Article Text

Abstract
To understand better a complex disease such as psoriatic arthritis (PsA), collection of a large amount of information on clinical, laboratory, and radiological features is required over an extended period of time. Longitudinal data can be effectively collected and stored in clinical registries and databases. This article reviews current databases in PsA and proposes a structure for an international PsA registry. Careful collection and analysis of patient data through collaborative efforts will likely advance our knowledge of pathogenesis and provide new and much needed insights about the course and prognosis of the disease.
- psoriatic arthritis
- registries
- genomics
- databases
- prognosis
Statistics from Altmetric.com
The study of a complex disease such as psoriatic arthritis (PsA) requires collection of a large amount of information on clinical, laboratory, and radiological features over prolonged periods of time. The best approach to learn about the course and prognosis of the disease, as well as to identify new features, is through clinical registries and databases.
UNIVERSITY OF TORONTO PSA CLINIC DATABASE
A PsA registry/database has been developed at the University of Toronto Psoriatic Arthritis Clinic, and over 650 patients with PsA have been followed prospectively since 1978 according to a standard protocol.1 Patients are admitted into the PsA Clinic Database if they have an inflammatory arthritis associated with psoriasis, but without evidence of another rheumatological disorder such as seropositive nodular rheumatoid arthritis, gout, grade 4 osteoarthritis, or inflammatory bowel disease.1 Demographic, clinical, and laboratory information on patients with PsA is recorded at six month intervals and tracked on the database. The assessments of actively inflamed joints (those with tenderness and/or swelling) and clinically damaged joints (those with deformity, flail, or ankylosed joints) have been shown to be reproducible in the Clinic.2 Other clinical features, such as dactylitis, enthesitis, tenosynovitis, and skin and nail lesions, are also recorded. Standard evaluation of skin lesions according to the Psoriasis Area and Severity Index (PASI) was added in 1991. Concurrent illnesses are recorded at each protocol visit, as are all medications. Radiographic assessments (hands, feet, complete spine, and pelvis) are performed at two year intervals. Peripheral joints are read according to a modification of the Steinbrocker method, which has been proved reliable in the Clinic.3 Sacroiliac joint radiographs are read according to the American College of Rheumatology (ACR) criteria for sacroiliitis, and syndesmophytes are recorded in the cervical, thoracic, and lumbar regions. Other radiological features of PsA, such as enthesitis, periostitis, spurs, tuft resorption, are also collected. Several studies have been published from this database, outlining new concepts in disease presentation and progression.4–8
In addition, information on health status and quality of life is entered through completion of the Health Assessment Questionnaire (HAQ) which includes questions on psoriasis,9 the Medical Outcome Survey Short Form 36 (SF-36),10 and the Fatigue Severity Scale.11
Oracle (Oracle, CA) was chosen as the database for three reasons:
-
A large amount of information can be collected at each visit and entered in a tabular format.
-
Data can be added without interfering with information already collected.
-
Oracle is a dynamic database and is easily transferable to an SAS format for more robust statistical analysis.
The University of Toronto PsA Clinic Database has both clinical and genetic components. Genetic information is also collected on all probands and any available family members. DNA is isolated from all patients registered in the PsA Clinic following informed consent. Genetic information is compiled in the laboratory database and can easily be collated with the clinical information. This has allowed determination of the relation between certain human leucocyte antigen (HLA) alleles and disease progression, as well as the conclusion that the HLA is a candidate region in PsA.12–14.
OTHER REGISTRIES
A similar registry has been developed at Memorial University, St John’s, Newfoundland by Proton Rahman. In addition to patient data collection, DNA from all patients is stored; a study from this cohort identified a gene for PsA on chromosome 16q.15
The original data gathered by John Moll and Verna Wright in Leeds, England, was kept on card index files in Dr Moll’s office.16 Roberts accessed patients using this resource for an outcome paper in the late 1970s.17 Helliwell abstracted data from 50 cases using the same resource in the late 1980s and published a re-evaluation of osteoarticular features in psoriasis.18
Adjoining Leeds, Bradford has a large diagnostic index based on Dataflex software at St Luke’s Hospital, where basic clinical and radiological information can be saved.19,20 Helliwell introduced this software in Huddersfield; two other sites in Yorkshire also have the same software. Data on approximately 800 patients with PsA have been entered into this database, using the Moll and Wright classification.
