Article Text

Abstract
Objective: To develop evidence-based recommendations for the management of systemic glucocorticoid (GC) therapy in rheumatic diseases.
Methods: The multidisciplinary guideline development group from 11 European countries, Canada and the USA consisted of 15 rheumatologists, 1 internist, 1 rheumatologist–epidemiologist, 1 health professional, 1 patient and 1 research fellow. The Delphi method was used to agree on 10 key propositions related to the safe use of GCs. A systematic literature search of PUBMED, EMBASE, CINAHL, and Cochrane Library was then used to identify the best available research evidence to support each of the 10 propositions. The strength of recommendation was given according to research evidence, clinical expertise and perceived patient preference.
Results: The 10 propositions were generated through three Delphi rounds and included patient education, risk factors, adverse effects, concomitant therapy (ie, non-steroidal anti-inflammatory drugs, gastroprotection and cyclo-oxygenase-2 selective inhibitors, calcium and vitamin D, bisphosphonates) and special safety advice (ie, adrenal insufficiency, pregnancy, growth impairment).
Conclusion: Ten key recommendations for the management of systemic GC-therapy were formulated using a combination of systematically retrieved research evidence and expert consensus. There are areas of importance that have little evidence (ie, dosing and tapering strategies, timing, risk factors and monitoring for adverse effects, perioperative GC-replacement) and need further research; therefore also a research agenda was composed.
Statistics from Altmetric.com
Since 1948, glucocorticoids (GCs) have been widely used in medicine.1 Although GCs soon became associated with the occurrence of adverse effects (AEs), they are still the most frequently used anti-inflammatory and immune-suppressive drugs in rheumatic diseases. Recent studies have demonstrated the disease-modifying potential of low-dose GCs in rheumatoid arthritis (RA) and this has renewed the debate on the risk–benefit ratio of this treatment.2 Current literature on the risk–benefit ratio of GCs is nevertheless inconsistent, and inappropriate use of GCs could lead to increased toxicity;3 this emphasises the need for clear statements on proper use of GCs. Hence, a EULAR task force on GCs, including a patient, was formed to develop evidence-based recommendations, to provide a tool for the better use and management of GC-therapy in rheumatic diseases.
METHODS
Endorsed by EULAR-ESCISIT, a multidisciplinary guideline development committee on GCs was formed, consisting of 20 experts in the field of GCs from 11 European countries, Canada and the USA: 15 rheumatologists, 1 internist, 1 rheumatologist–epidemiologist, 1 health professional, 1 patient and 1 research fellow. The Delphi method was used to agree on 10 key propositions related to the risk–benefit ratio of GCs, and EULAR standardised operating procedures4 were then followed: (1) to identify and critically appraise research evidence for the 10 propositions, performing a systematic literature search of PUBMED, EMBASE, CINAHL and Cochrane Library; (2) to generate and validate recommendations based on the best available evidence, according to research, clinical expertise and perceived patient preference (levels of evidence are defined in table 1); and (3) to formulate a future research agenda.
