Article Text

Abstract
Objectives: Patients with rheumatoid arthritis (RA) have increased cardiovascular mortality. Tumour necrosis factor α (TNFα)-blocking therapy has been shown to reduce RA disease activity measures and joint damage progression. Some observational studies suggest that TNFα blockade reduces mortality and incidence of first cardiovascular events. The mechanisms contributing to these outcomes are unclear. This study assessed the effects of infliximab treatment on vascular stiffness and structure in patients with RA.
Methods: A post hoc analysis of longitudinal data from a randomised placebo controlled study evaluated the effect of infliximab on vascular assessments. 26 patients received intravenous infliximab (3 mg/kg) at weeks 0, 2, 6 and every 8 weeks thereafter to week 54. Patients were followed up to 56 weeks of infliximab therapy with assessments of RA disease activity, cardiovascular risk factors, vascular stiffness (pulse wave velocity (PWV)), carotid intima media thickness (CIMT) and carotid artery plaque (CAP). Univariate analyses of changes over time by repeated measures analysis of variance (ANOVA) were followed by multivariate time-series regression analysis (TSRA) if changes were seen.
Results: PWV was significantly lower (better) after 56 weeks of treatment with infliximab (ANOVA p<0.01, TSRA p<0.01). However, CIMT (ANOVA p = 0.50) and CAP (χ2 = 4.13, p = 0.88) did not change over the study period. Multiple cardiovascular risk measures did not change with treatment and did not correlate with changes in measures of vascular structure.
Conclusions: Arterial stiffness improves with infliximab treatment in RA. This change may help explain the improved cardiovascular disease survival in patients with RA receiving TNFα-blocking therapy.
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is associated with increased cardiovascular morbidity and mortality.1 Patients with RA have a higher risk of cardiovascular events2 3 not explained entirely by traditional cardiovascular risk factors,4 implying that cardiovascular disease is an extra-articular manifestation of RA.5
Tumour necrosis factor α (TNFα) is a pro-inflammatory cytokine central to the pathology of RA and may also promote vascular disease.6 7 TNFα-blocking drugs reduce inflammation and joint damage in RA,8–11 and may reduce mortality12 and cardiovascular disease.13 14 Data indicate that patients responding to TNFα-blocking therapy within the first 6 months have a greater reduction in the incidence of myocardial infarction compared with non-responders.15 Surrogate vascular measures have been used to indicate early atherosclerosis and predict increased future cardiovascular risk. Increased arterial stiffness, increased carotid intima media thickness (CIMT) and endothelial dysfunction have been demonstrated in patients at increased risk of and with known cardiovascular disease.16 17 They have also been found to be independent predictors of future cardiovascular events.18 19 Carotid-femoral pulse wave velocity (PWV) is now used as a therapeutic end point in studies of antihypertensive treatments.20 All of these measures have been reported to be abnormal in patients with RA.21–23 Improvement in arterial stiffness has been reported in RA after TNFα-blocking therapy with etanercept.24 Previous reports of CIMT in response to TNFα blockade indicate mixed results.21 25
There is conflicting evidence regarding the roles of conventional cardiovascular risk factors in the pathogenesis of atherosclerosis in RA. Oxidised low-density lipoprotein (LDL) is thought to be particularly atherosclerogenic.26 Adiponectin is an adipokine associated with the metabolic syndrome and possibly with accelerated atherosclerosis.27 The relationship of these two factors with atherosclerosis in the setting of RA has not been evaluated.
This longitudinal study examined the effects of infliximab on vascular stiffness and structure in patients with RA and measured changes in multiple risk factors for atherosclerotic disease including oxidised LDL and adiponectin. We evaluated this initially as a randomised controlled trial and then undertook a post hoc re-evaluation when the entire cohort received infliximab.
METHODS
Patients
Adult subjects (⩾18 years) with RA defined by American College of Rheumatology criteria28 referred for TNFα-blocking therapy according to the British Society of Rheumatology (BSR) criteria were recruited from outpatient clinics at Guy’s and St Thomas’ Hospitals between January 2004 and June 2005. Patients were invited to participate if they had failed on two disease-modifying antirheumatic drugs including methotrexate, and had a disease activity score 28 (DAS28) >5.1 on two occasions at least 4 weeks apart. All patients were taking methotrexate (⩽25 mg/week). All antirheumatic medications remained stable for at least 4 weeks preceding and during the study unless changes in dose were medically indicated.
