Article Text

Abstract
Background Anti-tumour necrosis factor (anti-TNF) therapy has been associated with reports of rapid severe progression of rheumatoid arthritis-associated interstitial lung disease (RA-ILD). However, reports also exist of favourable responses to anti-TNF therapy in patients with ILD. The aim of this study was to examine the influence of anti-TNF therapy on mortality in patients with pre-existing RA-ILD.
Methods Using data from the British Society for Rheumatology Biologics Register, a national prospective observational study, 367 patients with pre-existing RA-ILD were identified (299 treated with anti-TNF therapy and 68 treated with traditional disease-modifying antirheumatic drugs (DMARDs)).
Results 70/299 patients (23%) in the anti-TNF cohort died after a median follow-up of 3.8 years compared with 14/68 (21%) in the DMARD cohort after a median follow-up of 2.1 years. The mortality was 68 deaths/1000 person years (pyrs) (95% CI 53 to 86) in the anti-TNF cohort and 92/1000 pyrs (95% CI 50 to 155) in the DMARD cohort, generating an age- and sex-adjusted mortality rate ratio (aMRR) of 1.26 (95% CI 0.69 to 2.31). After further adjustment for potential confounders, the aMRR fell to 0.81 (95% CI 0.38 to 1.73) for the anti-TNF cohort compared with the DMARD cohort. RA-ILD was the underlying cause of death in 15/70 (21%) and 1/14 (7%) patients in the anti-TNF and DMARD cohorts, respectively.
Conclusion The mortality in patients with RA-ILD is not increased following treatment with anti-TNF therapy compared with traditional DMARDs. The proportion of deaths attributable to RA-ILD is higher in patients treated with anti-TNF therapy, although reporting bias may exist.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://ard.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
Introduction
Rheumatoid arthritis (RA) is associated with extra-articular manifestations in around 40% of patients.1 2 Respiratory manifestations are common and include airways, pleural and interstitial disorders. Rheumatoid arthritis-associated interstitial lung disease (RA-ILD) is a non-neoplastic disorder resulting from damage to the lung parenchyma by varying patterns of inflammation and fibrosis.3 Estimates of prevalence vary widely from 1% to 80%, the broad range reflecting differences in disease definitions and populations studied.4
RA-ILD is associated with a significant mortality. Estimates of 2-year mortality in patients with prevalent disease are >20%.5 6 RA-ILD is the direct cause of death in 4% of unselected patients with RA, while featuring on the death certificate in 6%.7 Following the introduction of anti-tumour necrosis factor (anti-TNF) therapies for patients with RA, there have been a number of case reports and case series documenting either a rapid progression of pre-existing RA-ILD or the development of new-onset interstitial disease. Such reports exist for each of the three currently licensed anti-TNF therapies: infliximab (INF), etanercept (ETA) and adalimumab (ADA).8,–,14 Nineteen out of 20 of these cases of progressive RA-ILD occurred less than 3 months after starting anti-TNF therapy, providing a persuasive argument for causality despite the limitations of spontaneous pharmacovigilance. Eight of the 20 cases were fatal. These reports have led to the inclusion of ILD as an ‘undesirable effect’ in the Summary of Product Characteristics for each of the three drugs. However, in direct contrast, there are also reports of anti-TNF therapy stabilising or improving lung function in patients with RA-ILD.15,–,17 These paradoxical effects are, however, supported by animal models of both profibrotic and antifibrotic effects of TNF in the lung.18
The aim of this study was to examine the influence of anti-TNF therapy on all-cause and ILD-specific mortality in patients with pre-existing RA-ILD.
Methods
Patients
The subjects for this analysis were participating in a large national prospective observational study, the British Society for Rheumatology Biologics Register (BSRBR). The methods of patient recruitment and follow-up have been described in detail elsewhere.19 Briefly, the study was established in 2001 to examine the long-term safety of biological drugs in patients with RA. Recruitment targets of 4000 patients with RA treated with each of the three anti-TNF drugs, as well as 4000 biologic-naïve patients with active RA receiving standard disease-modifying antirheumatic drug (DMARD) therapy, were set in the first years of the study. UK national guidelines recommend that anti-TNF drugs are reserved for patients with active RA (defined as a 28-joint count disease activity score (DAS28) >5.1) despite previous therapy with at least two DMARDs, one of which should be methotrexate,20 and that ‘any clinician prescribing these medications must (with the patient's permission) undertake to register the patient with the BSRBR and forward information on dosage, outcome and toxicity on a six-monthly basis'.21 Recruitment targets for the ETA cohort were met in 2005, for the INF cohort in 2007 and for the ADA cohort in 2008. No accurate figures for anti-TNF penetration in the UK RA population exist, although estimates of around 7% have been suggested.22 Before recruitment targets were met, we estimated that >80% of anti-TNF treated patients with RA in the UK were registered on the BSRBR.