RESULTS
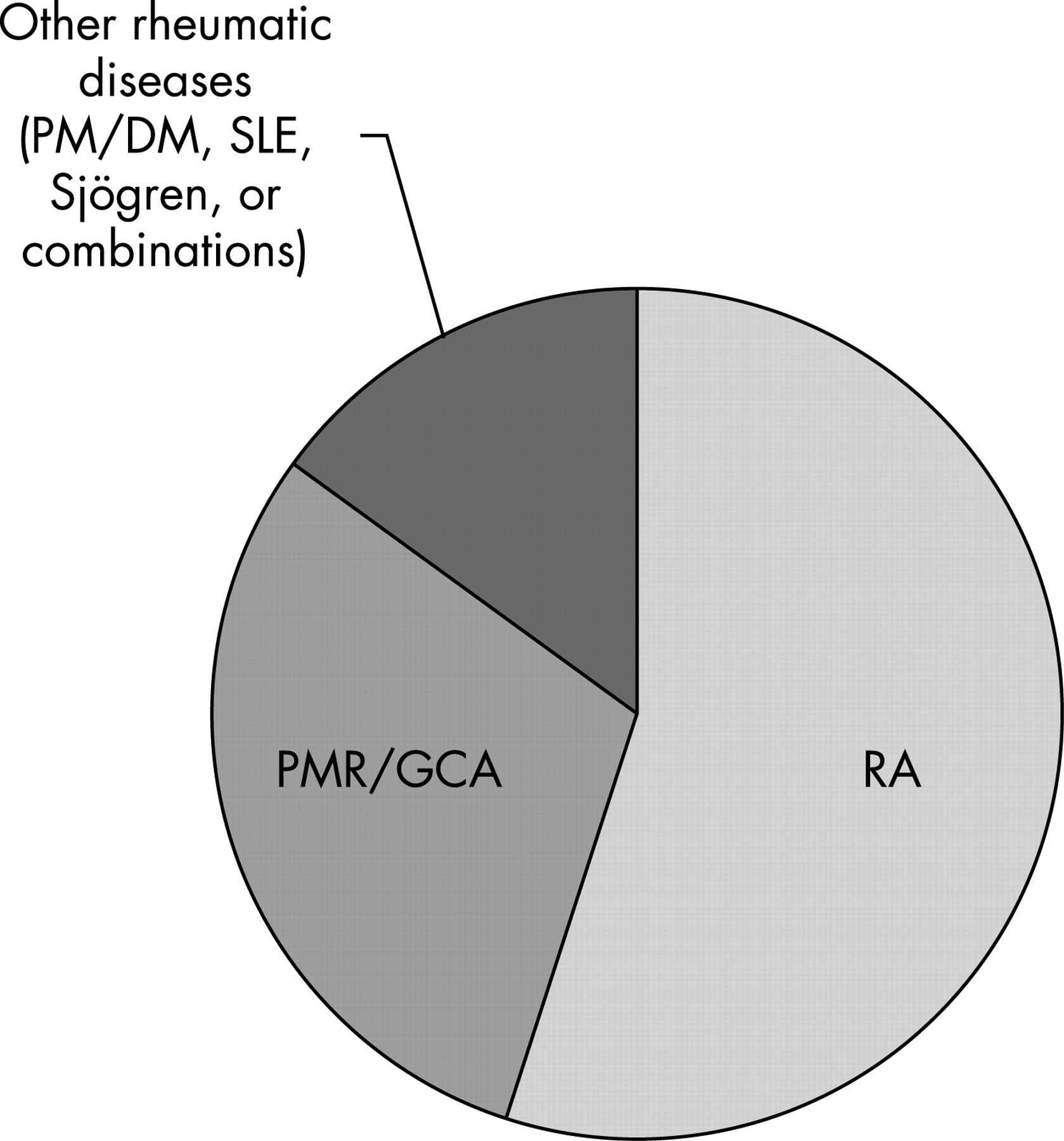
First, a general literature search was performed (appendix 1 of the full version of the article; available web-only at http://www.annrheumdis.com/supplemental), including the estimated incidence of different types of AEs as derived from studies reporting on frequencies of AEs of GCs (see fig 1 and table 2). Second, after the taskforce experts had discussed the results of this general literature search, the Delphi exercise was initiated. At the start, 153 (partly overlapping) propositions were produced, and after 2 anonymous Delphi rounds 10 final propositions were agreed upon (table 3). Third, proposition-specific searches were done, resulting in 5089 potentially useful studies, of which 165 were included to provide (circumstantial) evidence for propositions (table 4).
Recommendations
1. The adverse effects of glucocorticoid therapy should be considered and discussed with the patient before glucocorticoid therapy is started. This advice should be reinforced by giving information regarding glucocorticoid management. If glucocorticoids are to be used for a more prolonged period of time, a “glucocorticoid card” is to be issued to every patient, with the date of commencement of treatment, the initial dosage and the subsequent reductions and maintenance regimens.