Exclusion criteria were chosen in an effort to exclude patients with traditional cardiovascular risk factors or drug treatments that may confound results. Patients were therefore excluded from the study if they had a history of ischaemic heart disease, cerebrovascular disease, peripheral vascular disease, diabetes mellitus, treatment with aspirin or prednisolone at a dose >10 mg/day and previous treatment with infliximab or any therapeutic agent targeted at TNFα. Patients with evidence of current or previous infection with tuberculosis, regardless of previous treatment, were excluded.
Protocol
In a randomised, placebo controlled, double-blind study, patients were allocated using a 2:1 randomisation procedure to infliximab or placebo. Infliximab 3 mg/kg was administered by intravenous infusion at weeks 0, 2, 6 and every 8 weeks thereafter for a total of 54 weeks. Patients randomised to placebo received saline infusions for the first 22 weeks and switched to open-label infliximab at week 24. Patients in the placebo group with worsening RA disease activity at week 14 were permitted to escape to open-label infliximab at week 16. The primary outcome measures were vascular ultrasound assessments at weeks 24 and 56 (2 weeks after infusions to assess maximal improvement). Secondary outcome measures included RA disease activity and cardiovascular risk factors.
Assessment of RA disease activity
RA disease activity was assessed at baseline, 8, 16, 24, 40 and 56 weeks by the modified Health Assessment Questionnaire (HAQ),29 28 swollen and tender joint counts, erythrocyte sedimentation rate (ESR), patient global assessment using a 100 mm visual analogue scale and DAS28.30
Assessment of cardiovascular risk factors
Cardiovascular risk factors included systolic and diastolic blood pressure (BP), C-reactive protein (CRP), serum fasting lipid profile (total cholesterol, high- and low-density lipoprotein fractions (HDL, LDL) and triglycerides), oxidised LDL, insulin resistance measured by log homeostasis model assessment (HOMA)31 and adiponectin.27 Subjects who had smoked within the last 2 years were categorised as current smokers. BP, heart rate and HsCRP were assessed at baseline, 8, 16, 24, 40 and 56 weeks. Lipid profiles and HOMA were measured at 0, 24, 40 and 56 weeks and adiponectin at 0, 24, 40 and 56 weeks.
Vascular assessments
BP and assessment of vascular stiffness (PWV), structure (CIMT), augmentation index (AI) and carotid artery (atherosclerotic) plaque (CAP) were measured in supine fasting subjects in a quiet room with temperature controlled to 22°C. Antihypertensive, anti-inflammatory and cyclo-oxygenase-2 inhibitor medications were withheld 24 h before assessment. BP was measured using an Omron BP monitor. The mean of three measurements was recorded for each vascular assessment. The ultrasonographer was blind to the treatment status of the patients during the randomised controlled phase of the study.
Arterial stiffness: pulse wave velocity (PWV)
Carotid-femoral PWV was measured at baseline and after 24 and 56 weeks of treatment as the time delay between the rapid upstroke of the carotid and femoral artery pulse waves using the PWA system (SphygmoCor, PWA Medical, Sydney, Australia). The distance between the two arterial points was measured on the surface of the body using a tape measure. PWV was calculated as the distance travelled by the arterial pulse wave in metres divided by the time delay between the two arterial points in seconds (intra-observer reliability ICC = 0.84, N = 12 subjects with RA).
Arterial structure: carotid intima media thickness (CIMT)
CIMT was measured at weeks 0 and 56 using ECG-triggered high-resolution duplex ultrasonography (Acuson XP10) with a 7.5 MHz vascular probe. Measurements were performed on the common carotid arteries 1–2 cm proximal to the bulb and studied in longitudinal and transverse planes with anterior, lateral and posterior approaches. The average of the measurements of the anterior, lateral and posterior projections of the far wall performed on each side was used to calculate the CIMT for each subject (intra-observer reliability ICC = 0.98, N = 12 subjects with RA).