Anti-TNF cohort
Analysis was restricted to patients registered with the BSRBR with a physician diagnosis of RA who were commencing an anti-TNF drug as their first biological drug. Patients registered more than 6 months after the start of biological therapy were excluded. All patients were registered before 30 June 2008.
Comparison cohort
The cohort of biologic-naïve patients with active RA was recruited in parallel (see authorship list of the BSR Control Centre Consortium) and followed using identical methodology.19 These patients have a physician diagnosis of RA with active disease (guideline DAS28 ≥4.2) despite current treatment with a traditional DMARD and are naïve to biological agents. Comparison patients also had to be registered before 30 June 2008.
Baseline assessment
Baseline information for both cohorts included demographic characteristics, disease duration, 28 swollen and 28 tender joint counts, erythrocyte sedimentation rate and/or C-reactive protein and patient global assessment which enables calculation of a DAS28 score.23 Rheumatoid factor (RhF) positivity was defined as the presence (ever) of a titre ≥1/40. The presence of baseline RA-ILD was based on the response to the following question in the consultant baseline questionnaire: ‘Has the patient ever had any of the following systemic features (of RA): pulmonary fibrosis?’ Other extra-articular manifestations of rheumatoid arthritis (EARA) were defined as the presence (ever) of one or more of sicca syndrome, serosal involvement (pleuritis/pericarditis), eye involvement, systemic vasculitis or nailfold vasculitis. Details of all previous DMARD therapy and all current medications were obtained, as well as smoking history and comorbidity. Patients completed a Health Assessment Questionnaire (HAQ) adapted for British use.24
Follow-up
Data on changes in therapy, disease activity and the occurrence of adverse events were captured in three ways: 6-monthly rheumatologist questionnaire, 6-monthly patient diary and by ‘flagging’ with the UK Office for National Statistics (ONS) who provided information on mortality including cause of death coded according to the International Classification of Diseases 10 (ICD-10).
After 3 years of follow-up, consultant questionnaires were sent annually and patient diaries were no longer sent. Deaths occurring before 30 June 2008, notified from any source, were included in the all-cause mortality analyses. Data were collected until December 2008 to allow for a delay between the date of death and the notification of death being received by the BSRBR from the ONS. Analysis by cause of death was limited to those deaths where notification had been received from the ONS.
RA-ILD was identified from the death certificate using the ICD-10 codes J84.1 ‘Interstitial pulmonary diseases with fibrosis’, J84.9 ‘Interstitial pulmonary disease, unspecified’ and M05.1 ‘Rheumatoid lung’. RA-ILD deaths were categorised into recording of RA-ILD anywhere on the death certificate and RA-ILD as the underlying cause of death (a subset of the former).
Statistical analysis
Patients contributed person years (pyrs) of follow-up from their registration date (anti-TNF start date for the anti-TNF cohort) until the cut-off date (30 June 2008) or the date of death, whichever came sooner. Patients continued to contribute pyrs for the duration of follow-up, irrespective of drug discontinuation, switching between anti-TNF therapies (for the anti-TNF cohort) or the return of consultant questionnaires. Patients could switch from the DMARD cohort to the anti-TNF cohort. Such patients contributed pyrs of follow-up to the DMARD cohort up to the date an anti-TNF drug was started and subsequent follow-up to the anti-TNF cohort. Patients could not switch from the anti-TNF to the DMARD cohort.