Level of evidence: IV
Strength of recommendation (95% CI):
Overall: 91 (86 to 96)
Pretreatment advice: 92 (85 to 100)
Information: 88 (80 to 96)
Glucocorticoid card: 78 (67 to 89)
We recommend that the frequency of AEs during GC-therapy (table 2) should be categorised following WHO guidelines: very common (>1/10 patients); common (>1/100); uncommon (>1/1000); rare (>1/10 000); very rare (<1/100 000).5 Detailed discussion of common and very common AEs of therapy is an integral part of the management of any disease and of patient education. Because patients’ perspectives on AEs might differ from doctors’ perspectives, patient information should include both perspectives (category IV evidence). In a population-based cohort, 68% of patients who used GCs recalled discussing potential GC-related AEs with their practitioner.6 This recall might be influenced by the perception of severity of GC-related AEs, which may differ among patients.7
Whether discussion of possible AEs before GC-therapy has any beneficial effect on disease outcome—for example by improving patient compliance—is unclear because of lacking data. However, general patient education, including discussing possible AEs of other treatment, positively influences outcome of therapy.8–11 In contrast, in a controlled clinical study the knowledge about AEs of beta-blockers produced anxiety.12 So, in giving information, individual patient psychological characteristics should be taken into account. The format of patient education—for example the use of information leaflets—has not been investigated in long-term GC-therapy, so this part of the recommendation is also supported by expert opinion only. Likewise, no evidence was found to support the use of “glucocorticoid cards”, but the use of a pocket card in methotrexate (MTX) users improved patients’ knowledge on safety and toxicity of MTX.9
2. Initial dose, dose reduction and long-term dosing depend on the underlying rheumatic disease, disease activity, risk factors and individual responsiveness of the patient. Timing may be important, with respect to the circadian rhythm of both the disease and the natural secretion of glucocorticoids.
Level of evidence: I–III
Strength of recommendation (95% CI):
Overall: 83 (70 to 97)
Dose regimens: 92 (83 to 100)
Dose timing: 74 (59 to 89)
Dosing strategies were assessed in one retrospective and three prospective studies on short- to intermediate-term GC treatment in polymyalgia rheumatica (PMR) and giant cell arthritis (GCA) patients needing low initial dosages had fewer relapses and lower maintenance dose, and experienced less toxicity (category III).13–16 In early RA (disease duration <2 years), the use of low-dose GCs is based not solely on disease symptoms, but also on joint sparing effects on the long-term, as GCs can be categorised as disease-modifying antirheumatic drugs (DMARDs) (category IA).2 Different regimens with GCs have been used for joint sparing purposes in early RA, usually in combination with other DMARDs. These different schemes could result in different disease outcomes, but data are lacking.
A relation between dose strategies and risk factors, such as diabetes, hypertension and osteoporosis, can only be shown indirectly (category IIB–III).17–20 It is unknown whether an individual response on the same GC-dose is different among individuals, since no study was found on the relation between dose strategies and individual responsiveness of patients.
The timing of GC-administration might influence its efficacy, as both signs and symptoms (such as morning stiffness) of RA21 as well as serum levels of several pro-inflammatory cytokines22 show a circadian rhythm with a flare at the beginning of the day. Administration of GCs early in the morning23 (category IB), or the use of modified release tablet of prednisone, delivering the GC early in the morning (abstract)24 gave more improvement of RA symptoms than conventional timing of GC-therapy.
In conclusion, there is category III evidence on dosing regimens of GCs in PMR/GCA and category IA evidence showing a benefit for the use of low-dose long-term GCs in early RA. The relation between risk factors, AEs, high GC-dosages and long-term GC-use was indirectly shown for diabetes (category IIB) and hypertension (category III). No study was identified on individual responsiveness to GC (category IV). There are category IB data on a superior effect of circadian administration of GCs.