Augmentation index (AI)
AI is a method of pulse wave analysis (PWA) performed using applanation tonometry of the radial artery (PWA system, SphygmoCor); it was measured at weeks 0, 24 and 56. The PWA system acquires 10–12 sequential waveforms and generates an averaged radial and mathematically-derived corresponding central aortic waveform. AI is derived from the estimated aortic waveform and is defined as the increase in pressure from the first systolic peak/shoulder to the second systolic peak/shoulder expressed as a percentage of pulse pressure (intra-observer reliability ICC = 0.86, N = 8 subjects with RA).
Carotid artery plaque (CAP)
CAP was measured by ultrasound at weeks 0, 24 and 56. A grade of 0 was assigned for no plaque, 1 for minimal plaque and 2 for extensive plaque. A combined score for the right and left carotid arteries was calculated as the sum of the right and the left scores for each individual subject on a scale of 0–4.
Statistical analysis
Sample size calculation
The sample size was estimated for a 2:1 (infliximab: placebo) randomised controlled trial using unpublished paired assessments of PWV in 12 patients with RA (mean 8.88, σ 2.12 m/s (first assessment) and reliability ICC 0.84. Smallest detectable difference (Δ) was calculated as 3.23,32 giving a required sample size of six patients per group (α = 0.05, power = 0.80). Assuming a 30% drop-out rate, we aimed to recruit 9 patients for placebo and 18 for treatment.
Intention-to-treat analysis
Assessments of RA disease activity, BP and heart rate were compared between subjects in the treatment and placebo arms by a two-sided Student t test at 0, 8 and 16 weeks. Follow-up vascular assessments were not performed within the 16-week placebo controlled phase and, as such, could not be included in the analysis.
Post hoc analyses
Post hoc multivariate ANOVA modelling was performed to evaluate the effects of treatment with infliximab (vs placebo) and duration of treatment (0 vs 8 vs 16 weeks) on disease activity, systolic and diastolic blood pressure and heart rate during the initial controlled part of the trial.
Because all subjects in the placebo arm elected to “escape” to the treatment arm at 16 weeks, a second post hoc analysis was performed to evaluate trends in all subjects over time during treatment with infliximab. For patients in the placebo arm, the baseline infliximab assessment was at the end of the placebo controlled phase at 16 weeks, the 8-week assessment was at week 24, the week 24 assessment was at week 40, and the week 40 assessment was at week 56. Preliminary univariate analysis was performed to identify possible changes during infliximab. For continuous data the changes over time from pretreatment to 24 and 56 weeks were evaluated by repeated measures analysis of variance (RM ANOVA) with time point comparisons using Bonferroni-corrected t tests. Assessments of CAP, being categorical data, were evaluated by the χ2 test. Vascular assessments that changed during infliximab therapy were further explored for possible confounding influences by simple correlation followed by time-series regression analysis with linear random intercepts models accounting for clustering within individuals. In this analysis we used all available observations preceding and during infliximab treatment. Potentially modifiable cardiovascular risk factors that correlated with the vascular assessment at baseline with r>0.20 were evaluated.
The study database was generated by the Trial Coordination Center (TCC), Groningen, The Netherlands. All entries were double-entered to ensure complete and accurate data capture, and all data queries answered before the database was cleaned and locked. Statistical analysis was performed using Stata Version 6.0 (Statacorp, Texas, USA).
RESULTS
Twenty-six subjects were enrolled in the study; 17 were randomised to infliximab and 9 to placebo. All 9 subjects in the placebo arm elected to take the escape arm after 14 weeks. A greater proportion of patients in the treatment arm were rheumatoid factor positive, otherwise baseline characteristics were similar across the groups (table 1).
Intention-to-treat analysis
The results for the placebo controlled double-blind phase of the study are shown in fig 1. Tender and swollen joint counts, patient global assessments and DAS28 scores were all significantly lower in the treatment arm by 8 and 16 weeks. ESR was significantly better in the treatment arm at 8 weeks but not at 16 weeks. Heart rate, CRP, systolic and diastolic BP were not significantly different at 8 or 16 weeks. Arterial stiffness, lipid profiles, HOMA and adiponectin were not assessed during the placebo controlled phase of the study.
