Article Text

Abstract
Objective To investigate the kinetics of hepatitis B virus (HBV) viral loads and HBV reactivation in rheumatoid arthritis (RA) patients undergoing therapy with tumour necrosis factor alpha (TNFα) inhibitors.
Methods The authors investigated the virological, serological and biochemical evidence of HBV reactivation in 88 RA patients receiving anti-TNFα therapy. Levels of HBV surface (HBs) antigen (Ag), anti-HBV core (HBc)-IgG and anti-HBs antibody (Ab) were detected by electrochemiluminescence immunoassay, and viral loads were determined by real-time PCR assay.
Results In a total of 88 HBcAb-positive patients, 18 (20.5%) patients were HBsAg-positive, 12 (13.6%) patients were HBsAg-negative/HBsAb-negative and 58 (65.9%) patients were HBsAg-negative/HBsAb-positive before starting anti-TNFα therapy. Among HBsAg-positive patients receiving anti-TNFα therapy, HBV reactivation was documented in none of 10 patients who received lamivudine pre-emptive therapy and serum viral loads significantly decreased (mean±SEM, 153 860±80 120 IU/ml at baseline vs 313±235 IU/ml after 12 months antiviral therapy, p<0.001), paralleling the decrease in serum aminotransferase levels. In contrast, five (62.5%) of eight patients without antiviral prophylaxis developed HBV reactivation, viral loads significantly increased after anti-TNFα therapy (9375±5924 IU/ml vs 49 710 000±40 535 000 IU/ml, p<0.001), and markedly declined after antiviral therapy (49 710 000±40 535 000 IU/ml vs 6382±2424 IU/ml, p<0.001). Baseline viral loads were detectable in four (33.3%) of 12 patients who had HBsAg-negative/HBsAb-negative status, and one developed HBV reactivation after anti-TNFα therapy.
Conclusion HBV reactivation can occur in both HBsAg-positive and HBsAg-negative/HBcAb-positive patients with detectable HBV DNA, so-called occult HBV infection, during anti-TNFα therapy. Antiviral prophylaxis may effectively reduce HBV reactivation in HBsAg-positive RA patients undergoing anti-TNFα therapy.
Statistics from Altmetric.com
It is estimated that more than one-third of the world's population has been infected with the hepatitis B virus (HBV) and that 75% of these people live in southeast Asia and the western Pacific regions.1 Taiwan is an endemic area of HBV infection, with an HBV surface antigen (HBsAg) carrier rate of 15–20% and HBV core antibody (HBcAb) positive rate of 80–90%.2 3
Tumour necrosis factor alpha (TNFα) suppresses HBV replication and plays an important role in eradicating HBV by stimulating HBV-specific cytotoxic T-cell response.4,–,6 HBV reactivation is a recently recognised complication characterised by the abrupt reappearance or rise of HBV DNA in the sera of HBsAg-positive rheumatoid arthritis (RA) patients who received anti-TNFα therapy.7,–,10 Guidelines have been proposed for the assessment and antiviral therapy of chronic HBV infection in patients receiving anti-TNFα therapy.11 12 Despite such a high prevalence of HBV in Taiwan, there is no national guideline for effective screening of HBV or prophylactic antiviral strategies in RA patients receiving anti-TNFα therapy.
Recent studies showed that HBV reactivation could also occur in occult HBV infection patients receiving cytotoxic chemotherapy or immunosuppressive therapy, most of whom had HBcAb-positive status.13,–,16 Accumulative cases developed severe or fulminant hepatitis due to HBV reactivation after anti-TNFα therapy and rituximab-based regimens in HBsAg-negative patients.17 18 Despite these findings, the precise incidence or risk factors of HBV reactivation in RA patients with occult HBV carriers have not yet been defined. Systemic evaluation of the relationship between HBV reactivation and anti-TNFα therapy is limited in RA patients.18 19
Prophylactic antiviral therapy has been demonstrated to have excellent efficacy in the prevention of HBV reactivation for HBsAg-positive patients treated with anticancer agents including rituximab-containing immunochemotherapy.20,–,22 However, effective monitoring, risk assessment for HBV reactivation, and the benefit of prophylactic antiviral therapy for RA patients receiving anti-TNFα therapy have not been widely reported.11
The aim of this study was to investigate the virological, serological and biochemical evidence of HBV reactivation in 88 RA patients who had a different status of HBV infection and were treated with TNFα inhibitors. We also examined the dynamic change in the HBV viral loads in RA patients during a 1-year therapy period with TNFα inhibitors.