Mortalities are presented as the number of deaths/1000 pyrs with 95% CI. Mortality rate ratios (MRRs) were calculated using Cox regression, comparing the anti-TNF cohort with the DMARD cohort. Adjustment was made for age, gender and calendar year of recruitment. Multivariable regression was performed with additional confounders identified from an a priori list of possible confounders including smoking (current/former/never), diabetes, chronic obstructive pulmonary disease (COPD)/asthma, prior tuberculosis, disease severity (HAQ, DAS28 and disease duration as continuous variables), EARA, RhF positivity, number of prior DMARDs, baseline methotrexate use (yes/no) and baseline steroid use (yes/no). Analysis exploring potential confounders was done both by limiting analysis to patients with complete data and by imputing missing data to include all patients. True confounders were identified by sequentially including each confounder in the regression model, and including in the multiple variable regression those confounders that individually changed the estimation after adjustment by more than 10%.25 All analyses were performed using Stata 9.2 (StataCorp, College Station, Texas, USA).
Results
A total of 13 883 patients were included in the analyses, 3464 in the DMARD cohort and 10 649 patients had ever received an anti-TNF drug; 210 patients switched from the DMARD cohort to the anti-TNF cohort and contributed pyrs to both cohorts. In all, 2725 patients in the anti-TNF cohort were known to have been exposed to more than one anti-TNF drug during follow-up. The anti-TNF treated cohort had more severe disease than the DMARD cohort (table 1).
Baseline characteristics
Sixty-eight patients in the DMARD cohort and 299 patients in the anti-TNF cohort had physician-reported RA-ILD at baseline. The RA-ILD cohorts were older and comprised proportionally more men than patients without RA-ILD (table 1). They also had slightly higher disease activity and longer disease duration. Patients with RA-ILD at baseline had more other EARA than patients without RA-ILD, as well as more COPD/asthma. Higher proportions of patients with RA-ILD had ever smoked. Fewer patients with RA-ILD were using methotrexate at baseline. All subsequent analyses are limited to patients with baseline RA-ILD. Three patients with baseline RA-ILD contributed pyrs to both cohorts.
Considering only patients with RA-ILD, the anti-TNF RA-ILD cohort was younger with more severe disease including more EARA than the DMARD RA-ILD cohort. COPD/asthma was balanced in the two cohorts, as was smoking status. The median pyrs of follow-up per patient was 2.1 years for the DMARD RA-ILD cohort and 3.8 years for the anti-TNF RA-ILD cohort (table 2). Fourteen of 68 (21%) of the DMARD RA-ILD cohort died during this follow-up period compared with 70 of 299 (23%) of the anti-TNF RA-ILD cohort. None of the three patients who contributed pyrs to both the DMARD and the anti-TNF RA-ILD cohorts died.
