Article Text

Abstract
Objectives To evaluate efficacy and safety of immediate switch from upadacitinib to adalimumab, or vice versa, in patients with rheumatoid arthritis with non-response or incomplete-response to the initial therapy.
Methods SELECT-COMPARE randomised patients to upadacitinib 15 mg once daily (n=651), placebo (n=651) or adalimumab 40 mg every other week (n=327). A treat-to-target study design was implemented, with blinded rescue occurring prior to week 26 for patients who did not achieve at least 20% improvement in both tender and swollen joint counts (‘non-responders’) and at week 26 based on Clinical Disease Activity Index (CDAI) >10 (‘incomplete-responders’) without washout.
Results A total of 39% (252/651) and 49% (159/327) of patients originally randomised to upadacitinib and adalimumab were rescued to the alternate therapy. In both switch groups (adalimumab to upadacitinib and vice versa) and in non-responders and incomplete-responders, improvements in disease activity were observed at 3 and 6 months following rescue. CDAI low disease activity was achieved by 36% and 47% of non-responders and 45% and 58% of incomplete-responders switched to adalimumab and upadacitinib, respectively, 6 months following switch. Overall, approximately 5% of rescued patients experienced worsening in disease activity at 6 months postswitch. The frequency of adverse events was similar between switch groups.
Conclusions These observations support a treat-to-target strategy, in which patients who fail to respond initially (or do not achieve sufficient response) are switched to a therapy with an alternate mechanism of action and experience improved outcomes. No new safety findings were observed despite immediate switch without washout.
- adalimumab
- arthritis
- rheumatoid
- tumor necrosis factor inhibitors
- therapeutics
- outcome assessment
- health care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- adalimumab
- arthritis
- rheumatoid
- tumor necrosis factor inhibitors
- therapeutics
- outcome assessment
- health care
Key messages
What is already known about this subject?
In patients with rheumatoid arthritis, a treat-to-target strategy is recommended, in which therapy is optimised every 3–6 months until remission, or low disease activity, is achieved. Recent treatment recommendations suggest the addition of a biological or targeted-synthetic disease-modifying antirheumatic drug in patients who do not achieve treatment goals, and switches between mechanisms of action occur commonly in clinical practice.
The SELECT-COMPARE study followed treat-to-target principles. Patients were blindly switched from upadacitinib, a Janus kinase (JAK) inhibitor, to adalimumab, a tumour necrosis factor (TNF) inhibitor, and vice versa following insufficient response to the initial therapy. Previously reported high-level efficacy data from this study showed that patients switched to either agent experienced improved response following switch.
What does this study add?
This observation from SELECT-COMPARE provides clinically relevant and detailed switch efficacy data in the subgroups of patients who switched due to initial non-response or incomplete-response. Following a blinded switch in mechanism of action, more patients were able to achieve treatment goals of remission and low disease activity, in both the non-responder and incomplete-responder groups. This study also reports minimal risk of flare following a switch in treatment.
Additionally, not previously reported, unique and important details on the safety of an immediate switch from a JAK inhibitor to a TNF inhibitor are also provided. This study revealed no new safety signals despite an immediate switch in mechanism of action without washout.
Key messages
How might this impact on clinical practice or future developments?
Findings here indicate that an immediate switch in mechanism of action (from a JAK inhibitor to a TNF inhibitor and vice versa) following treat-to-target principles is feasible with minimal risk of flare regardless of whether patients are switched due to non-response or incomplete-response without an increase in clinically meaningful adverse events.
Introduction
It is recommended that the rheumatoid arthritis (RA) treatment paradigm use a treat-to-target strategy in which therapy is optimised every 3–6 months until clinical remission, or at minimum, low disease activity (LDA) is achieved.1–5 For patients who do not achieve these goals with conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), both American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR) guidelines suggest the addition of a biological DMARD (bDMARD) or a targeted synthetic DMARD (tsDMARD).2 3 If patients continue to exhibit unacceptable disease activity, a switch to a different bDMARD, or to a tsDMARD, is recommended. Although therapeutic options continue to increase, many patients with RA do not achieve stringent treatment goals. Therefore, data on the effectiveness and safety of switching between different mechanisms of action (MoAs) have become increasingly important. Results from controlled trials suggest that patients with insufficient response to a bDMARD may respond to a Janus kinase inhibitor (JAKi).6–9 In contrast, there is limited evidence regarding the efficacy and safety of switching patients to a tumour necrosis factor inhibitor (TNFi) following insufficient response to a JAKi.10
Upadacitinib, an oral JAKi, has been studied across various patient populations in RA, including methotrexate (MTX)-inadequate responders in SELECT-COMPARE.11–13 The most recent EULAR recommendations for RA treatment address the shifting therapeutic paradigm.3 This study employed a unique rescue strategy, permitting blinded rescue from upadacitinib to adalimumab, and vice versa, in the subgroup of patients who did not achieve treatment targets with their initial therapy. Although preliminary data on an immediate switch from either a TNFi to a JAKi or vice versa have been reported,10 11 the safety of an immediate switch and the efficacy of a switch from a JAKi to a TNFi in patients who either do not have an initial response or experience an insufficient response have not been fully described. The present observational analysis describes the efficacy and safety results of the application of this treat-to-target strategy and expands significantly on the limited results reported previously.10
Patients and methods
Patients
Eligibility criteria have been described previously.11 Briefly, adult patients with RA with ≥6 swollen and ≥6 tender joints, a high-sensitivity C-reactive protein (hsCRP) level ≥5 mg/L, and evidence of erosive disease and/or seropositivity for either rheumatoid factor or anticyclic citrullinated peptide antibodies were enrolled.
