Article Text

Statistics from Altmetric.com
The type I interferons (IFNs), IFNβ and various IFNαs, are pleiotropic cytokines acting on a range of cell types and eliciting a diverse range of responses. For many years IFNβ was thought to be a potential agent for the treatment of a variety of immune-mediated diseases. Clinical trials showing a beneficial effect of IFNβ treatment on clinical and MRI measures in relapsing–remitting multiple sclerosis were published almost a decade ago.1 2 These publications have stimulated studies on its potential for the treatment of patients with rheumatoid arthritis (RA). IFNβ has clear anti-inflammatory properties3 and plays an important role in bone homeostasis.4 Of special interest is the ability of IFNβ to reduce the secretion of proinflammatory mediators such as interleukin (IL)6, tumour necrosis factor (TNF)α, matrix metalloproteinases (MMPs) and prostaglandin E2, which are key players in the pathogenesis of RA.5 6 In addition, IFNβ has antiangiogenic properties,7 which could boost therapeutic effect in RA.8
The notion that IFNβ treatment may reduce arthritis is supported by animal experiments. Several studies examining the effect of IFNβ in collagen-induced arthritis (CIA) in mice have been published. In one study mice were given daily intraperitoneal injections with mouse IFNβ9 and in another study, mice were injected intraperitoneally with a single injection of fibroblasts expressing IFNβ, resulting in continuous IFNβ production.10 Both studies revealed a beneficial effect on arthritis activity and histological scores for inflammation. A similar effect was shown in CIA in rhesus monkeys that were treated daily for 7 days with recombinant human IFNβ.11 More recently, it has been shown that IFNβ-deficient mice had prolonged CIA with a higher incidence of arthritis compared to control mice,12 supporting the evidence that IFNβ has an anti-inflammatory effect.
Based on the favourable effects of daily treatment with relatively high dosages of IFNβ in animal models of RA, we previously performed an open label phase I study in 12 patients with active RA who were treated with purified natural fibroblast IFNβ,11 followed by a double-blind, placebo-controlled phase II trial that evaluated the efficacy of mammalian cell-derived recombinant IFNβ1a.13 In the first, open study there were trends towards clinical improvement, although there was no change in key synovial biomarkers.14 In the latter study 209 patients with RA who were on stable methotrexate received 2.2 or 44 μg IFNβ1a, or placebo, subcutaneously three times weekly for a period of 24 weeks.13 It was felt that daily injections with higher dosages, comparable to those used in the animal models, would not be tolerated by the patients. This dosing regimen did not result in clinical improvement or protection against joint destruction,13 perhaps because higher and more constant levels of IFNβ may be required to translate into clinical benefit.3
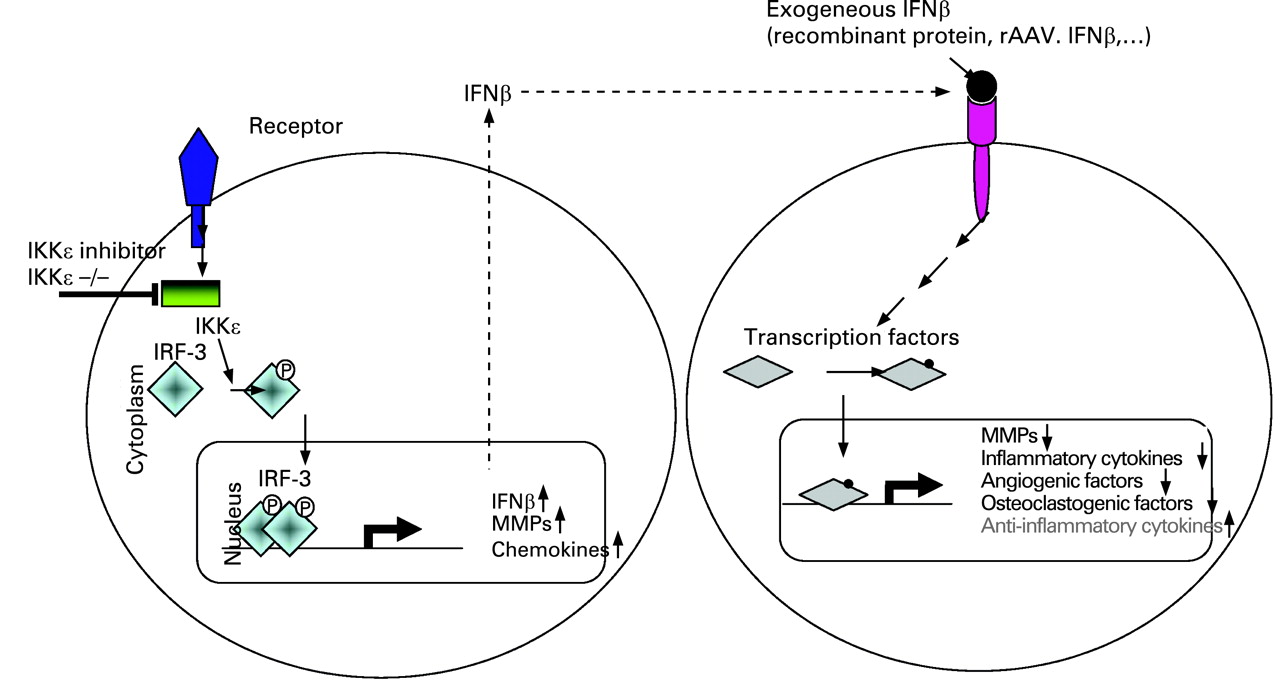
Novel approaches are under investigation using IFNβ as a therapeutic agent. Two different strategies are being evaluated: (1) systemic combination therapy of low dosage IFNβ treatment with inhibition of the IκB kinase (IKK)-related kinase, IKKϵ and (2) intra-articular gene therapy aimed at reaching relatively high levels of IFNβ at the site of inflammation, thus limiting systemic side effects. The interesting study by Corr et al (see page 257) in this issue of the Annals of the Rheumatic Diseases15 examined the role of IKKϵ in the K/BxN serum model of RA and its ability to improve the response to systemic IFNβ therapy. IKKϵ is constitutively expressed in synovial tissue of patients with RA and significantly higher levels of phosphorylated IKKϵ were observed in RA synovium compared to osteoarthritis.16 IKKϵ is an IKK-related kinase with 30% homology to IKK1 and IKK2, and was first described as a lipopolysaccharide (LPS)-inducible kinase.17 Recent work has suggested that the primary role of IKKϵ may be the phosphorylation of interferon regulatory factor 3 (IRF3),18 leading to the induction