Mortality in DMARD and anti-TNF cohorts stratified by baseline RA-ILD
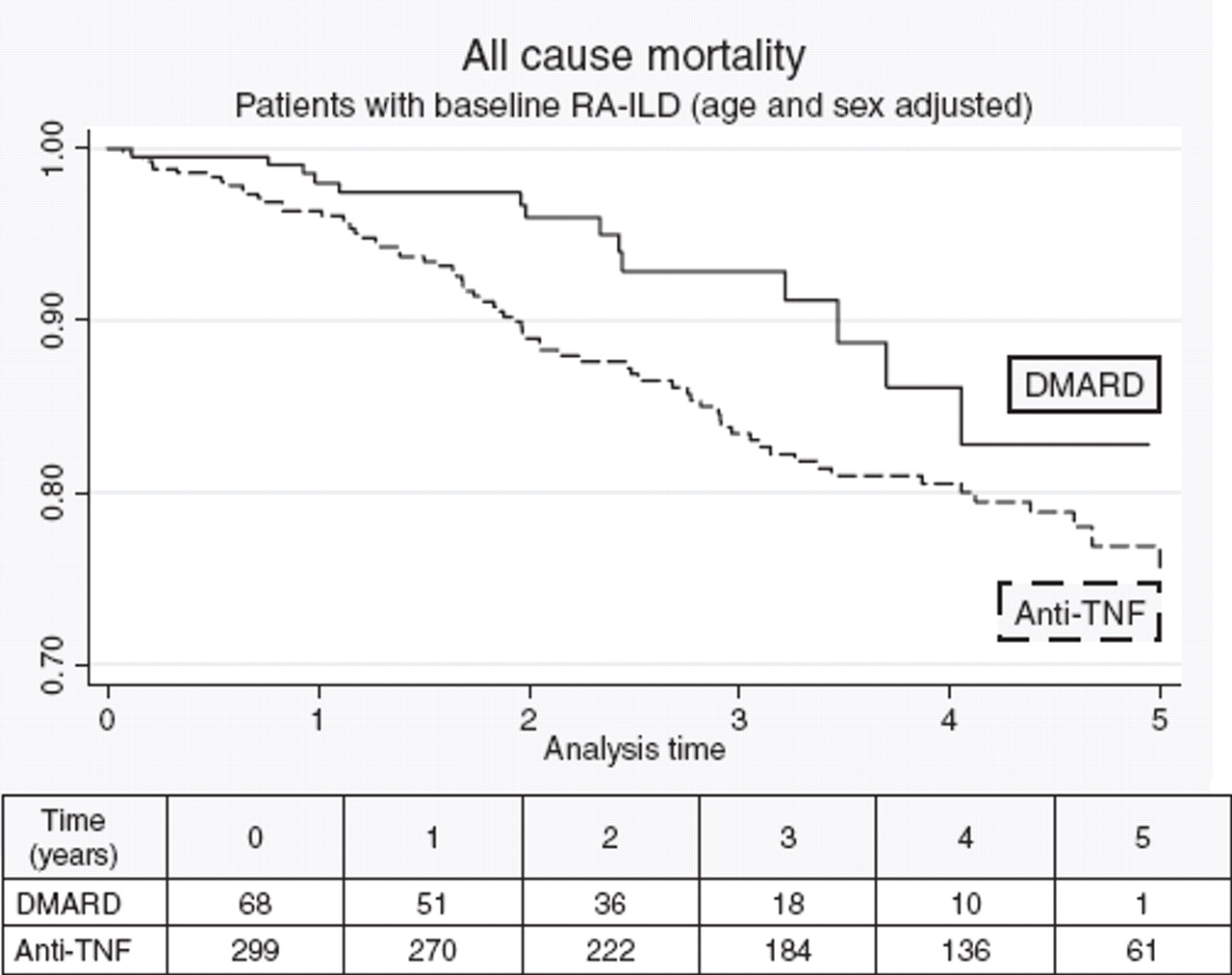
The all-cause mortality was 68 deaths/1000 pyrs (95% CI 53 to 86) in the anti-TNF RA-ILD cohort compared with 92 deaths/1000 pyrs (95% CI 50 to 155) in the DMARD RA-ILD cohort (table 2 and figure 1). After adjustment for age and gender, the adjusted mortality rate ratio (aMRR) was 1.26 (95% CI 0.69 to 2.31) for the anti-TNF RA-ILD cohort compared with the DMARD RA-ILD cohort. However, after full adjustment for potential confounders, the aMRR fell to 0.81 (0.38 to 1.73). Of the potential confounders, age, gender, calendar year of entry, disease duration, HAQ, DAS28 score, COPD/asthma, baseline steroid use and baseline methotrexate use were included in the multivariate model. The only significant predictors of mortality were age (HR 2.28 (95% CI 1.64 to 3.15) per decade) and DAS28 score (HR 1.43 (95% CI 1.11 to 1.85) per unit increase).
{kind=link}
Influence of anti-TNF therapy on all-cause mortality in patients with pre-existing RA-ILD, adjusted for age and gender. Numbers in table represent the number of patients included in follow-up at annual time points. Anti-TNF, anti-tumour necrosis factor; DMARD, disease-modifying antirheumatic drug; RA-ILD, rheumatoid arthritis-associated interstitial lung disease.
RA-ILD was the underlying cause of death in 15/70 patients (21%) who died in the anti-TNF RA-ILD cohort compared with 1/14 (7%) in the DMARD RA-ILD cohort (table 3). The proportion of deaths where RA-ILD was recorded anywhere on the death certificate was also higher in the anti-TNF RA-ILD cohort than in the DMARD RA-ILD cohort (24/70 (34%) vs 2/14 (14%)). The age- and sex-adjusted MRR for deaths where ILD featured on the death certificate was 2.63 (95% CI 0.60 to 11.45) for the anti-TNF RA-ILD cohort compared with the DMARD RA-ILD cohort. We also explored the frequency of RA-ILD-related deaths in patients without baseline RA-ILD. The proportion of deaths for which RA-ILD was the underlying cause was significantly lower in patients who did not have pre-existing RA-ILD (14/635 (2%) deaths in the anti-TNF cohort vs 2/181 deaths (1%) in the DMARD cohort). Similarly, the proportions of deaths where RA-ILD was recorded anywhere on the certificate were much lower in patients without baseline RA-ILD (25/638 deaths (4%) in the anti-TNF cohort vs 4/181 deaths (2%) in the DMARD cohort). When comparing mortalities in patients with RA-ILD compared with no baseline RA-ILD, baseline RA-ILD was a strong predictor of all-cause mortality in both the anti-TNF and DMARD cohorts (age- and sex-adjusted MRR 2.85 (95% CI 2.22 to 3.66) and 2.69 (95% CI 1.55 to 4.67), respectively).