3. When it is decided to start glucocorticoid treatment, comorbidities and risk factors for adverse effects should be evaluated and treated where indicated. These include hypertension, diabetes, peptic ulcer, recent fractures, presence of cataract or glaucoma, presence of (chronic) infections, dyslipidemia and co-medication with non-steroidal anti-inflammatory drugs.
Level of evidence: IV
Strength of recommendation (95% CI): 92 (87 to 96)
Even though the above-mentioned risk factors for GC-associated AEs are well known,25 and there is obvious face validity trying to prevent these from occurring by assessing and treating comorbidities and risk factors at baseline, there is no evidence to show that this is effective (category IV).
4. For prolonged treatment, the glucocorticoid dosage should be kept to a minimum, and a glucocorticoid taper should be attempted in case of remission or low disease activity. The reasons to continue glucocorticoid therapy should be checked regularly.
Level of evidence: IV
Strength of recommendation (95% CI): 81 (68 to 94)
This proposition is supported by expert opinion alone, although this proposition has obvious face validity, since the occurrence of GC-related AEs, osteoporosis in particular (proposition 5 and 6), is dependent on dose and duration of therapy.
5. During treatment, patients should be monitored for body weight, blood pressure, peripheral oedema, cardiac insufficiency, serum lipids, blood and/or urine glucose and ocular pressure depending on individual patient’s risk, glucocorticoid dose and duration.
Level of evidence: IV
Strength of recommendation (95% CI): 89 (81 to 97)
There is no direct evidence from appropriately designed studies to support this proposition (category IV). Since risks of AEs during GC-treatment are related to GC-dose and duration of treatment, monitoring should be dependent on both variables. Furthermore, monitoring for an AE is especially useful if the AE is preventable or treatable, common, severe, and if the cost of screening is low and monitoring is feasible in daily clinical practice. Also, non-modifiable AEs should be assessed, as they could be important from the patient’s perspective and could be a surrogate marker for other AEs (eg, reflecting patient’s sensitivity to GCs), alerting the physician. A theoretical framework showing elements of the discussion on monitoring the above-mentioned AEs is found in table 5, based upon group consensus after discussing all propositions.
6. If a patient is started on prednisone ⩾7.5 mg daily and continues on prednisone for more than 3 months, calcium and vitamin D supplementation should be prescribed. Antiresorptive therapy with bisphosphonates to reduce the risk of glucocorticoid-induced osteoporosis should be based on risk factors, including bone-mineral density (BMD) measurement.
Level of evidence: I
Strength of recommendation (95% CI):
Overall: 95 (89 to 100)
Calcium and vitamin D: 95 (91 to 99)
Bisphosphonates: 96 (92 to 99)
Calcium and vitamin D supplementation have been shown to reduce GC-induced bone loss and fractures (category IA).26 27 However, they do not totally prevent GC-induced bone loss, in contrast to bisphosphonates, which have been proven superior in this respect (category IA).28 Bisphosphonate therapy can be indicated, based on the following risk factors: decreased BMD, female gender, older age, postmenopausal status and low body mass index (category IIB).29 Both GC-dose and low BMD have been shown to be predictors of fractures, but at the same BMD level, postmenopausal patients on GCs were more prone to getting fractures than postmenopausal patients without this therapy (category 1B).30 The ACR has published a clear guideline on the treatment of GC-induced osteoporosis,31 and several algorithms have been proposed to decide whether or not to start with bisphosphonates based on GC-dosage, pre-existent fractures, age and gender, menopause, and BMD measurement32 33 (fig 2 gives an example).

{kind=link}
{kind=link}
7. Patients treated with glucocorticoids and concomitant non-steroidal anti-inflammatory drugs (NSAIDs) should be given appropriate gastro-protective medication, such as proton pump inhibitors (PPIs) or misoprostol, or alternatively could switch to a cyclo-oxygenase-2 selective inhibitor (coxib).