Study design
Patients were randomised to double-blinded upadacitinib 15 mg once daily, placebo or adalimumab 40 mg every other week with background MTX (online supplemental figure S1). Blinded rescue (upadacitinib to adalimumab, adalimumab to upadacitinib and placebo to upadacitinib) occurred prior to week 26 (weeks 14, 18 or 22) for patients who did not achieve ≥20% improvement from baseline in both tender and swollen joint count based on 68 joints (TJC68) or 66 joints (SJC66) (defined as ‘non-responders’ (NR)). An additional blinded switch occurred at week 26 for patients who did not achieve Clinical Disease Activity Index (CDAI) LDA (≤10; defined as ‘incomplete-responders’ (IR)). Rescue was immediate and without washout according to the following schedule: (1) switching to upadacitinib: last dose of adalimumab was administered 2 weeks prior to starting upadacitinib; (2) switching to adalimumab: adalimumab was injected 1 day after the last dose of upadacitinib. Each patient could only be switched once. Further details on the blinded rescue are provided in the online supplemental text. The observations of efficacy and safety of patients switching between upadacitinib and adalimumab (and vice versa) are presented here.
Supplemental material
The study was conducted in accordance with the International Conference on Harmonization guidelines, applicable regulations and the Declaration of Helsinki. All patients provided written informed consent.
Assessments
Efficacy was evaluated up to 6 months (±2 weeks) postswitch using validated outcome measures including ACR response criteria (ACR20/50/70 (improvement of ≥20%, 50% and 70% in ACR criteria)); CDAI LDA (≤10) and remission (≤2.8); 28-joint Disease Activity Score based on C-reactive protein (DAS28(CRP))≤3.2 and<2.6 and change from baseline in Health Assessment Questionnaire-Disability Index (HAQ-DI), patient assessment of pain (0–100 mm visual analogue scale), TJC68, SJC66, Patient’s Global Assessment of Disease Activity (PtGA), Physician’s Global Disease Activity (PhGA) and hsCRP. Response criteria and change from baseline were evaluated as change from original baseline value at randomisation.
Disease worsening after switch was determined based on DAS28(CRP) increase >0.6 or >1.2 from rescue, evaluated at 3 and 6 months following rescue.14
Treatment-emergent adverse events (TEAEs) were evaluated 0–3 months postswitch to assess the safety of an immediate switch and, separately, 4–6 months following switch.10 11 To better understand the safety preswitch and postswitch, TEAEs were evaluated for the same patients both before and after switch. In this analysis, a matching follow-up period was used to ensure a consistent evaluation across patients who were rescued at different time points. Finally, TEAEs were also evaluated in patients who switched and those who remained on continuous therapy using matching time periods.
Statistical analysis
For these observations, descriptive statistics are summarised for the NR and IR treatment groups following switch. As rescue groups were not randomised for this subset of patients, no direct statistical comparison was made between groups. The study was not designed to compare efficacy or safety between the switch treatment arms. Data are reported as observed with no imputation for missing data. Adverse event data are reported as n (%) with 95% CIs.
Sensitivity analyses were conducted to exclude the few patients in the IR group who were rescued at week 26 despite the achievement of CDAI LDA. Spearman correlation and a univariate logistic regression analysis were used to assess the association between baseline disease characteristics and ‘double non-response’, defined as patients who required rescue (at any time point) and still failed to achieve CDAI LDA at both 3 and 6 months postswitch.
