIRE study and week 52 in all other studies).
Discussion
The results of this study show that the characteristics of patients who were enrolled in studies of TNFα inhibitors in RA have changed over the years. Since 1993, with the first randomised, controlled study of an anti-TNFα agent, disease characteristics of patients who participate in these studies have become generally less severe. Among patients in methotrexate-experienced studies, significant decreases in baseline swollen joint count and CRP were observed. The most dramatic change was seen in baseline radiographic scores, which decreased by more than 50% over just one decade. This change relates to both baseline scores and estimated annual progression rates and has been suggested by others.57,–,60 Despite these observations, the determination of whether these changes are clinically meaningful is beyond the scope of the current study.
In line with the decline in swollen joint count and CRP at baseline, which are the major variables associated with the progression of joint damage,61 62 these data suggest that the standard of care (for the pool of patients from which clinical trial patients are obtained) has improved during the past decade.63 The decrease in baseline disease characteristics was less pronounced in the methotrexate-naive (early RA) population than the methotrexate-experienced (more established and longer standing disease) population, an observation suggesting that the general characteristics of RA at presentation may not have changed over the years. Methotrexate-naive early RA patients may reflect the clinical characteristics of RA at presentation/diagnosis more closely with minimal influence of treatments received, whereas the clinical characteristics of more established methotrexate-experienced RA patients may be influenced by the treatments received. The changes in the clinical characteristics of patients being enrolled in randomised clinical trials may thus be more of a function of improved standard of care and change in the treatment paradigm of RA (for the pool of patients from which clinical trial patients are recruited). However, while changes in demographics and general health aspects may contribute to less severe disease,12 better care for patients with RA may be the major reason for this observation.9 Other possibilities must also be considered; for example, investigative sites are recruiting higher proportions of patients with less severe disease to meet the demands of an increased number of clinical trials being conducted, the changing geographical distribution of clinical trial sites, etc. However, the current study did not allow for the assessment of such possibilities.
There are several limitations to our study. First, we focused on TNFα inhibitors rather than on all clinical trials performed during the time of observation. However, the more recent randomised controlled trials for abatacept, rituximab and tocilizumab64,–,66 employed the Genant-modified Sharp score, which has a much lower total value than the Sharp or van der Heijde modified Sharp score64 and, therefore, comparability would be impaired. Moreover, the inclusion of data from the studies of newer TNFα inhibitors, including certolizumab and golimumab,14 46 62 ensured the integration of studies performed at the same time period as these other trials. Second, the number of studies on early RA patients was much smaller than on established RA patients with inadequate response to methotrexate; consequently, the interpretation of these data has to be seen with the respective caution. Third, we did not assess publications from registries; however, patients evaluated in registries, while constituting ‘real life patients’, are of much broader range, do not have to fulfil trial-like inclusion criteria, are dependent on the reimbursement status in the individual countries, and are thus more heterogeneous. Fourth, the geographic distribution of patients was not reported consistently in detail in the manuscripts reviewed. Although clinical trials are currently being conducted in more regions and countries compared with the previous decade, due to the unavailability of consistent data from all studies reviewed, we were not able to evaluate the change in geographic distribution of patients in these studies. Fifth, a majority of the studies included in these analyses did not provide adequate and consistent data regarding duration of disease, which limited the assessment of changes in disease duration of patients enrolled in clinical trials over the years. However, the limited data available to be analysed did not show any specific pattern in disease duration over the years. Disease duration of RA has been shown to impact clinical characteristics and responsiveness to treatment by others.67 Finally, the patient populations studied are from randomised clinical trials; and thus, the changes observed over 16 years may reflect the changes in patient populations of investigative sites looking for patients fulfilling inclusion criteria for clinical trials rather than the entire RA population, at least for sites in the US, Canada and western Europe.63 68
Despite the limitations, the trends described above have several implications. They suggest that the overall disease characteristics of the population of patients with RA from which these subjects are recruited have become less severe over the years. During the time period of this study, the standard of care (treatment paradigm) of RA has changed, emphasising the earlier diagnosis and earlier and more intensive use of combination therapy,69 70 which results in fewer patients with persistent severe disease activity and advanced disability. We also acknowledge that trial centres that have limited access to biological therapies have improved their therapeutic approaches to RA by virtue of the many studies published on the advantage of early and intensive therapy. Indeed, mean methotrexate doses have increased when compared with the anchor study,16 and studies of methotrexate-naive patients have employed much higher doses than were used in the anchor study22 or studies published around the same time on leflunomide trials.71 In line with this, the results of long-term observational studies have suggested that the health status of patients with RA has improved.9 12
Whereas multiple factors may be responsible for this change in the patient populations enrolled in clinical trials for RA, the change in standard of care for RA may be the single most important factor. The standard of care now emphasises early intensive treatment, and RA patients receive methotrexate earlier and in higher doses than patients did more than a decade ago, during the clinical trials for etanercept and infliximab. The changes in the treatment paradigm for RA, coupled with the changes in the populations of patients enrolled in clinical trials should be considered when reviewing new studies on all therapies for RA. These changes in the baseline characteristics will also need to be considered when designing clinical trials in RA. They also have to be accounted for when performing meta-analyses of clinical trials.72
Acknowledgments
The authors thank the patients, investigators and study personnel who made these trials possible. The authors thank Kirsten Schuck and Mary Whitman, PhD, of Centocor Ortho Biotech Inc, a wholly owned subsidiary of Johnson & Johnson, and Scott Newcomer of Cephalon, formerly of Centocor Ortho Biotech, who helped prepare the manuscript.
References
Footnotes
↵* Current affiliation of the author
-
Funding This study was funded by Johnson & Johnson.
-
Competing interests MUR, JB, MKD, ECH, TG and SP were all employees of Johnson & Johnson at the time of the study and own Johnson & Johnson stock options. ELM has been a paid consultant and advisory board member and is an investigator for Johnson & Johnson/Centocor. PGC has received consulting fees, speaking fees and/or research grants from Astra Zeneca, Bristol-Myers Squibb, Centocor; Merck, Sharpe and Dohme, Novartis, Roche and Pfizer. EK has received funding research from Abbot Laboratories, Amgen, AstraZeneca Pharmaceuticals LP, Bristol-Myers Squibb, Centocor, F. Hoffman-LaRoche, Novartis Pharmaceuticals Schering-Plough Corporation, UCB and Wyeth Pharmaceuticals. He has consulting agreements/advisory board memberships with Abbott Laboratories, Amgen, Bristol-Myers Squibb Company, Centocor, F. Hoffman-LaRoche, Genentech, Schering-Plough Corporation, UCB and Pfizer Pharmaceuticals. He has speaker honoraria agreements with Abbott Laboratories, Amgen, Bristol-Myers Squibb Company, F. Hoffman-LaRoche, Schering-Plough Corporation and Pfizer Pharmaceuticals. JSS has received grant support from and/or provided expert advice to Abbott, Amgen, BMS, Centocor, MSD, Pfizer, Roche, UCB and Sanofi-Aventis. DA and DvdH have nothing to declare.
-
Provenance and peer review Not commissioned; externally peer reviewed.