Level of evidence: I
Strength of recommendation (95% CI): 91 (84 to 98)
No study investigated gastro-protective measures in GC-using patients specifically, but the rationale for this proposition is given by the fact that gastro-intestinal (GI) toxicity possibly increases by treatment with GCs alone (see proposition 3). Likewise, although not studied in GC-using patients specifically, several treatment regimens have been shown to be gastro-protective for conventional NSAID users. Proton pump inhibitors (PPIs) and misoprostol reduce the risk of gastric and duodenal ulcers in patients taking conventional NSAIDs (category I B),34 35 and cyclo-oxygenase-2 inhibitors cause less GI toxicity than conventional NSAIDs in RA patients (category I B).36–38 However, conventional NSAIDs combined with PPI cause less dyspepsia than cyclo-oxygenase-2 inhibitors do (category I A).39 In deciding on the prescription of cyclo-oxygenase-2 inhibitors and conventional NSAIDs, cardiovascular risk factors should also be taken into account.40–45
8. All patients on glucocorticoid therapy for longer than 1 month, who will undergo surgery, need perioperative management with adequate glucocorticoid replacement to overcome potential adrenal insufficiency.
Level of evidence: IV
Strength of recommendation (95% CI): 91 (84–99)
Adrenal insufficiency due to surgical stress has already been described in the 1950s.46 As patients with RA and PMR are considered to have relative adrenal insufficiency due to their disease,47 they might be more prone to adrenal insufficiency at surgery. The incidence and duration of GC-induced adrenal insufficiency depend, apart from possible individual differences in sensitivity for GC, on the type and dosage of GC48 49 and the duration of therapy. GC-treatment of less than 3 weeks or alternate-day therapy does not exclude the risk of suppression of the hypothalamic–pituitary–adrenal axis,50 51 but the risk is still dose-dependent.52
GC-replacement is recommended in case of surgery for patients at risk of adrenal insufficiency (category IV). For moderate physical stress-inducing procedures, a single dose of 100 mg of hydrocortisone intravenously has been proposed, and for major surgery, 100 mg of hydrocortisone intravenously before anaesthesia and every 8 h 4 times thereafter.53 The dose can be gradually tapered by half per day afterwards. However, several other schemes of GC-replacement exist.
9. Glucocorticoids during pregnancy have no additional risk for mother and child.
Level of evidence:
Mother: IV
Child: I–III
Strength of recommendation (95% CI): 87 (78 to 96)
Safety of GC-usage during pregnancy refers to both the mother and the unborn child. First, for the pregnant mother, the spectrum of AEs associated with the use of GCs is believed not to differ between a pregnant patient and a non-pregnant patient (category IV evidence), but since pregnant or lactating women are more at risk for pregnancy-associated Aes, which are also seen as AE of GC-therapy (eg, osteoporosis,54 diabetes,55 hypertension56), this risk of these AEs could be especially increased by GC-therapy for these women, but no data are available.
Second, regarding the safety of GCs for the fetus and neonate, dexamethasone can be used to treat fetal conditions such as immature lungs, because it is not metabolised well by the placenta, and so higher dosages are available to the fetus. Prednisone, prednisolone and methylprednisolone are less available to the fetus (10% of the maternal dose), and so these substances are preferred for the treatment of maternal disorders.57 GCs prior to and during pregnancy do not seem to have a negative impact on the development of the fetus. GCs in high doses have caused low birth weights in humans and cleft palate in experimental animal models,58 59 but there is no evidence that in humans prednisone or methylprednisolone are teratogenic (Food and Drug Administration risk category B,60), category III evidence.61 The incidence of infection was not increased in neonates who had been exposed to GCs in utero (category IB).62
GCs are excreted minimally into breast milk,63 64 and breastfeeding by women on low-dose GC-therapy is generally considered to be safe.65 Exposure of an infant can be further minimised if breastfeeding is avoided during the first 4 h after GC-intake, because there is an equilibrium between the concentration of prednisolone in mother milk and serum.64
10. Children receiving glucocorticoids should be checked regularly for linear growth and considered for growth-hormone replacement in case of growth impairment.