Cause of death in patients with baseline RA-ILD
Discussion
We have shown that the mortality in patients with RA-ILD is not increased following treatment with anti-TNF therapy compared to treatment with traditional DMARDs. However, the proportion of deaths attributable to RA-ILD is higher in patients treated with anti-TNF therapy.
There are a number of methodological issues to consider when interpreting these data. The first important issue is what the reporting of baseline RA-ILD constitutes, and whether this may have differed between the treatment arms. Patients with baseline RA-ILD were identified in response to the question on the consultant baseline questionnaire: ‘Has the patient ever had any of the following systemic features (of RA): pulmonary fibrosis?’. Patients may have been misclassified in either direction. It is possible that patients reported to have baseline RA-ILD did not have the disease. Such misclassification was unlikely to have been imbalanced in the two treatment arms or to introduce bias. The opposite misclassification is more likely: where patients with true RA-ILD at baseline were not reported to the register. Most rheumatologists do not systematically screen for ILD and they may have varying thresholds for initiating investigations. Severe ILD is more likely to be diagnosed than mild ILD.
Anti-TNF safety signals in patients with RA-ILD have been published since 2004.26 Consequently, clinicians may have been less inclined to prescribe anti-TNF therapy to patients with severe RA-ILD. As increasing RA-ILD severity is probably associated with increased mortality, such a selection bias would relatively increase the mortality in the DMARD cohort and lead to a reduction in our estimates of MRR. We should therefore conclude from our results that the way in which UK rheumatologists select patients with pre-existing RA-ILD to receive anti-TNF therapy is not leading to an increase in all-cause mortality, rather than concluding that anti-TNF therapy does not increase the mortality in unselected patients with RA-ILD.
Despite the original cohort size of nearly 14 000 patients, there were only 364 patients with baseline RA-ILD, of whom 84 (23%) died. The small population size has implications for the precision of the estimated relative risk of death attributable to anti-TNF therapy, and is particularly sensitive to the number of deaths in the DMARD RA-ILD cohort, given its smaller size. The aMRR of 0.81 (95% CI 0.38 to 1.73) has wide CIs following adjustment for multiple potential confounders. Although the number of deaths was relatively small, the final inclusion of eight confounders did not contravene guidance that there should be more than 10 events per variable in the model.27 The precision of the estimate could be narrowed with a larger population size. However, this result represents the outcome of a national study conducted over 7 years, and we must accept it as the best available estimate of risk with respect to this important clinical question at this stage.
We were able to measure and adjust for many potential confounders. These included smoking, other EARA and RhF positivity, all of which were more common in patients with baseline RA-ILD. While stepwise adjustment led to moderate changes in the aMRR point estimate, fluctuation was always around unity, reinforcing the absence of an increased risk. As with most observational studies, there may be remaining unmeasured or residual confounding. As mentioned above, RA-ILD severity may have been higher in the DMARD cohort. Unfortunately, despite our efforts to do so, it was not possible to collect robust high-quality data retrospectively about baseline RA-ILD severity.
The proportion of deaths where RA-ILD was recorded on the death certificate was higher in the anti-TNF-treated RA-ILD cohort. The proposed selection bias favouring less severe RA-ILD in the anti-TNF cohort would not explain this finding. Alternative explanations include anti-TNF therapy truly increasing the proportion of deaths attributable to RA-ILD, or clinicians being more inclined to report RA-ILD on the death certificates of patients treated with anti-TNF therapy. Given the existing safety concerns, this latter possibility is plausible.