Patients and methods
Patients
We retrospectively reviewed the medical records of 106 consecutive RA patients who fulfilled the 1987 revised criteria of the American College of Rheumatology for RA23 and received anti-TNFα therapy from January 2006 to June 2009 at Taichung Veterans General Hospital. Of these patients, we included 88 patients (77 women and 11 men; mean age±SD, 50.1±12.0 years) with positive anti-HBc-IgG, which is a marker of previous exposure to HBV. Disease activity was determined using the 28-joint disease activity score (DAS28).24 All patients had been treated with methotrexate and other disease-modifying antirheumatic drugs, but still had active disease, so anti-TNFα therapy was initiated based on the British Society for Rheumatology guidelines.25 Etanercept was given at a dose of 25 mg twice weekly in 40 patients and adalimumab was given at a dose of 40 mg every other week in 48 patients in combination with a stable dose of methotrexate 7.5–15 mg weekly and corticosteroids 2.5–10 mg daily. The Clinical Research Ethics Committee of Taichung Veterans General Hospital approved the study, and informed consent was obtained from each participant.
Definitions
Hepatitis was defined as a threefold or more increase in ALT that exceeded the upper limit of normal (44 U/l) or an absolute increase of ALT to more than 100 U/l.26 27 HBV reactivation was defined as a change to a positive HBsAg, serum HBV DNA greater than 105 (>2.6 log) copies/ml or a 10-fold rise in HBV DNA.28 The diagnosis of de-novo HBV-related hepatitis was made when hepatitis occurred in a patient whose HBsAg reversed from negative to positive, or an elevation of the serum HBV-DNA level exceeded 105 copies/ml after immunosuppressive therapy.29 Occult HBV infection was defined as the presence of HBV DNA in blood and/or hepatocyte without a detectable HBsAg.30 31 Resolved HBV infection was defined as the presence of a past HBV infection with positive HBcAb, but undetectable serum HBV DNA and HBsAg, and normal ALT levels.32 33
Serological and virological evaluation for HBV infection
The stored serum specimens were obtained in 88 RA patients before starting therapy (as a baseline) and undergoing therapy with TNFα inhibitors. HBsAg, HBcAb and hepatitis B surface antibody (HBsAb) were determined by electrochemiluminescence immunoassay (Roche Diagnostics, Mannheim, Germany). If a positive HBsAg was observed, hepatitis envelope antigen (HBeAg) and antibody test was conducted immediately. Serum DNA was extracted using a High Pure Viral Nucleic Acid kit (Roche, Mannheim, Germany) according to the manufacturer's instructions. Serum HBV genome was quantified by Roche Cobas TaqMan HBV Test (Roche Diagnostics, Basel, Switzerland), with a detection limit of 12 IU/ml. Two-hundredths of a microlitre of double distilled water served as a blank control to ensure all reagents and extraction equipment were free from contamination.
Statistical analysis
Results are presented as the mean±SD unless specified otherwise. The non-parametric Kruskal–Wallis test was used for between-group comparison of serum viral loads. Only when this test showed significant differences were the exact p values determined using the Mann–Whitney U test. A multivariate logistic regression analysis was used to evaluate the risk factors for HBV reactivation in RA patients. For comparison of serum viral loads during follow-up for RA patients before and after anti-TNFα therapy or antiviral therapy, the Wilcoxon signed rank test was employed. A probability of less than 0.05 was considered to be significant.