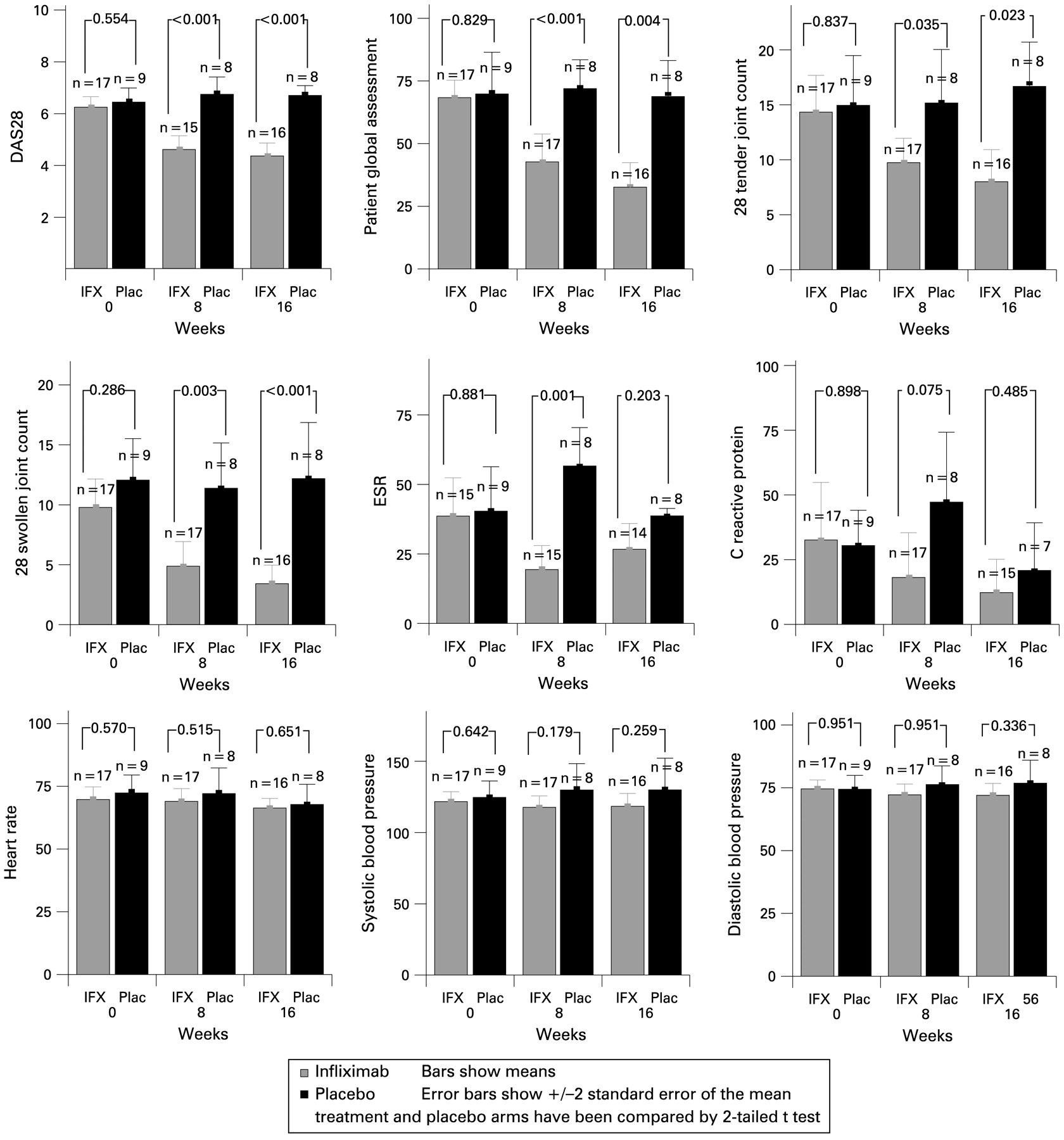
Comparison of disease activity (DAS), heart rate, systolic and diastolic blood pressure in infliximab (IFX) and placebo (Plac) groups during the placebo controlled phase of the trial. ESR, erythrocyte sedimentation rate.