Less than 3% of patients in this study were reported to have baseline RA-ILD, despite the BSRBR population including only patients with severe active RA. Although estimates of the prevalence of RA-ILD in the literature vary according to the definition of RA-ILD, the cohort under study and the investigation technique, values range from 1% to 80%.1 28,–,30 Our low prevalence of 2.6% would support the suggestion that physicians are identifying only a proportion of the patients who have RA-ILD. As a benchmark of RA-ILD mortality, a UK inception cohort of patients with RA treated in the prebiological era reported 4% of deaths due to RA-ILD,7 which is comparable to the 3% of deaths attributable to RA-ILD in the BSRBR DMARD cohort. Our finding of a nearly threefold higher mortality in patients with RA-ILD than in patients with no RA-ILD replicates recent results from the Mayo Clinic.31
An observational study by Wolfe et al has previously attempted to investigate the association between anti-TNF therapy and the risk of hospitalisation for RA-ILD.32 Although they reported a univariate association between prior anti-TNF use and hospitalisation for RA-ILD, the authors acknowledge this probably represents confounding by indication, concluding that they were unable to make any inference about causality.
Despite initial concerns about the safety of anti-TNF therapy in patients with RA-ILD, our study has not found an increased rate of mortality. This is reassuring, and suggests that UK clinicians are currently making appropriate decisions about which patients with RA-ILD to treat with anti-TNF. However, it should not be assumed that it is safe to prescribe anti-TNF therapy to unselected patients with RA-ILD. Our analysis does not enable us to advise on whether patients should be screened prior to treatment, how patients should be selected for treatment, or how patients should be monitored once treatment is commenced.
Acknowledgments
The authors acknowledge the enthusiastic collaboration of all consultant rheumatologists and their specialist nurses in the UK in providing the data. In addition, we acknowledge the support from Dr Ian Griffiths (Past) and Professor David Isenberg (Current), Chairs of the BSRBR Management Committee, Professor Gabriel Panayi, Professor David GI Scott, Dr Andrew Bamji and Dr Deborah Bax, Presidents of the BSR during the period of data collection, for their active role in enabling the Register to undertake its tasks and to Samantha Peters (CEO of the BSR), Mervyn Hogg, Nia Taylor and members of the BSRBR Scientific Steering Committee. We also acknowledge the seminal role of the BSR Clinical Affairs Committee for establishing national biologic guidelines and recommendations for such a Register. Finally we would like to acknowledge the substantial contribution of Andy Tracey, Katie McGrother and ML in database design and manipulation and Professor Alan Silman in his prior role as a principal investigator of the BSRBR.
References
Footnotes
-
BSRBR Control Centre Consortium Antrim Area Hospital, Antrim (Dr Nicola Maiden); Cannock Chase Hospital, Cannock Chase (Dr Tom Price); Christchurch Hospital, Christchurch (Dr Neil Hopkinson); Derbyshire Royal Infirmary, Derby (Dr Sheila O'Reilly); Dewsbury and District Hospital, Dewsbury (Dr Lesley Hordon); Freeman Hospital, Newcastle-upon-Tyne (Dr Ian Griffiths); Gartnavel General Hospital, Glasgow (Dr Duncan Porter); Glasgow Royal Infirmary, Glasgow (Professor Hilary Capell); Haywood Hospital, Stoke-on-Trent (Dr Andy Hassell); Hope Hospital, Salford (Dr Romela Benitha); King's College Hospital, London (Dr Ernest Choy); Kings Mill Centre, Sutton-In Ashfield (Dr David Walsh); Leeds General Infirmary, Leeds (Professor Paul Emery); Macclesfield District General Hospital, Macclesfield (Dr Susan Knight); Manchester Royal Infirmary, Manchester (Dr Ian Bruce); Musgrave Park Hospital, Belfast (Dr Allister Taggart); Norfolk and Norwich University Hospital, Norwich (Professor David Scott); Poole General Hospital, Poole (Professor Paul Thompson); Queen Alexandra Hospital, Portsmouth (Dr Fiona McCrae); Royal Glamorgan Hospital, Glamorgan (Dr Rhian Goodfellow); Russells Hall Hospital, Dudley (Professor George Kitas); Selly Oak Hospital, Selly Oak (Dr Ronald Jubb); St Helens Hospital, St Helens (Dr Rikki Abernethy); Weston General Hospital, Weston-super-Mare (Dr Shane Clarke); Withington Hospital, Manchester (Dr Paul Sanders); Withybush General Hospital, Haverfordwest (Dr Amanda Coulson).
-
Competing interests None.
-
Ethics approval Ethical approval for this study was obtained in December 2000 from the Multicentre Research Ethics Committee (MREC) for the Northwest of England.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Miscellaneous