Results
Clinical characteristics of RA patients
The background characteristics and HBV status of RA patients before starting anti-TNFα therapy are shown in figure 1 and table 1. Eighteen (20.5%) RA patients had positive HBsAg, 12 (13.6%) patients had HBsAg-negative/HBsAb-negative status and 58 (65.9%) patients had HBsAg-negative/HBsAb-positive status before starting anti-TNFα therapy. All RA patients had active disease (median DAS28, 7.17; range 5.23–8.75). None of 10 HBsAg-positive patients who received lamivudine therapy (prescribed for three patients according to Taiwan's treatment guidelines and another seven patients because of immunosuppressive treatment) developed HBV reactivation. In this retrospective study, out of the eight patients who were found to be HBsAg positive and should have been given prophylactic antiviral therapy before starting anti-TNFα therapy, five (62.5%) developed HBV reactivation. Elevated hepatic enzymes (ALT) were normalised within 3 months after initiation of antiviral therapy in all patients with HBV reactivation. In addition, higher viral loads at baseline were observed in HBsAg-positive patients with reactivation than in those without reactivation (118 568±229 439 IU/ml vs 21 706±28 838 IU/ml, p=0.160).

Flowchart shows the distribution of serological and virological results for hepatitis B virus (HBV) infection at baseline and the development of HBV reactivation in 88 rheumatoid arthritis (RA) patients who had a different status of HBV infection and were treated with tumour necrosis factor alpha inhibitors. HBcAb, antibody against HBV core antigen; HBsAb, antibody against HBV surface antigen; HBsAg, HBV surface antigen.
Demographic data and laboratory findings of RA patients with different status of HBV infection†
There was one episode of breakthrough hepatitis associated with lamivudine-resistant HBV mutants at the tenth month of lamivudine therapy. This patient with breakthrough hepatitis had a higher level of baseline HBV DNA (421 400 IU/ml) when compared with those without breakthrough hepatitis (median 32 100 IU/ml, IQR 9930–111 150 IU/ml) and also an elevated ALT level (more than two times the normal value). Four patients who had HBsAg-negative/HBsAb-negative/HBcAb-positive status and detectable viral loads should be regarded as having an occult HBV infection. These patients had low viral loads at baseline (124, 186, 358 and 520 IU/ml) with HBeAg seronegativity, but one of them developed HBV reactivation with seroconversion during an interval of 5-month anti-TNFα therapy. Eight HBsAb-negative/HBcAb-positive patients and 58 HBsAb-positive/HBcAb-positive patients, who did not have detectable viral loads should be regarded as having resolved HBV infection, and none of them developed HBV reactivation during the 12-month anti-TNFα therapy. There was no significant difference in demographic data, disease duration, female proportion, disease activity including DAS28 and erythrocyte sedimentation rate, positive rate of serum rheumatoid factor, the daily dosage of corticosteroids or the dosage of methotrexate among RA patients with different status of HBV infection before anti-TNFα therapy (table 1).
Characteristics of RA patients who developed HBV reactivation after anti-TNFα therapy
As illustrated in table 2, all six patients were women and were receiving corticosteroids 5.0–7.5 mg daily and methotrexate 12.5–15 mg weekly at the time of HBV reactivation. Before starting anti-TNFα therapy, five patients had chronic hepatitis B (viral loads >2000 IU/ml) with HBeAg seronegativity, and another patient had an occult HBV infection with low viral load (520 IU/ml). None of these patients had blood transfusion history, new usage of hepatotoxic agents or novel HBV infection resulting from iatrogenic procedure after anti-TNFα therapy. At the time of HBV reactivation, 47 to approximately 228 505-fold increases of viral loads were observed when compared with baseline levels. HBV-related hepatitis completely resolved after antiviral therapy in all patients. Among RA patients who had detectable HBV DNA, no significant difference in demographic data, disease duration, disease activity, the dose of corticosteroids or methotrexate, or the type of TNFα inhibitors was observed between those with and without HBV reactivation (data not shown).