Post hoc analysis
Post hoc multivariate ANOVA modelling of the initial controlled phase of the trial confirmed the effect of treatment on disease activity (DAS28, ESR, tender and swollen joint counts) but not heart rate, systolic and diastolic BP. In the second post hoc analysis, evaluating trends in all patients as they received infliximab, RM ANOVA showed a significant reduction in arterial stiffness (PWV, p = 0.004) over 56 weeks (fig 2). However, CIMT (p = 0.499), AI (p = 0.265) and CAP (χ2 = 4.13, p = 0.88; data not shown) did not change. RA disease activity (DAS28, tender and swollen joint counts, patient global scores and ESR) improved significantly (p<0.05, fig 2). There were no significant changes in systolic BP (p = 0.506) or diastolic BP (p = 0.835), triglycerides (p = 0.830) or adiponectin levels (p = 0.962), although HOMA (p = 0.540) showed a non-significant decrease and serum HDL (p = 0.336) showed non-significant increases (fig 3).
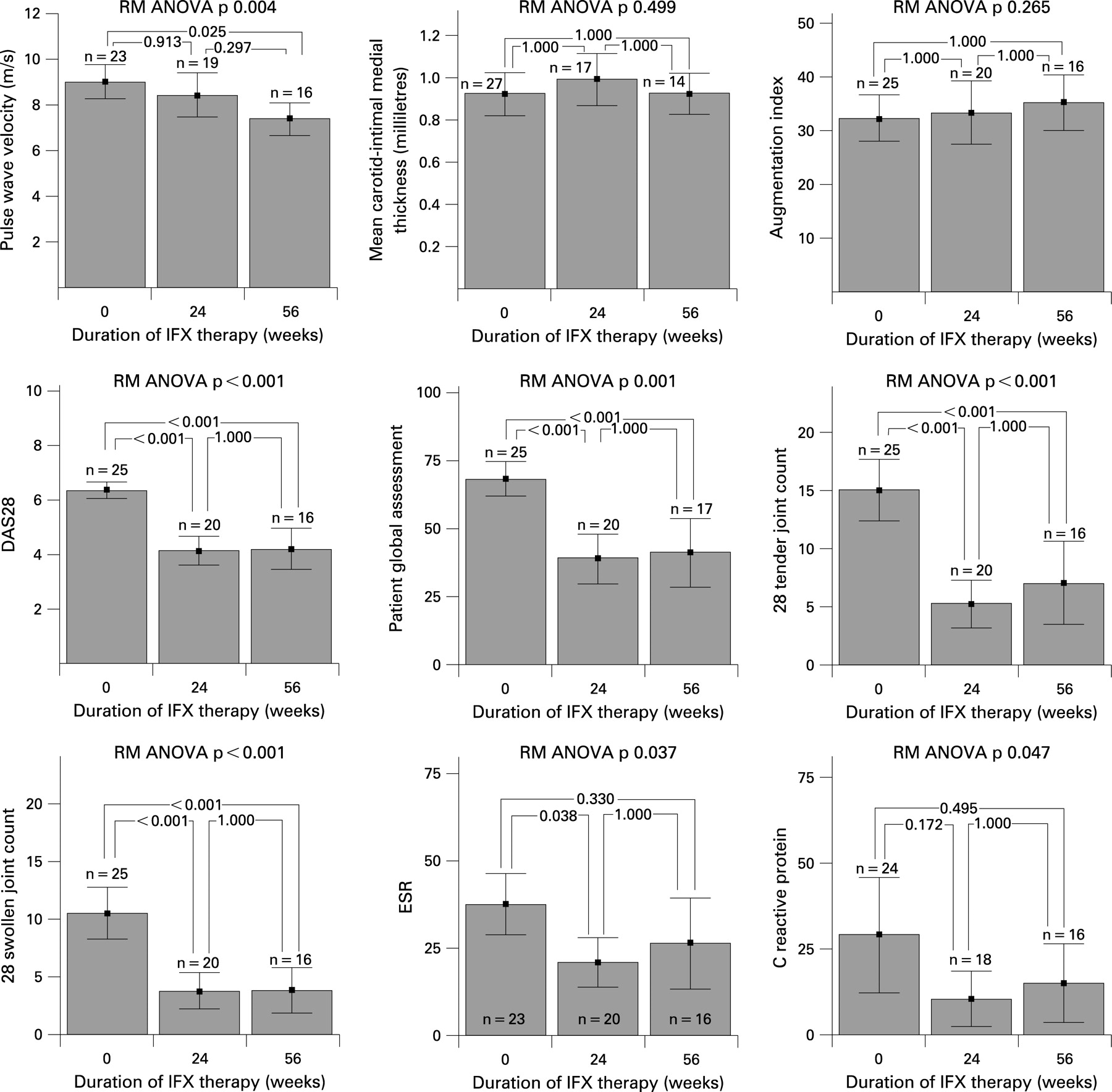
Post hoc analysis: trends in vascular measurements and rheumatoid arthritis disease activity (DAS) during treatment with infliximab (IFX). Repeated measures (RM) ANOVA p values indicate the significance of the overall trend while comparison between paired time points are compared by t tests adjusted for multiple comparisons (Bonferroni correction). ESR, erythrocyte sedimentation rate.