Neil McHugh developed a registry for PsA in Bath, England, which included data on 100 patients collected before 1994.21 Over the past 15 years, more than 400 patients have been included in this cohort. The present database (Access 2000, Microsoft) includes core demographic and baseline information as well as follow up visits, activity data on tender, swollen, and damaged joints, PASI, nail scores, and radiographs. More recently, DNA and serum have been stored on a more regular basis (N McHugh, personal communication). McHugh and colleagues, using this database, showed that PsA progresses over time22 and demonstrated that shared epitope alleles are associated with erosive disease in PsA.23
A new registry was recently created in Sweden for the detection of early PsA.24 This was developed as a national PsA programme, and those patients whose disease duration is less than two years are enrolled. This cohort includes patients with symptoms and/or signs consistent with PsA. The information collected is similar to that outlined above for the University of Toronto PsA Clinic and includes clinical and laboratory assessments, patient derived questionnaires, and radiographic assessments. Of the 92 patients included in the programme between 1 January 2000 and 1 August 2001, 60 were diagnosed as having PsA and 32 were possible PsA. The programme is easy to administrate and not overly time consuming in daily clinical practice (U Lindqvist, personal communication). Another PsA database in Sweden is that of Gerd Marie Alenius (G M Alenius, personal communication) who has collected information on ∼400 patients with PsA as well as some families for genetic studies.
The Rheumatology Unit II of the University of Cagliari (Sardinia) has a database for patients with PsA containing demographic data, disease onset, clinical subset classification, extra-articular manifestations, drug history, and tissue typing of HLA alleles and HLA selected polymorphisms (A Cauli, personal communication).
A PsA registry was recently developed in New York under the supervision of Soumya Reddy and Clifford Bingham (C Bingham, personal communication). Patients with PsA are followed according to a standard protocol, based on the University of Toronto protocol. Samples are obtained for biological studies as well.
GOALS OF AN INTERNATIONAL REGISTRY
Although these individual databases are helpful, a large PsA collaborative registry would allow investigators to approach fundamental questions about the contribution of genetic and environmental factors in the aetiology of the disease and gain better understanding of the pathophysiological mechanisms underlying synovitis, soft tissue inflammation, and joint destruction in patients with PsA. In addition, data derived from this registry would assist in the development and evaluation of new diagnostic modalities and therapies in PsA. In an international registry a larger cohort of patients can be assembled, and clinical, demographic, and laboratory data will be continually collected and updated. The registry would also serve as a repository of tissue, sera, and DNA.
On the basis of the nature of the disease and the research needs outlined above, the goals of a PsA registry should include:
-
enrolment of large numbers of patients
-
availability of patients representative of the broad spectrum of PsA, both clinically and radiographically
-
use of international consensus classification criteria for PsA
-
longitudinal follow up of clinical, serologic, and radiographic data
-
recruitment of patients/subjects from different specialists representing the clinical spectrum of PsA.
A large collaborative registry can significantly benefit all areas of PsA research. The ability to study relatively large, homogeneous groups of patients will foster studies focused on identifying basic immunological and genetic abnormalities and delineating specific pathophysiological mechanisms. Availability of tissue, sera, plasma, and DNA is essential for immunological and genetic studies. Furthermore, a large, well defined patient population and serum bank will contribute to studies seeking to correlate clinical manifestations with conventional and newly defined mediators of inflammation. The ability to enrol homogeneous subsets of well classified patients with PsA will be a tremendous advantage for clinical investigators recruiting patients for clinical trials testing new therapeutic agents or approaches.