Results
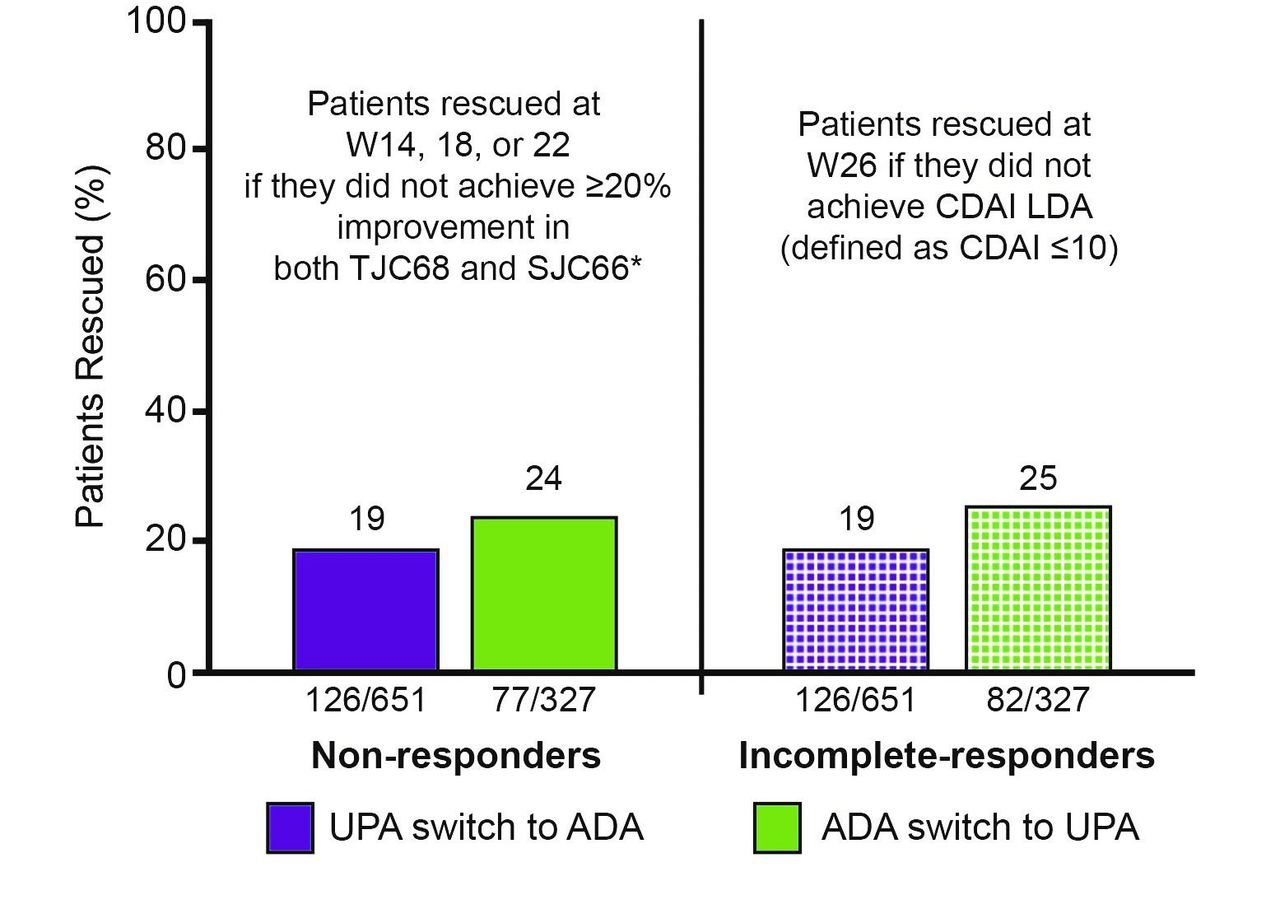
Of the 651 patients randomised to upadacitinib and 327 patients randomised to adalimumab, 38.7% (252/651) and 48.6% (159/327), respectively, were rescued to the alternate therapy prior to week 26 due to NR or at week 26 due to IR (figure 1). Across both treatment groups, roughly equal proportions of patients were rescued due to NR and IR.

Proportion of patients rescued. *12% (78/651), 5% (29/651) and 3% (19/651) of patients were rescued from UPA to ADA at W14, W18 and W22, respectively. 17% (56/327), 4% (14/327) and 2% (7/327) were rescued from ADA to UPA at W14, W18 and W22, respectively. ADA, adalimumab; CDAI, Clinical Disease Activity Index; LDA, low disease activity; SJC66, swollen joint count-66 joints; TJC68, tender joint count-68 joints; UPA, upadacitinib; W, week.
Baseline demographics were generally similar between patients who were switched and the overall study population.11 There was improvement in disease activity assessments from baseline to the time of switch, and the improvements were greater in the IR patients compared with patients in the NR group (online supplemental table S1).
