Article Text

Statistics from Altmetric.com
Purpose
Treatment with hydroxychloroquine (HCQ) is associated with a decreased risk of thrombosis in APLS. In vitro, HCQ decreases the binding of aPL-beta2 glycoprotein I complexes to phospholipid bilayers and reduces aPL levels in clinical assays. The time-dependent effects of HCQ on aPL in SLE patients have not been studied extensively. We therefore investigated the association of changes in aPL titres over time with HCQ therapy.
Method
We identified all SLE patients followed at a tertiary care centre with aPL or lupus anticoagulant (Lac), which had been checked at least twice between 2002 and 2009. At baseline, patients were defined as aPL/Lac− if they tested negative for both aPL and Lac, and as aPL/Lac+ if they tested positive for either aPL or Lac. We used the standard laboratory cut-offs for the above definitions. In the aPL/Lac+ group an ‘event’ was defined as aPL and/or Lac conversion from positive to negative. In the aPL/Lac− group an ‘event’ was defined as aPL or Lac conversion from negative to positive. ‘Time to event’ was defined as the number of months from baseline to censoring or conversion. Patients were defined as HCQ+ if they were being treated with HCQ at the time of the event, and HCQ− if they were not. Kaplan–Meier graphs were generated separately for the aPL/Lac+ and aPL/Lac− groups.
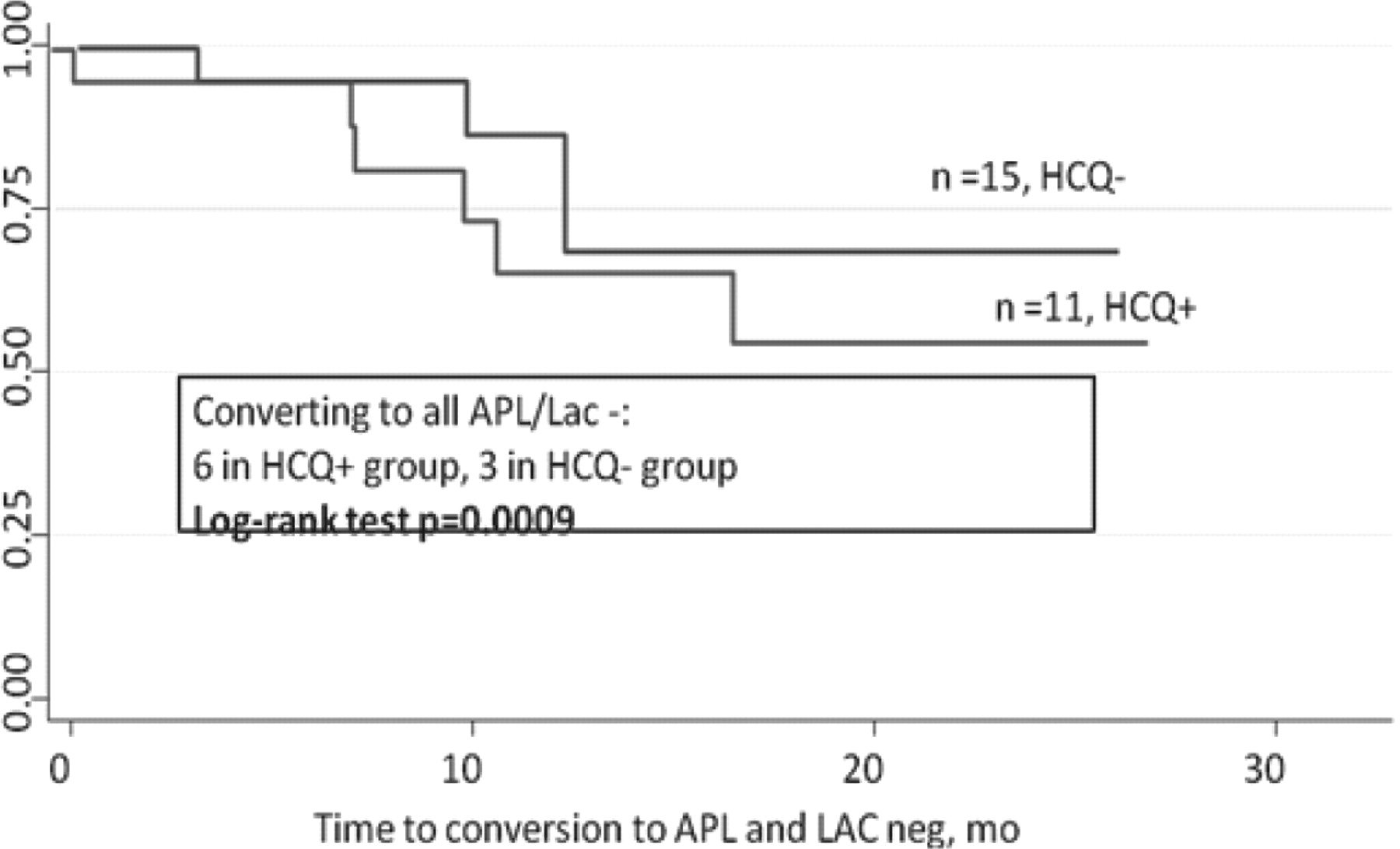
Kaplan-Meier estimates for APL/Lac neg patients at baseline

{kind=link}
{kind=link}
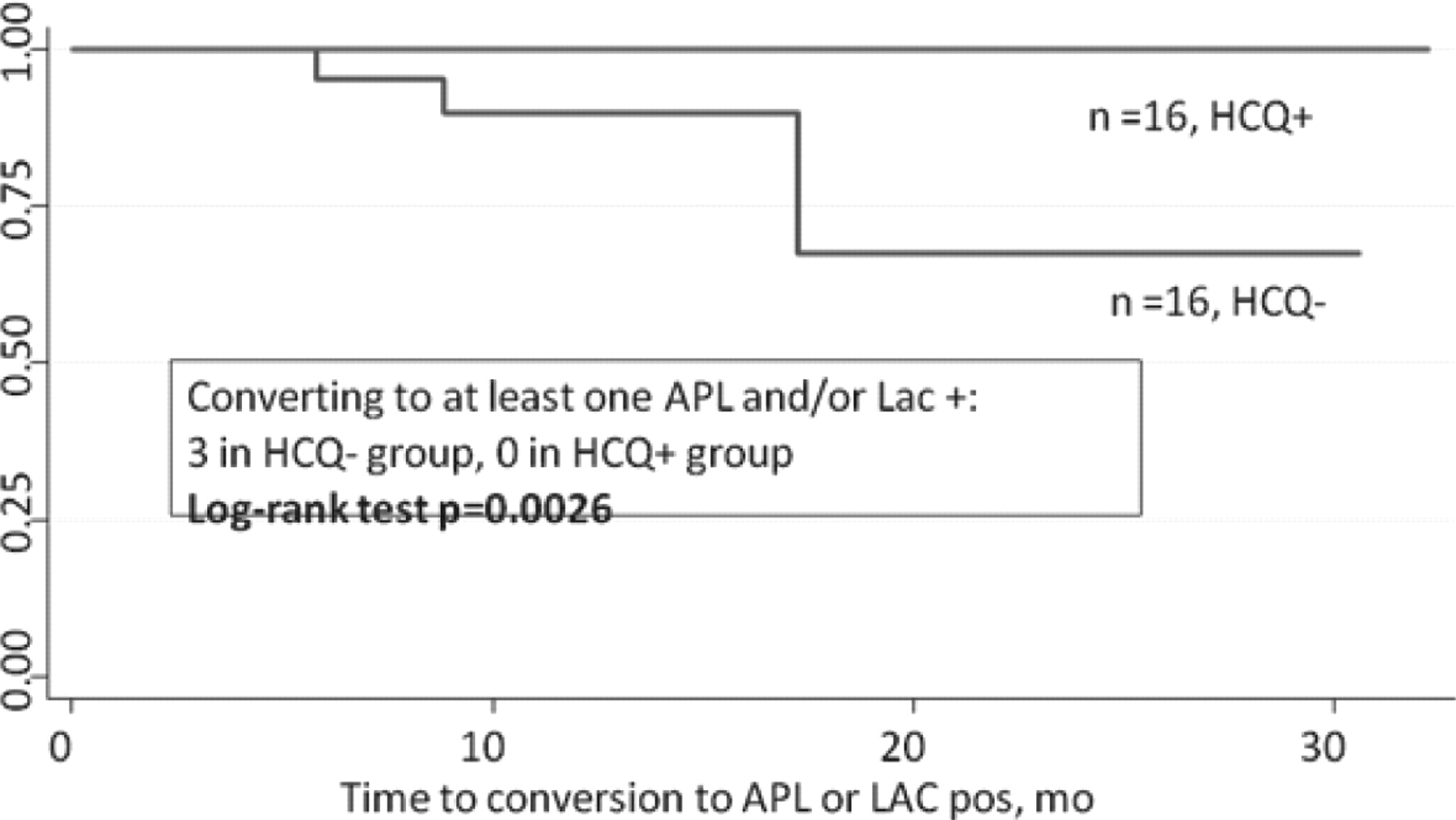
Kaplan-Meier estimates for APL/LAC pos patients at baseline
Results