Clinical, serological and virological characteristics in RA patients who developed hepatitis B reactivation
Change in HBV viral loads and HBsAb titres during anti-TNFα therapy
Twenty-two RA patients with detectable HBV DNA were available for kinetic analysis of viral loads. Among individuals without antiviral prophylaxis, viral loads significantly increased early in 1-month therapy with TNFα inhibitors (155 027±75 080 IU/ml vs 9375±5924 IU/ml at baseline, p<0.005), reached its peak (49 706 366±40 534 682 IU/ml) at the time of HBV reactivation, and promptly declined after institution of antiviral therapy (49 706 366±40 534 682 IU/ml vs 6382±2424 IU/ml; figure 2A). In patients with prophylactic or pre-emptive therapy, serum viral loads were observed to decrease significantly early in the 1-month therapy with lamivudine (105 110±76 724 IU/ml vs 153 860±80 120 IU/ml at baseline, p<0.01) and further decline after 12 months of antiviral therapy (313±235 IU/ml), paralleling the decrease in serum ALT levels (65.6±7.2 U/ml at baseline vs 25.1±2.5 U/ml at month 12, p<0.01; figure 2B). Among 58 patients who had resolved HBV infection (HBsAg-negative/HBsAb-positive status), serum viral loads were not detectable before and after 12-month anti-TNFα therapy, while serum titres of HBsAb significantly decreased after 12-month therapy with TNFα inhibitors (1323.4±648.3 U/ml vs 253.9±47.7 U/ml, p<0.001).
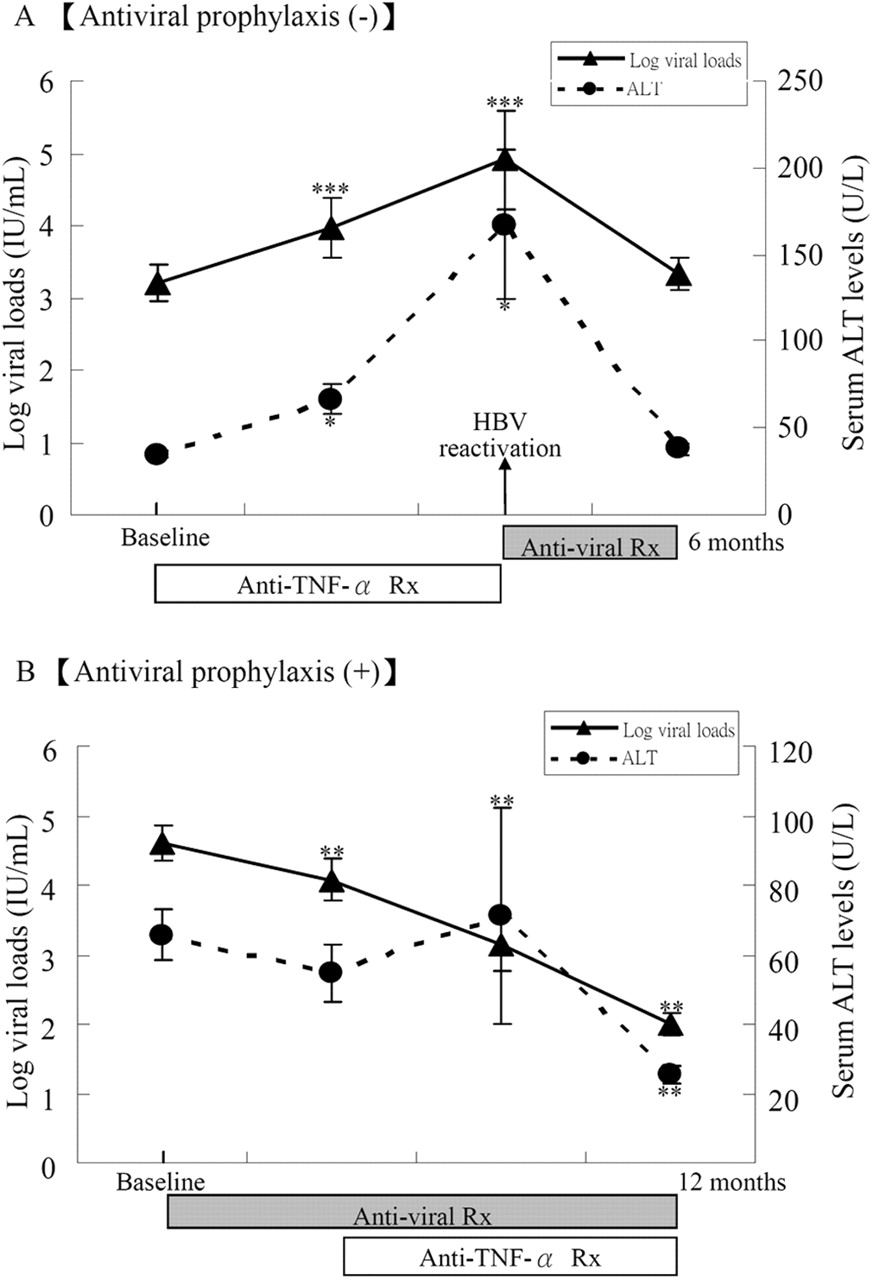
The kinetics in serum levels of viral loads and ALT in rheumatoid arthritis patients with detectable hepatitis B virus (HBV) genome, including (A) 12 patients without antiviral prophylaxis and (B) 10 patients receiving antiviral prophylaxis during a 12-month follow-up period. Data are presented as mean±SEM. *p<0.05, **p<0.01, ***p<0.005, versus values at baseline. TNFα Rx, tumour necrosis factor alpha treatment.
Multiple logistic regression analysis
In the multiple logistic regression analysis controlling for various potential confounding factors such as gender, isoniazid prophylactic therapy, antiviral prophylaxis, the type of TNFα inhibitors and therapeutic response, only a lack of antiviral prophylaxis was a significant risk factor for HBV reactivation (p<0.05).
Discussion