Non-responders
A switch in MoA had a beneficial effect on clinical responses in both groups. Six months after rescue, 59.3% (67/113)/25.9% (29/112)/12.3% (14/114) of patients achieved ACR20/50/70 responses following rescue to adalimumab and 74.6% (53/71)/49.3% (34/69)/23.6% (17/72) following rescue to upadacitinib (figure 2). CDAI LDA and remission were achieved by 36.0% (41/114) and 5.3% (6/114) of patients after rescue to adalimumab and 47.1% (33/70) and 14.3% (10/70) of patients after rescue to upadacitinib (figure 3). Six months after rescue to adalimumab, DAS28(CRP) ≤3.2 and DAS28(CRP) <2.6 were achieved by 34.9% (38/109) and 19.3% (21/109) of patients; 54.3% (38/70) and 31.4% (22/70) of patients achieved DAS28(CRP) ≤3.2 and DAS28(CRP) <2.6 at 6 months after rescue to upadacitinib (figure 3). There were also improvements from baseline in function (HAQ-DI), joint counts (TJC68/SJC66), patient and physician global assessments (PtGA, PhGA, pain) and hsCRP following rescue to the alternate agent (online supplemental figure S2).
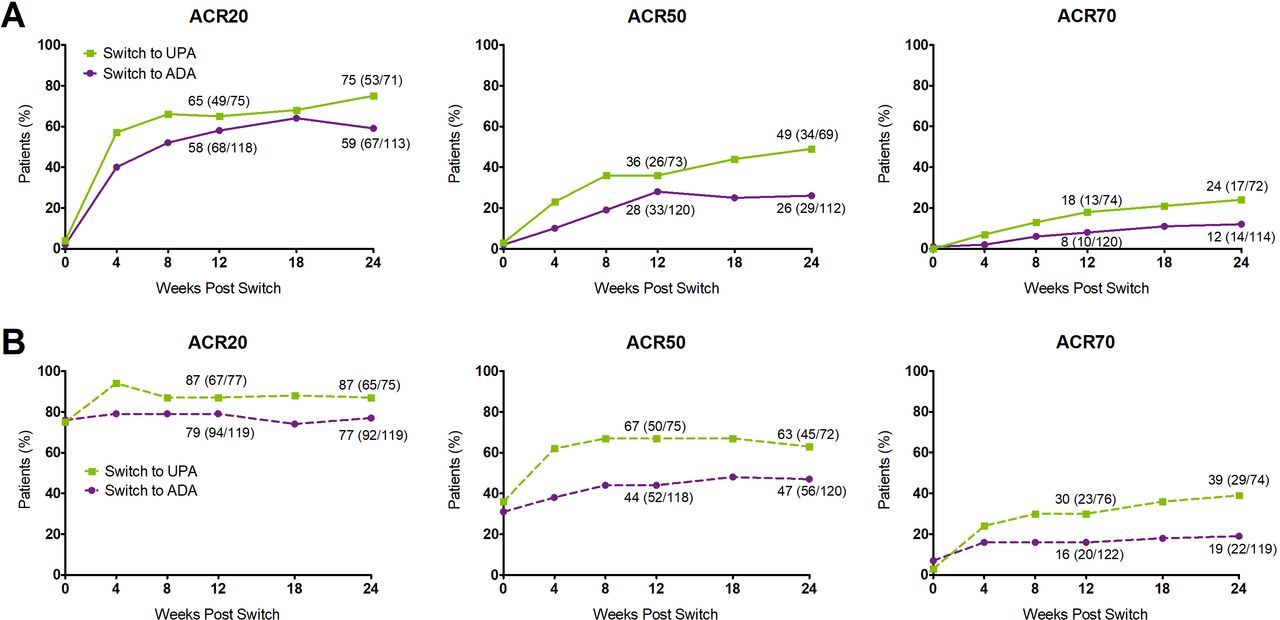
Percentage of non-responders (A) and incomplete-responders (B) achieving ACR20/50/70 at 3 and 6 months postswitch. All data points are provided in online supplemental table S6. ACR20/50/70, improvement of at least 20%, 50% and 70% in American College of Rheumatology criteria from baseline; ADA, adalimumab; mo, month; UPA, upadacitinib.