{kind=link}
{kind=link}
{kind=link}
Post hoc analysis: trends in cardiovascular risk factors during treatment with infliximab (IFX). Repeated measures (RM) ANOVA p values indicate the significance of the overall trend while comparisons between paired time points are made by t test adjusted for multiple comparisons (Bonferroni correction). BP, blood pressure; HDL, high-density lipoprotein; HOMA, insulin resistance measured by log homeostasis model assessment; LDL, low-density lipoprotein.
Influences on PWV were explored further by univariate Pearson correlation (data not shown). PWV correlated most strongly with age at enrolment (r = 0.64, N = 26, p<0.01) and, to a lesser extent, with heart rate (r = 0.39, N = 70, p<0.01), systolic BP (r = 0.45, N = 70, p<0.01), serum HDL (r = −0.35, N = 70, p<0.01), serum triglycerides (r = 0.25, N = 63, p<0.05) and total serum cholesterol (r = −0.17, N = 63, p = 0.19). PWV also correlated negatively with duration of infliximab treatment (r = −0.34, N = 70, p<0.01) and positively with patient global assessment (r = 0.26, N = 70, p = 0.03) and DAS28 (r = 0.23, N = 70, p = 0.06). Multivariate time-series regression modelling found that duration of infliximab treatment (negative correlation) and heart rate (positive correlation) were the only significant influences on PWV (table 2).
DISCUSSION
This study evaluated the effect of TNFα-blocking therapy on vascular structure in RA. The placebo controlled part of the study was unable to assess vascular effects of infliximab due to early drop-out of the placebo group. The post hoc analysis of long-term treatment showed that arterial stiffness (PWV) improved after treatment with infliximab for 56 weeks. CIMT, AI and CAP did not change over the course of the study. Although we showed significant improvements in vascular stiffness, the mechanisms of this improvement remain unclear. We measured multiple modifiable cardiovascular risk factors but these did not change significantly during infliximab treatment. This may reflect a type II error owing to the small study size. However, the fact that significant changes were seen in PWV and not in any other cardiovascular risk factor suggests that changes in PWV cannot be explained entirely by changes in conventional risk factors.
This is the first study to demonstrate long-term improvement in RA vascular stiffness with TNFα-blocking therapy. One small study showed improvement in PWV with etanercept24 while others found no change in AI after TNFα-blocking therapy,24 33 supporting our own work. AI measures vascular stiffness and peripheral resistance,34 while PWV purely reflects vascular stiffness20 and probably reflects the severity of atherosclerosis and vessel wall calcification. PWV is increased in hypertension,20 hypercholesterolaemia,35 vasculitis36 and RA,24 and strongly predicts cardiovascular events in hypertension19 and cardiovascular and all-cause mortality in diabetes37 and hypertension.38
The long-term improvements in vascular stiffness shown in our study support the registry studies demonstrating improvements in vascular disease in patients receiving TNFα-blocking drugs.12–14 Cohort studies show reductions of cardiovascular events in patients treated with TNFα-blocking therapy.13 The CORRONA Registry found a reduction of cardiovascular events in patients receiving TNFα-blocking therapy14 that was not evident before 6 months of treatment, with greatest benefit after 12 months of treatment. This time course is consistent with our findings using PWV.