HBV reactivation in HBsAg-positive patients is a frequent complication, occurring in 21–53% of HBV carriers who receive cytotoxic agents or immunosuppressants, and may yield to acute hepatitis and even hepatic failure.34 The probability of HBV reactivation in HBsAg-positive RA patients is thought to be high in Taiwan where HBV is endemic.2 3 35 The present study is the first attempt to investigate HBV reactivation in RA patients who have a different status of HBV infection and are undergoing anti-TNFα therapy. Our results showed that HBV reactivation was documented in five (27.7%) of 18 HBsAg-positive patients and one (25%) of four patients with occult HBV infection during 1-year anti-TNFα therapy. Our results were consistent with those of previous reports showing a high incidence of HBV reactivation in RA patients undergoing anti-TNFα therapy.9 10 Our findings also supported the possibility that TNFα inhibitors could cause HBV reactivation just as cytotoxic chemotherapy did for lymphoma in HBV carriers.36 In addition, a trend towards a higher risk of HBV reactivation was observed among patients who had higher viral loads at baseline when compared with those with lower viral loads.
Although fatal hepatitis due to HBV reactivation has been reported sporadically in HBsAg-negative RA patients,13,–,15 the precise incidence or risk factors of HBV reactivation in those with occult HBV infection has not yet been defined. In the present study, 12 HBcAb-positive patients demonstrated a HBsAg-negative/HBsAb-negative status before starting anti-TNFα therapy. Unexpectedly, four (33.3%) of them had detectable serum HBV DNA, so-called occult HBV infection. The occurrence of occult HBV infection could involve different mechanisms, including HBV mutants that are not recognised by current assays for HBsAg,37 hindrance of HBsAg through circulating immune complex,38 co-infection with hepatitis C virus,39 chronic carriage status with HBsAg too low to be detected35 or low levels of viraemia in the condition of immunosuppression.9 36 Although we did not investigate HBsAg mutants that prevent the detection of HBsAg with current assays, our patients with occult HBV infection had low viral loads and had undergone long-term immunosuppressive therapy, which may be contributing factors. In addition, one of our four patients with occult infection developed HBV reactivation with seroconversion after anti-TNFα therapy. It is clinically important for physicians to be aware that a failure to detect an occult HBV infection, with a previous HBsAg-negative status, may result in a delayed diagnosis or antiviral therapy for HBV reactivation. Therefore, baseline and periodic monitoring of HBsAg, ALT levels and viral loads is recommended for RA patients with occult HBV infection, so that HBV reactivation can be detected early and antiviral therapy be given at an asymptomatic stage.