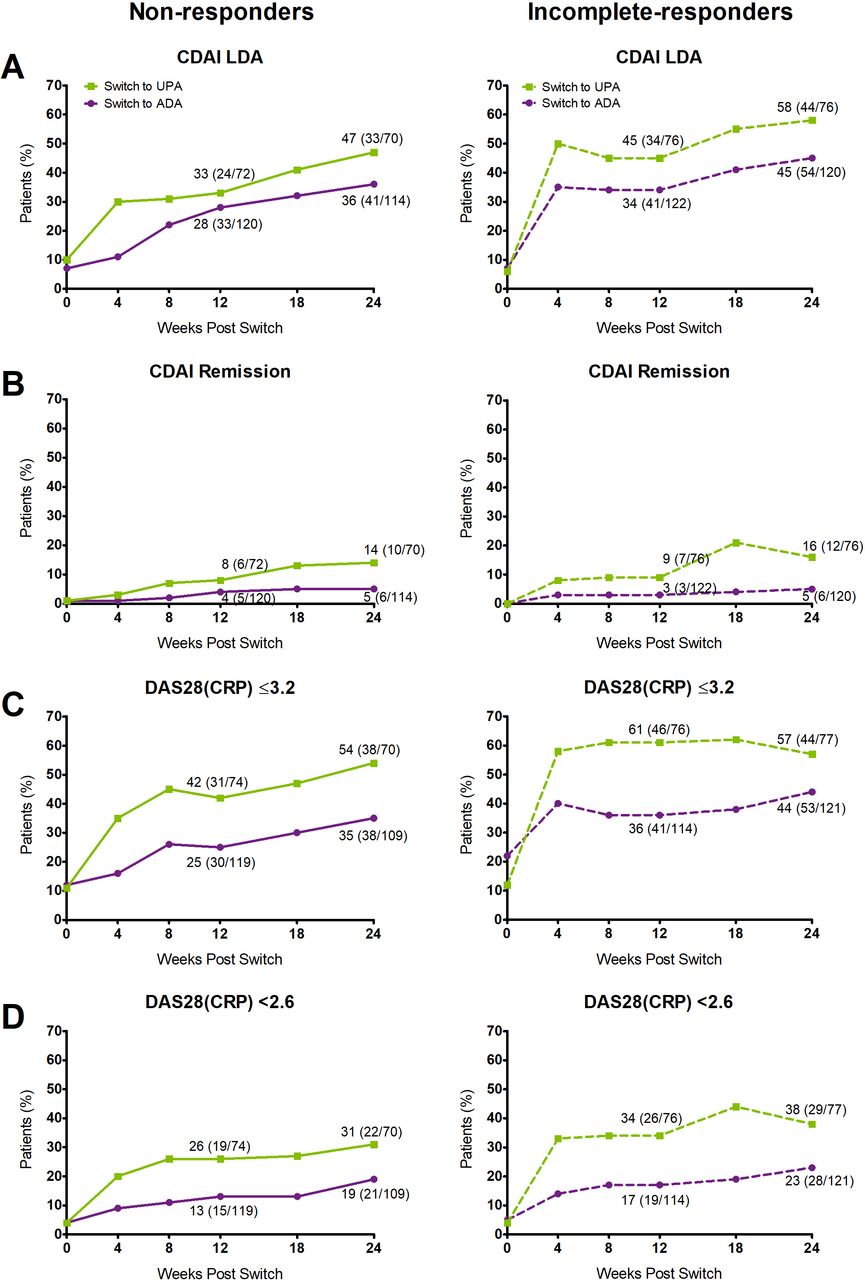
Percentage of non-responders and incomplete-responders achieving CDAI LDA (A) and remission (B), and DAS28(CRP)≤3.2 (C) and <2.6 (D) at 3 and 6 months postswitch. All data points are provided in online supplemental table S7. ADA, adalimumab; CDAI, Clinical Disease Activity Index; DAS28(CRP), 28-joint Disease Activity Score based on C-reactive protein; LDA, low disease activity; UPA, upadacitinib.
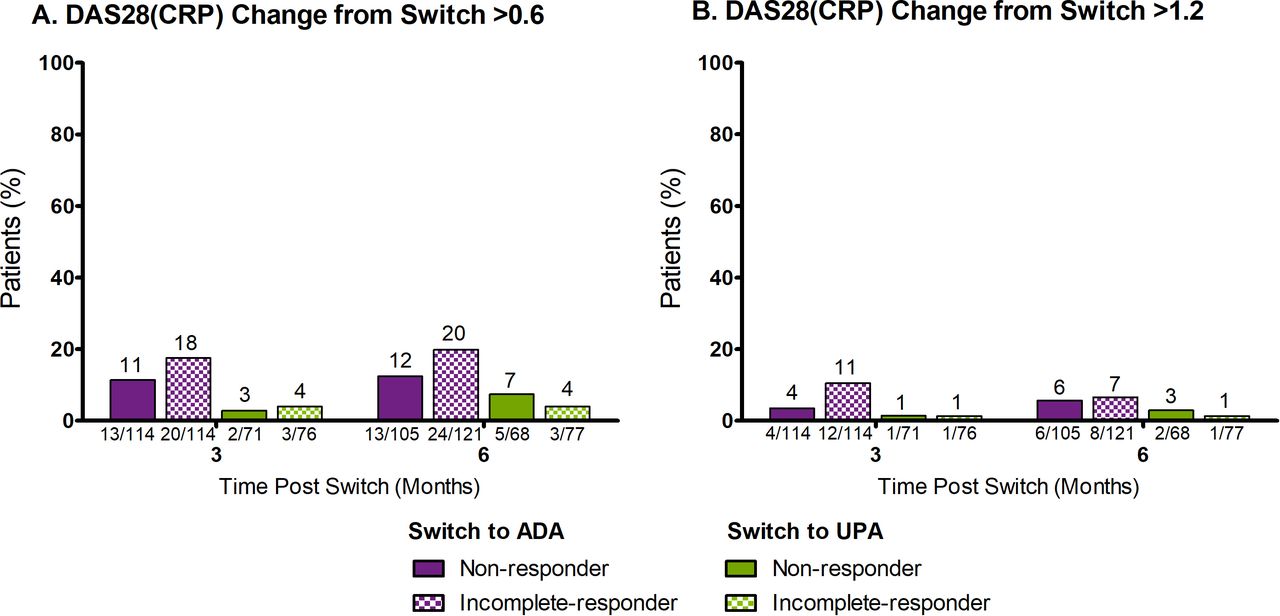
Some NR experienced increases in disease activity following rescue: at 6 months postrescue, 12.4% (13/105) and 7.4% (5/68) of those switched to adalimumab and upadacitinib, respectively, had an increase in DAS28(CRP) >0.6. Eight (4.6%; 8/173) of all NR (6 rescued to adalimumab and 2 rescued to upadacitinib) experienced a worsening in DAS28(CRP) >1.2 (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of non-responders and incomplete-responders with DAS28(CRP) change from switch >0.6 (A) and >1.2 (B). ADA, adalimumab; DAS28(CRP), 28-joint Disease Activity Score based on C-reactive protein; UPA, upadacitinib.