Eighty-four patients met the above inclusion criteria: 31 HCQ−, 27 HCQ+, and 26 missing HCQ data. HCQ+ and HCQ− groups were similar in terms of age, race, gender, as well as platelet counts, serum creatinine, C3, C4, and anti-dsDNA titres at the event time. During the course of follow-up, HCQ+ patients were more likely to be prescribed prednisone (p=0.004) and/or DMARDs including cyclophosphamide, azothioprine, or mycophenolate mofetil (p=0.02). Twenty (64%) patients in the HCQ− group and 9 (33%) in the HCQ+ group (p=0.02) were placed on warfarin during the course of follow-up, suggesting that there was a higher rate of thrombotic events in the HCQ− group. Thirty-two patients, 16 (50%) HCQ+ and 16 (50%) HCQ−, were APL/Lac− at baseline. Three (9%) patients became APL/Lac+. All 3 were in the HCQ– group. The differences were statistically significant by the log-rank test (p=0.0026). Twenty-six patients, 11 (42%) HCQ+ and 15 (58%) HCQ−, had at least one APL/Lac+ at baseline. Six (55%) were on HCQ and 3 (20%) were not on HCQ at the time of conversion to all APL/Lac−. The differences were statistically significant by the log-rank test (p=0.0009). The mean decrease of APL antibody levels was 10.9 GPL in HCQ− group and 20.25 GPL in the HCQ+ group.
Conclusion
Despite several limitations associated with this retrospective analysis, our data indicate that hydroxychloroquine may play a role in decreasing APL antibody levels in APL positive patients and maintaining low APL levels in APL negative patients. This observation is consistent with previously published laboratory data. Long-term prospective studies in a larger group of patients are needed to confirm this observation. If confirmed, hydroxychloroquine may be used to treat APLS in the future.