Level of evidence: I
Strength of recommendation (95% CI): 93 (85 to 100)
GCs can cause growth retardation in children (category I B).66–69 The pathogenesis of this growth impairment is multifaceted. Growth-hormone replacement (GHR) can be used to prevent growth impairment due to GCs: an increase in linear growth with GHR was shown in several studies of GC-using JIA patients (category I–III),70–75 and in studies of “slowly growing GC-treated patients” (category II).76 77 The daily GC-doses used in these studies varied between 0.2 and 0.5 mg/kg prednisolone equivalent, and the duration GHR therapy was 2–4 years.
If GHR is considered, referral to an experienced paediatrician is indicated (category IV evidence), and additional testing can confirm growth-hormone deficiency. Routine usage of GHR in GC-using patients is hampered by several factors: the therapy involves daily injections (subcutaneously or intramuscularly), the length gain is relatively small, and it is a very costly therapy (between €15 000 and €50 000 annually, depending on the weight of the individual child78).
DISCUSSION
This EULAR document on the safer use of systemic GCs in rheumatic diseases used a similar design to that of earlier EULAR taskforces,79–82 i.e. a combination of both evidence and expert opinion. The added value of this taskforce, like previous ones, is provided by the fact that they (1) are a broad representation of experts in the field of GCs within and outside Europe; (2) use recent research data; and (3) use a thorough evidence-based format. The order of 10 propositions in the paper does not reflect importance, but more or less the logical order of patient management. Both the level of evidence of each proposition and the strength of recommendations are given. This approach has led to a reduction of personal bias, good external validity and generalisability, and clear identification of areas of clinical practice where more research data are required.83 The propositions promote the safer use of GCs among physicians and patients alike in daily clinical practice, and they will form the basis of further EULAR research and education.
These recommendations have some limitations. Since GCs are used quite extensively, the search results were often overwhelming. To overcome this, we used more specific search strategies in which relevant studies might have been overlooked. Second, the selection of circumstantial evidence in the absence of direct evidence has some degree of subjectivity. Third, in the literature, the evidence hierarchy has focused on treatment efficacy, whereas evidence on safety might be better graded by other study types than RCTs. Other grading systems might be preferred for grading future studies on safety.
The literature search showed that studies on GCs in general lack a systemic assessment of AEs and that AEs often are poorly described, let alone defined, which made it difficult to provide direct evidence for most propositions. It is therefore advisable to monitor a well-defined list of AEs in a standardised manner in future studies, taking into account patients’ perspectives, but standardised scoring for most AEs has yet to be developed. Hypertension, diabetes, osteoporosis, gastric ulcer, cataract, glaucoma, infections, and dyslipidaemia are AEs that merit monitoring. To point out the most important topics for future research on GCs, a research agenda of 11 research questions has been formulated through 2 additional Delphi rounds (table 6).
Acknowledgments
Professor H Capell, Centre for Rheumatic Diseases, Royal Infirmary Glasgow, Scotland, UK, participated in the taskforce during the Delphi exercises.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
This is an abbreviated version of the article; the full version is available online at http://ard.bmj.com/supplemental
Competing interests: None declared.
- Abbreviations:
- AE
- adverse effect
- BMD
- bone-mineral density
- DMARD
- disease-modifying antirheumatic drug
- GC
- glucocorticoid
- GCA
- giant cell arthritis
- GHR
- growth-hormone replacement
- NSAID
- non-steroidal anti-inflammatory drug
- PMR
- polymyalgia rheumatica
- PPI
- proton pump inhibitor
- RA
- rheumatoid arthritis