On the contrary, none of our HBs-negative patients with resolved HBV infection (positive HBcAb without detectable viral loads) developed HBV reactivation. Our observation was consistent with the result of a recent study showing that the incidence of HBV reactivation was low in RA patients whose HBV infection had been resolved.40 However, recent studies showed that HBV reactivation after immunosuppressive or biological therapy may also occur in HBV-resolved patients who are negative for HBsAg and positive for HBcAb, with/without positivity for HBsAb.40 41 Based on these observations, careful monitoring should be implemented when HBV-resolved patients are undergoing anti-TNFα therapy.
The exact mechanism of HBV reactivation is unknown in RA patients undergoing anti-TNFα therapy. HBV reactivation is uncommon in RA patients receiving immunosuppressive agents such as azathioprine and low doses of corticosteroids, but has been reported in those who received long-term methotrexate therapy.42,–,44 In the present study, we showed no difference in the dose of corticosteroids or methotrexate between RA patients with and without HBV reactivation. Previous studies showed that TNFα inhibits HBV replication and stimulates HBV-specific T-cell responses, suggesting that TNFα plays an important role in clearing HBV from infected hepatocytes.4 5 45 Therefore, TNFα inhibitors may allow viral replication to escape, resulting in the spread of infection within hepatocytes and an increase in circulating viral loads. Our study for the kinetics of HBV genomes showed a significant increase in HBV viral loads with a subsequent increase in serum ALT levels early at the first month of anti-TNFα therapy (figure 2A). Viral loads markedly elevated in parallel with the emergence of HBV reactivation in patients undergoing anti-TNFα therapy suggest that TNFα inhibitors may play a critical role in HBV reactivation beyond the effects of corticosteroids and disease-modifying antirheumatic drugs. The parallel change in elevated ALT levels and HBV viral loads suggests the association of abnormal liver function with the reactivation of HBV. In addition, HBV reactivation seems to have been a class effect of TNFα inhibitors because half of our patients received etanercept and the other half receive adalimumab.
Consistent with the findings of recent studies,19 46 no HBV reactivation was observed in our HBV-resolved patients with positive HBsAb who were undergoing anti-TNFα therapy. Our results also support the findings of a previous study showing that HBsAb may prevent HBV reactivation in recipients of liver grafts from donors with positive HBcAb.47 In addition, the results of our study and previous reports19 46 showed a significant decrease in serum HBsAb titre in patients with resolved HBV infection (HBsAg-negative/HBsAb-positive) after 12-month therapy with TNFα inhibitors. These observations may be explained by the finding of a recent study showing a decreased frequency of circulating CD27+ memory B cells in RA patients treated with an anti-TNFα agent (etanercept) when compared with those treated with methotrexate.48 Our results were also in agreement with previous reports showing reduced serological response to flu vaccination in RA patients during anti-TNFα therapy.49 50 Our findings concerning a decreased HBsAb level after anti-TNFα therapy may pose a potential risk of new-onset HBV infection for these patients.
Antiviral prophylactic therapy significantly reduced the incidence of HBV reactivation in HBsAg-positive patients receiving cytotoxic chemotherapy, immunosuppressive therapy and rituximab therapy.20,–,22 51 A recent meta-analysis of the role of lamivudine prophylaxis in preventing HBV reactivation has provided support for its effectiveness.52 None of our RA patients who received prophylactic therapy developed HBV reactivation, whereas five (62.5%) of HBsAg-positive patients without antiviral prophylaxis developed HBV reactivation. Our data were consistent with those of previous reports showing that HBV reactivation was documented in 14% of patients receiving antiviral prophylaxis compared with 73% of patients without prophylaxis,9 indicating the efficacy of antiviral prophylaxis in preventing HBV reactivation.20,–,22 52 In addition, we showed that a lack of antiviral prophylaxis was a significant risk factor for HBV reactivation. Given the safety and tolerability of current antiviral therapy,51 52 clinical guidelines from expert groups recommend antiviral prophylaxis to prevent HBV reactivation in high-risk patients.53 54 Consistent with the proposal of previous studies,55 our findings suggest that the coadministration of antiviral agents in HBsAg-positive RA patients need not preclude anti-TNFα therapy.