Incomplete-responders
Six months after switch to adalimumab, 77.3% (92/119)/46.7% (56/120)/18.5% (22/119) of IR achieved ACR20/50/70 responses; of those switched to upadacitinib, 86.7% (65/75)/62.5% (45/72)/39.2% (29/74) achieved ACR20/50/70 at 6 months following switch (figure 2). As expected, given that incomplete-responders by definition had at least 20% improvement in TJC and SJC at the rescue visits prior to week 26, most had achieved an ACR20 response at switch. At 6 months following switch, CDAI LDA and remission were achieved by 45.0% (54/120) and 5.0% (6/120) of patients switched to adalimumab and 57.9% (44/76) and 15.8% (12/76) of patients switched to upadacitinib (figure 3). Among patients switched to adalimumab, 43.8% (53/121) and 23.1% (28/121) achieved DAS28(CRP) ≤3.2 and DAS28(CRP) <2.6 at 6 months postswitch; 57.1% (44/77) and 37.7% (29/77) of patients switched to upadacitinib achieved DAS28(CRP) ≤3.2 and<2.6 (figure 3). In addition, when switched to the alternate therapy, an improvement from baseline was observed in HAQ-DI, TJC68/SJC66, PtGA, PhGA, pain and hsCRP (online supplemental figure S2).
Following switch, some IR experienced a worsening in disease. At 6 months postrescue, 19.8% (24/121) and 3.9% (3/77) of patients switched to adalimumab and upadacitinib, respectively, experienced an increase in DAS28(CRP) >0.6. (figure 4). At the same time point, 9 (4.5%; 9/198) of all IR (8 switched to adalimumab and 1 switched to upadacitinib) experienced a clinically relevant worsening of DAS28(CRP) >1.2.14
In the IR group, 7.1% (9/126) of patients switched to adalimumab and 6.1% (5/82) of patients switched to upadacitinib were switched despite achievement of CDAI LDA. Results were unchanged when these patients were excluded from the analyses (online supplemental table S2).
Double non-response
Correlation and logistic regression analyses were conducted to evaluate potential factors associated with double non-response. In total, 210 patients (21.2% (138/651) and 22.0% (72/327) of patients initially randomised to upadacitinib or adalimumab, respectively) were double non-responders. Both analyses showed a weak association between higher disease activity and functional impairment at baseline and double non-response (online supplemental tables S3 and S4). No other discriminators were observed.
Safety
Following immediate switch in treatment without washout, the proportion of patients experiencing any TEAE was similar regardless of whether patients switched to adalimumab or upadacitinib (table 1). The frequency of infections, including serious infections, and herpes zoster was also similar between switch groups. No active tuberculosis, non-melanoma skin cancer, adjudicated major adverse cardiovascular event, or deaths were reported. Additionally, no differences in the proportion of TEAEs were observed when the same patient groups were evaluated prior to and following rescue (table 2). Similarly, no meaningful differences in TEAEs were observed in patients who switched therapy compared with those who remained on continuous therapy (online supplemental table S5).