PROPOSED STRUCTURE FOR AN INTERNATIONAL REGISTRY
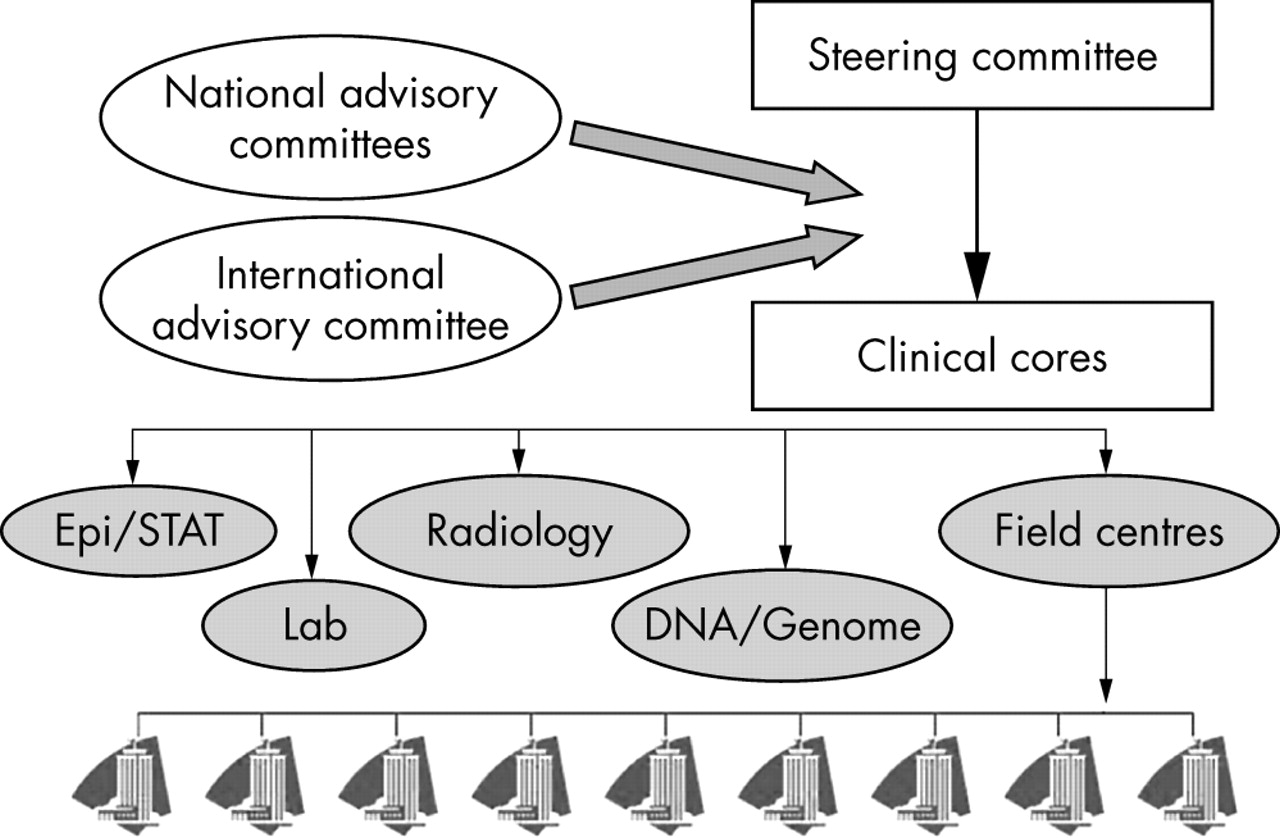
An outline of the proposed structure for an international PsA registry is depicted in fig 1. The registry would consist of a coordinating centre, which will maintian the demographic and clinical database and the tissue repository. Serum and DNA would be stored at a biorepository able to process and store a large number of samples, following strict patient confidentiality guidelines. We favour a collaborative approach to the registry to take advantage of the extensive PsA clinical research experience of investigators worldwide—those with established research programmes in PsA would constitute the registry steering committee. This committee, chaired by the principal investigator (PI)/director, would be responsible for making decisions about enrolment criteria, data collections forms, overall database structure, classification of unusual patients, and evaluation of proposals to access registry resources. Whenever possible, the goal is for these decisions to be made by consensus. The committee would meet annually to discuss patient enrolment and review grant applications. To broaden the spectrum of opinions available to the PI/director and the steering committee, several international experts would be invited to assist in defining research agendas and advise on ongoing research projects.
{kind=link}
Proposed structure for an international psoriatic arthritis registry. Epi/STAT, epidemiology and biostatistics.
The activity of such an international registry will require availability of a full time study coordinator at the coordinating centre to assist the PI/director and be responsible for data entry and maintenance of the database and repositories. In addition, coordinators at collaborating centres worldwide will be needed to ensure recruitment and enrolment of patients. An epidemiology and biostatistics core is an essential component of a registry. Serum, plasma, and buffy coat cells will be obtained from all patients enrolled in the registry. These specimens will be stored at the biorepository. Rheumatoid factor, erythrocyte sedimentation rate, and C reactive protein would be assessed, and biomarker assays performed at a core lab facility.
Registry information and specimens should be made available to the scientific community. Thus, investigators wishing to use these resources would need to apply to the coordinating centre; an application form developed and approved by the steering committee will facilitate this process. The steering committee chaired by the PI/director would evaluate and approve or reject these applications. Basic criteria for granting the application will be as follows:
-
The applicant and collaborators must be bona fide investigators capable of conducting the proposed experiments.
-
The question being asked must be scientifically legitimate.
-
The proposed study must be ethical and conducted under the approval of the investigator’s institutional review board and/or animal care and use committee.
-
The proposed study will have sufficient statistical power to answer the question being asked.
A major issue for both existing databases and the proposed international registry is adequate funding. A few investigators have obtained some funding through peer review process, but the funding has not been maintained. This is an increasingly costly endeavour, and although individuals working in the field appreciate its importance, granting agencies and individual reviewers may not share this view. The development of an international registry for PsA will require a major funding commitment to create and maintain this important initiative.