In the present study, one patient with high viral loads at baseline developed breakthrough hepatitis at the tenth month of lamivudine therapy. Our results support the findings of previous studies showing that a high viral load at baseline was an independent risk factor for the evolution of lamivudine resistance mutations,56 and the prolonged use of lamivudine is associated with the development of resistance.57 Therefore, a high genetic barrier to resistance such as entecavir and adefovir would be chosen first in patients who have high viral loads and are anticipated to receive therapy for more than 12 months in whom there is a high risk of lamivudine resistance. However, the optimal duration of antiviral prophylactic therapy has not yet been conclusively determined. Large, prospective and well-designed randomised controlled studies are needed to address this issue.
Based on our results, the findings of previous reports,7,–,20 40 41 and the current treatment guidelines,31 32 we recommend an algorithm (figure 3) with an emphasis on appropriate HBV screening and prophylactic/pre-emptive antiviral therapy before starting anti-TNFα therapy. It is reasonable to recommend that rheumatic patients who are scheduled for anti-TNFα therapy should receive up-front screening of HBsAg and HBcAb. Consideration of a high risk of HBV reactivation in HBsAg-positive patients without antiviral therapy, HBV viral loads should be checked and pre-emptive therapy be given before starting anti-TNFα therapy. For HBsAg-negative/HBcAb-positive patients, the evaluation of HBsAb is useful. A negative result for HBsAb should be followed by checking for the HBV-DNA level. For patients with occult HBV infection (with detectable DNA), pre-emptive therapy should be given, and periodic monitoring of ALT levels and viral loads be checked as for those with positive HBsAg. Among patients with resolved HBV infection or those with positive HBsAb, the incidence of HBV reactivation will be low or absent, but careful monitoring of ALT levels will still be needed, particularly in HBV endemic areas.

{kind=link}
{kind=link}
{kind=link}
Algorithm for screening and prevention of hepatitis B virus (HBV) reactivation in rheumatoid arthritis (RA) patients scheduled for anti-tumour necrosis factor alpha (TNFα) therapy (Rx) based on the current treatment guidelines and the results of this study and previous reports. HBcAb, antibody against HBV core antigen; HBeAb, antibody against HBV envelope antigen; HBeAg, HBV envelope antigen; HBsAb, antibody against HBV surface antigen; HBsAg, HBV surface antigen.
Although the results of our study provide some important evidence concerning appropriate screening and antiviral prophylaxis, there are some limitations of our study that need to be addressed. The present study was a retrospective cohort study. In addition, the sample size was small, and the duration of anti-TNFα treatment as well as follow-up in the enrolled subjects was short. The long-term safety of TNFα inhibitors in RA patients with HBV infection remains to be confirmed. Future prospective investigation of the incidence and risk factors of HBV reactivation in a large number of subjects, and the occurrence of lamivudine resistance due to HBV mutations, is needed.
In conclusion, the results of our study and recent reports showed that anti-TNFα therapy can induce HBV reactivation in both HBsAg-positive patients and HBsAg-negative patients with detectable HBV DNA or with a HBcAb-positive/HBsAb-negative status, whereas it can be safely used without increasing HBV reactivation in HBV-resolved patients with positive HBsAb. More awareness is needed regarding the potential risk of HBV reactivation in HBsAg-negative patients undergoing anti-TNFα therapy. Antiviral prophylactic therapy can effectively reduce the risk of HBV reactivation in RA patients undergoing anti-TNFα therapy.
References
Footnotes
See Editorial, pg 1701
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Clinical Research Ethics Committee of Taichung Veterans General Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.