Not all studies support the above findings. The British Society for Rheumatology Biologics Register (BSRBR) demonstrated an improvement in the incidence of myocardial infarction in patients with RA responding to TNFα-blocking therapy within the first 6 months compared with patients receiving traditional disease-modifying antirheumatic drugs.15 Two large nested case-control studies have not found a significant improvement in the rates of myocardial infarction39 40 or stroke39 in patients treated with TNFα-blocking therapy compared with patients not receiving this therapy. However, these observational studies may be falsely negative due to confounding by indication.
Data regarding the effect of anti-TNF therapy on CIMT is conflicting. CIMT has been shown to be increased in some studies of patients with RA compared with age-matched control subjects.41–43 CIMT improves slowly with lipid-lowering therapy. Del Porto et al found significant improvements in CIMT after 12 months of TNFα-blocking therapy,21 but Gonzalez-Juanatey showed worsening of CIMT during 2–3 years of TNFα-blocking therapy.25 Our study may have been underpowered to demonstrate improvements in CIMT, but it is equally possible that anti-TNF therapy prevented increases in CIMT that would have occurred without treatment. We also did not evaluate plaque characteristics (softness, hardness) which may have changed more rapidly.
Methotrexate has been shown to improve mortality in RA.44 All patients in the present study were taking stable background methotrexate, so any benefit on cardiovascular function seen in this study will be due to infliximab. However, we were unable to demonstrate synergy of methotrexate and infliximab in relation to vascular structure as has been shown for joint disease activity.8–11
The major limitation of our study mainly is the study size. Also, the lack of vascular outcome measures before 24 weeks means that we may have missed any earlier changes to vascular structure and stiffness, particularly if changes did in fact occur earlier but then reverted back to baseline within the time-frame of assessment. This study has, however, shown for the first time that BP measures are stable over a 16-week period and do not exhibit a placebo response. This finding is particularly important since PWV is affected by BP. As BP remains constant, the changes demonstrated for PWV more likely reflect true changes in aortic stiffness.
We examined many potential mechanisms for the long-term improvements in vascular stiffness, including novel modifiable cardiovascular risk factors such as HOMA and adiponectin. Adiponectin is lower in patients at increased risk of cardiovascular disease.27 Most of the modifiable cardiovascular risk factors we measured did not correlate with vascular measures at baseline. More importantly, we found no significant changes in these measures over time despite significant improvements in disease activity and vascular stiffness, suggesting that this might have occurred at least partly independent of conventional cardiovascular risk factors. The evidence for a role for conventional risk factors in anti-TNFα-mediated cardiovascular protection is conflicting, with some work supporting45 and other work not supporting46 a role for these factors. It has also been suggested that a reduction in oxidative stress changes the function of lipid particles,47 but we found no changes in oxidised LDL levels or the ratio of oxidised LDLto LDL. We are therefore left with the enigma that vascular abnormalities are somehow linked to chronic active RA, but the mechanisms of this link are unclear.
In conclusion, we report that arterial stiffness improves with long-term infliximab treatment in RA and that this seems to occur independently of conventional cardiovascular risk factors. These findings suggest that the combination of TNFα-blocking therapy with methotrexate not only reduces joint damage but also vascular “damage” in patients with RA. This is consistent with recent findings of reduced mortality and cardiovascular events after several months in patients with RA receiving TNFα-blocking therapy.
Acknowledgments
The authors thank Karen McNeill and Janine Kelleher for their help in study coordination and data collection.
REFERENCES
Footnotes
Competing interests: BK conducts clinical trials and sits on speaker panels for Abbott, Centocor, Schering-Plough, Bristol-Meyers-Squibb and Amgen. SPO conducts trials for Amgen, Abbott, Centocor and Bristol-Myers-Squibb.
Funding: This study was supported by a grant from Centocor Pty Ltd. MW was supported by the Arthritis Foundation of Australia.
Ethics approval: The study was approved by the Guy’s Hospital Research Ethics Committee and patients gave written informed consent.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.