Article Text

Statistics from Altmetric.com
Tumour necrosis factor receptor-associated periodic syndrome (TRAPS) is a dominantly inherited autoinflammatory disease characterised by recurrent episodes of fever, arthritis and serositis. In adulthood, inflammation often becomes persistent1 and AA amyloidosis may occur. Evidence of dysregulated secretion of proinflammatory cytokines, particularly interleukin 1 (IL-1) beta, in autoinflammatory diseases recently supported anakinra, the recombinant IL-1 receptor antagonist, as a target therapy for most of these conditions.2 3 In TRAPS, response to anakinra was reported in two case reports and in one prospective trial, in which five patients were treated for a mean duration of 11.4 months.4,–,6 However, longer follow-up and additional observations are warranted. We report the long-term efficacy and safety of anakinra in seven TRAPS patients with and without AA amyloidosis.
We reviewed the medical records of seven patients genetically diagnosed with TRAPS (four men, aged 21–53 years, median disease duration 33 years, range 13–48), who started anakinra treatment (100 mg/day subcutaneously) between October 2006 and September 2009 (table 1). In three patients the disease was persistent, with incomplete control of symptoms and inflammatory markers despite daily prednisone. Two patients had biopsy-confirmed renal amyloidosis and had previously been treated with etanercept. Unfortunately, one relapsed after 1 year (C43Y) and the other (C52Y) developed a skin reaction, requiring discontinuation of etanercept after 4 weeks.
Characteristics of patients at start of anakinra treatment
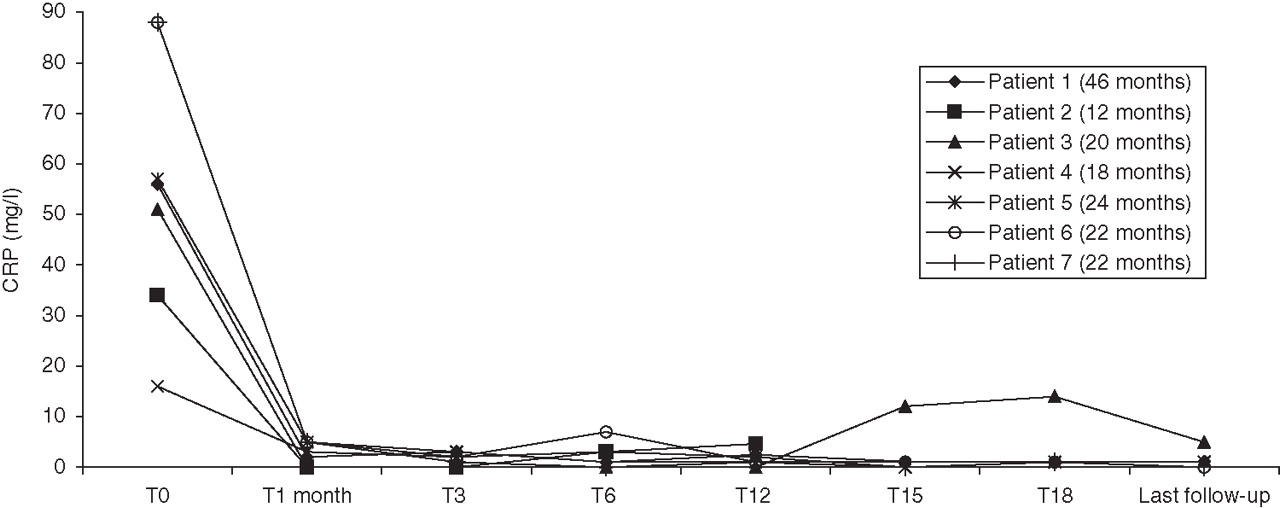
Anakinra induced complete resolution of symptoms with normalisation of C-reactive protein (CRP) and serum amyloid A in all patients within 1 month (figure 1). Three patients were on prednisone at the start of anakinra. Prednisone was discontinued in two patients and maintained (5 mg/day) in the third (C43R) to control injection site reactions. At last follow-up, (mean treatment duration 23 months, range 12–46), complete response was maintained in six patients, including patient C52Y in whom proteinuria (g/day) completely regressed (7.3→1.8 (3 months)→0.5 (6 months)→0.15 (1 year)). In the remaining patient (C43Y) two abdominal attacks occurred after 15 months and maintenance prednisone (10 mg/day) was required. Since then, he has had no additional bouts and CRP was normal at last follow-up. Renal failure and proteinuria have stabilised after starting anakinra.
{kind=link}
Changes in concentrations of C-reactive protein (CRP) in seven tumour necrosis factor receptor-associated periodic syndrome patients treated with anakinra 100 mg/day subcutaneously. Treatment duration (in months) for each patient is reported in the insert box.
Anakinra was well tolerated. The expected side-effects according to large studies in rheumatoid arthritis are injection site reactions and respiratory and urinary infections.7 In our series only two patients (no 2 C52Y and no 6 T50M) experienced pharyngitis and bronchopneumonia, respectively. Mild injection site reactions occurred in five patients but resolved spontaneously in three over a few weeks. These reactions were treated with the anti-histamine loratadine in one patient and with low-dose prednisone in another.
In our experience, anakinra is safe and effective in TRAPS, reducing disability and improving everyday life. Skin reactions are frequent but manageable. We support anakinra as first-line treatment for patients with TRAPS who require high-dose glucocorticoids, also in light of the variable efficacy of etanercept that is increasingly reported.8 9 Long-lasting drugs targeting IL-1, such as canakinumab and rilonacept, have proved to be highly effective and tolerated in cryopyrinopathies,3 10 overcoming the need for daily injections. Trials to evaluate their efficacy in TRAPS are warranted.
Footnotes
-
Patient consent Obtained.
-
Funding This work was supported by the European Community's Seventh Framework Programme (FP7/2007-2013) under grant agreement no 200923, Eurotraps project.
-
Competing interest None.
-
Ethical approval The Institutional review Board of the Fondazione Istituto di Ricovero e Cura a Carattere Scientifico Policlinico San Matteo, Pavia, approved the storage and use of biological samples and the use of patients' clinical data for research purposes.
-
Provenance and peer review Not commissioned; externally peer reviewed.