of type I interferons. In addition, IKKϵ may induce the expression of several MMPs and chemokines, suggesting that IKKϵ might be a good target to suppress synovial inflammation.19 Corr et al showed that either IKKϵ deficiency or low dose IFNβ treatment in wild type mice protects in part against inflammation in the passive serum transfer model of RA. There was a statistically significant decrease in arthritis activity in IFNβ-treated mice and IFNα/β receptor-deficient mice had an accentuated course of arthritis, consistent with the studies evaluating the role of IFNβ in arthritis discussed above. Of interest, the potential benefit of combination therapy was suggested by the observation that low dose IFNβ treatment in IKKϵ-deficient mice resulted in a further reduction of arthritis scores. This combination therapy could enhance efficacy and decrease the suppressive effects of IKKϵ inhibition on host defence. Thus, combination therapy comprising low dose IFNβ treatment and IKKϵ inhibition may perhaps offer a new treatment option for patients with RA. An overview of the proposed mechanisms of action is shown in fig 1.The study by Corr et al does not only present very interesting scientific data on IFN-regulated mechanisms, but it also provides the rationale for more comprehensive preclinical studies on the effects of coadministration of IFNβ with an IKKϵ inhibitor. However, an important question will be if systematic treatment with even low dosages of IFNβ will be tolerated by patients with RA. In our previous clinical trial we observed a trend towards increased injection site reactions (13%), flu-like symptoms (18%) and fever (6%) in the group that received very low IFNβ dosages (2.2 μg three times weekly) compared to matching placebo (3%, 12% and 0%, respectively).12
{kind=link}
In light of the potential side effects of systemic treatment, an alternative might be the development of intra-articular treatment. We have previously hypothesised that continuous therapeutic levels of IFNβ local at the site of inflammation may be required to induce clinical efficacy and to avoid systemic side effects.3 This could be achieved by local gene therapy of the inflamed joint. Recombinant adenoassociated (rAAV) vectors are currently considered as the most optimal vectors for the treatment of immune-mediated inflammatory diseases, including RA, because of their high safety profile together with the capacity to confer long-term expression of therapeutic transgenes in a variety of tissues.20 We have identified rAAV serotype 5 as the most efficient rAAV vector for transducing synovial tissue.21 22 After successful proof of concept studies, using an adenoviral vector (Ad),23 we have investigated the potential of intra-articular IFNβ gene therapy using an rAAV5 vector expressing rat IFNβ in adjuvant-induced arthritis in rats.24 Local delivery of Ad or rAAV5 vectors expressing rat IFNβ in the ankle joint after the onset of disease reduced paw swelling impressively in treated and untreated contralateral joints. Strikingly, IFNβ treatment also protected against bone erosions and cartilage degradation. Together, the results provide a strong rationale for IFNβ gene therapy as a novel therapeutic approach for arthritis. Recently, toxicity and biodistribution studies have been initiated evaluating the effects of an rAAV5 vector expressing human IFNβ. Conceivably, based on the results presented by Corr et al, the effects of this approach might be enhanced by simultaneous inhibition of IKKϵ, although this remains to be shown.
Taken together, recent studies have placed IFNβ back on the list of potential new therapies for RA aimed at targeting synovial inflammation and joint destruction. Low dose IFNβ treatment combined with IKKϵ inhibition as well as intra-articular IFNβ gene therapy appear interesting options worth exploring for future clinical development.
REFERENCES
Footnotes
Competing interests: All authors are affiliated with Arthrogen BV, a company developing adenoassociated virus based gene therapy for rheumatoid arthritis.
Linked Articles
- Basic and translational research