Number and percentage of patients experiencing TEAEs 0–3 months and 4–6 months post-treatment switch
Number and percentage of patients experiencing TEAEs in patients prior to and following treatment switch
Discussion
Recent advances in drug development have led to approval of multiple therapeutic options, including oral therapies, for RA. Recommendations from professional societies have noted the importance of the availability of a variety of MoAs and discuss switching MoAs in the event of insufficient response.2 3 While there are multiple reports of switching to an alternative agent following inadequate response to a TNFi, there are no other data on an immediate switch in MoA following insufficient response to a JAKi. This poses a challenge for clinicians making evidence-based treatment decisions. The unique trial design of SELECT-COMPARE, the first fully blinded study to report switch data between a JAKi and a TNFi, permitted assessment of these questions in a setting with defined criteria and provides the first data showing clinical outcomes in patients who failed to respond to a JAKi and subsequently switched to a TNFi. In contrast to another JAKi trial where patients were not rescued from the JAKi to adalimumab, SELECT-COMPARE provides data with a rescue in both directions based on objective and predefined criteria.15 Ultimately, the observations from SELECT-COMPARE provide valuable outcomes for providers using treat-to-target principles for their patients who continue to manifest active disease despite treatment with a TNFi and highlights the importance of diverse MoAs.
In the present analysis, many patients with initial NR or IR to either upadacitinib or adalimumab experienced meaningful improvement in clinical and functional outcomes following rescue to the alternate therapy, suggesting that a switch to either MoA may be beneficial for patients with RA not previously meeting treatment goals. Clinically relevant improvements from baseline across different disease measures were consistently seen in both groups, although numerically better improvement was generally observed in IR versus NR patients. The data observed for patients switching from adalimumab to upadacitinib were in line with previously reported data from the SELECT-BEYOND trial, which evaluated upadacitinib in bDMARD-inadequate responder patients.6 Similarly, the outcomes observed for patients switching from upadacitinib to adalimumab were consistent with those reported in the EXXELERATE study where patients were switched to adalimumab following inadequate response to an alternate TNFi.16 Studies involving bDMARD-inadequate responder patients, such as SELECT-BEYOND, used prolonged intervals between the stop of biological therapy and initiation of JAKi for perceived safety concerns; the observations in SELECT-COMPARE provide direct switch data with no washout period suggesting that an immediate switch did not lead to increased safety concerns. The safety of immediate switch between adalimumab and upadacitinib seen here is in line with prior safety experience of an immediate switch between two TNFis seen in EXXELERATE.16
As with all therapies, there was a proportion of patients who either had little if any initial response or who improved but failed to achieve disease targets. A potential concern with switching therapies in the latter group is whether their disease will worsen on a change in therapy. In the present analysis, relatively few patients experienced a clinically significant worsening in disease following switch. Six months following rescue for either incomplete-response or non-response, only approximately 5% of patients rescued to either therapy (adalimumab to upadacitinib or vice versa) experienced a worsening in disease as defined by an increase in DAS28(CRP) >1.2. In SELECT-COMPARE, this flare risk is largely outweighed by the observed efficacy outcomes. Approximately one-half of patients who had a clinically relevant response with a significant decrease in CDAI, but did not achieve CDAI LDA, were able to achieve this stringent endpoint with a switch in MoA. These outcomes support a treat-to-target strategy, and address a common question asked in clinical practice regarding the likelihood of a patient achieving treatment goals with a switch in therapy versus the chances of them experiencing disease worsening. The current analysis would suggest that a switch is much more likely to be successful than the risk of a flare.
There were patients who did not respond to either therapy. Based on exploratory analyses examining baseline demographics, predictors for double non-response could not be identified; additional research is needed to elucidate predictors of patients who will fail to respond to either therapy.
Although it may appear that the proportion of patients rescued in this study (in total, 252 patients (39%) rescued to adalimumab and 159 patients (49%) rescued to upadacitinib) is greater than rescue rates observed in other trials, this was largely due to the unique rescue scheme used in SELECT-COMPARE. Treatment switch was permitted at four time points and included rescue based on the stringent metric of CDAI LDA at week 26. Other studies typically only permitted rescue at a single time point.17–19 In these studies, the rates of rescue are consistent with those described at week 14 for SELECT-COMPARE.
This analysis also provides clinically relevant, blinded data on the safety of an immediate switch in therapy from a biological to a JAKi without washout. Given a mean terminal half-life of approximately 2 weeks for adalimumab,20 21 pharmacodynamic (PD) effects might persist to a certain degree after discontinuation of adalimumab until complete washout within several weeks. On the other hand, upadacitinib has a shorter half-life of 9–14 hours and immediate PD effects (eg, those based on IL-6 signalling) are expected to disappear within a day.22 Complete washout of upadacitinib is expected within a few days; however, delayed PD effect may last beyond this. While there is potential for differences in the overlap of inhibition between the two switch arms, overall efficacy appears consistent through 6 months with no fluctuations in response. Clinically, consideration for half-life and PD effects may need to be given for individual patients. Importantly, in terms of safety, although limited by sample size, based on available data from over 400 patients, no additional safety concerns were observed in either treatment group (upadacitinib to adalimumab and vice versa) despite this immediate switch. In particular, and perhaps most pertinent considering overlapping PD effects, no differences in frequency of infections were observed between treatment groups at both 0–3 and 4–6 months postrescue. Overall consistent findings were observed in the adverse event profile of patients evaluated prior to and following switch.
This study is not without limitations. Due to the observational nature of this analysis, both the safety and efficacy evaluations are ultimately limited by the number of patients who met rescue criteria; as such, the present analysis was not designed or powered for statistical comparisons between switch groups (either the two switch arms, or NR versus IR) and the results should be interpreted as observational. Additionally, this analysis from a clinical trial population may not be generalisable to all patients in clinical practice; further real-world studies are needed to confirm these results. While the study used aspects of a treat-to-target strategy, the rescue was based on predefined criteria at specified timepoints, and did not allow providers the opportunity to adjust therapy more freely in accordance with their clinical judgement, as may be more typical of a true treat-to-target strategy. Patients were not rerandomised at rescue but were switched to the alternate treatment in a double-blind fashion using an interactive response technology system.
In summary, SELECT-COMPARE used a treat-to-target strategy with blinded rescue and provides the first data to suggest patients switching from a JAKi to a TNFi may experience an improved response following rescue. Patients with initial NR or IR to either upadacitinib 15 mg once daily or adalimumab 40 mg every other week, both in combination with MTX, showed benefit in both clinical and functional outcomes when switched to the alternate therapy. Numerous patients who had a significant clinical response but did not reach CDAI LDA were able to reach this target with a switch in MoA. Despite an immediate switch in MoA, without washout, no new safety signals were observed in either treatment group.23
Acknowledgments
AbbVie, Inc was the study sponsor, contributed to study design, data collection, analysis and interpretation and to writing, reviewing and approval of final version. No honoraria or payments were made for authorship. The authors thank Mark C. Genovese (Stanford University) for contributions to the manuscript content. Medical writing support was provided by Jamie Urbanik, PharmD, of AbbVie, Inc.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Josef S Smolen
Contributors RMF, YL and I-HS were involved in the design of the study. RMF, RB, SH, GTDT, FEVdB, CZ and LB were involved in the acquisition of data. All authors were involved in the analysis and interpretation of the data, drafting the manuscript and revising it for critically important intellectual content and reviewing and approving the final version of the manuscript.
Funding This study (NCT02629159) was funded by AbbVie, Inc.
Competing interests RMF has received grant/research support from AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, EMD-Serono, Genentech, Gilead, Janssen, Novartis, Pfizer Inc, Regeneron, Roche, Sanofi-Aventis, UCB and Viela and is a consultant for AbbVie, Amgen, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Janssen, Novartis, Pfizer Inc, Sanofi-Aventis and UCB. RB has received grants/research support from AbbVie, MSD and Roche and had consultation fees/participation in company-sponsored speaker’s bureau from AbbVie, Bristol-Myers Squibb, Eli Lilly, Janssen, Pfizer, and Roche. SH has received research grants and consultancy fees from AbbVie, Bristol-Myers Squibb, Eli Lilly, Janssen, Novartis, Pfizer and UCB. GTDT has received a research grant from AbbVie and consulting fees from Amgen. FEVdB has received speaker and/or consultancy fees from AbbVie, Bristol-Myers Squibb, Celgene, Eli Lilly, Galapagos, Janssen, Merck, Novartis, Pfizer and UCB. CZ has received grants/research support from AbbVie, Amgen, Eli Lilly, GlaxoSmithKline, Novartis, Pfizer and Sanofi. LB has received grant/research support from AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Eli Lilly, Gilead, Janssen, Novartis, Pfizer Inc, Sanofi-Aventis and UCB and is a consultant for AbbVie, Amgen, Bristol-Myers Squibb, Eli Lilly, Gilead, Janssen, Novartis, Pfizer Inc, Sanofi-Aventis and UCB. JE, YL, YS, RD and I-HS are full-time employees of AbbVie and may hold AbbVie stock or stock options.
Patient consent for publication Not required.
Ethics approval Study-related documents were approved by institutional ethics committees and review boards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. AbbVie is committed to responsible data sharing regarding the clinical trials we sponsor. This includes access to anonymised, individual and trial-level data (analysis datasets) as well as other information (eg, protocols and Clinical Study Reports), as long as the trials are not part of an ongoing or planned regulatory submission. This includes requests for clinical trial data for unlicensed products and indications. This clinical trial data can be requested by any qualified researchers who engage in rigorous, independent scientific research and will be provided following review and approval of a research proposal and Statistical Analysis Plan (SAP) and execution of a Data Sharing Agreement (DSA). Data requests can be submitted at any time and the data will be accessible for 12 months, with possible extensions considered. For more information on the process, or to submit a request, visit the following link: https://www.abbvie.com/our-science/clinical-trials/clinical-trials-data-and-information-sharing/data-and-information-sharing-with-qualified-researchers.html.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.