Article Text

Statistics from Altmetric.com
Rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) are multifactorial autoimmune diseases that originate from the patient’s excessive immune and inflammatory response to a pathogenic agent (that is, an infective antigen).1
The pathophysiological mechanisms are activated after the combination of several predisposing factors, which include the relations between histocompatibility epitopes and epitopes of the pathogenic antigen, the altered status of the stress response system (hypothalamic-pituitary-adrenocortical axis = HPA) and the gonadal hormone pattern (hypothalamic-pituitary-gonadal axis = HPG), with oestrogens principally implicated as enhancers of the immune response, and androgens and progesterone as natural suppressors (fig1).2-8

Genetic, infectious, and dietary factors, as well as gonadal/adreanal steroid hormones, play a predisposing part in autoimmune diseases such as RA and SLE. Therefore, the involvement of the hypothalamus-pituitary-adrenal (HPA = adrenal steroids) and -gonadal (HPG = gonadal steroids) axis is crucial and interferes with the immune system response.
An intricate balance with bidirectional interactions between soluble mediators, released by the neuroendocrine system (that is, steroid hormones and neuropeptides) and products of activated cells of the immune/inflammatory system (cytokines) maintains the homeostasis in presence of the immune/inflammatory stimulus.9-12
Cytokine patterns and sub-patterns in RA and SLE
Cytokine secretion seems fundamental in determining the duration and intensity of an immune response, and how steroid hormones (gonadal and adrenal steroids) influence autoimmunity may entail a further balance between Th1 and Th2 lymphocyte responses.13-15
Th1 lymphocytes produce mainly interleukin 2 (IL2) and interferon γ (IFNγ) and are primarly responsible for cell mediated immunity, while Th2 lymphocytes produce mainly IL4, IL5, IL13, and IL10, and are responsible for humoral immunity, supporting the activation of immunoglobulin secreting cells (fig 2).16 17

Role of Th1/Th2 cytokines in the regulation of cellular and humoral immunity. IL6, probably secreted by activated macrophages (Mφ) is able to polarise naive CD4+ T cells (Th0) to effector Th2 cells, by inducing the initial production of IL4 in CD4+ T cells. IL12 triggers the differentiation of Th1 cells. Th1 and Th2 cells are mutually inhibitory. RA and SLE are Th1 and Th2 driven diseases, respectively.
IL6, probably secreted by activated antigen presenting cells (macrophages), is able to polarise naive CD4+ T cells to effector Th2 cells by inducing the initial production of IL4 in CD4+ T cells (fig2).18 In contrast, IL12 triggers the differentiation of Th1 cells. Th1 and Th2 cells are mutually inhibitory (fig 2).
Recent data show different patterns of cytokine production (Th1 and Th2) between patients affected by RA and SLE.19 20 In particular, based on these differences, RA is considered to be “Th1-cytokine driven” disease, whereas SLE is considered to be “Th2-cytokine dependent” disease.21 22
Broad differences in the clinical presentation and progression of both RA and SLE, complicate both the early diagnosis and the identification of patients in need of differentiated treatment. In fact, distinct sub-patterns of cytokine secretion characterise new onset synovitis versus chronic RA.20
Patients with new onset synovitis, presented increased numbers of peripheral blood mononuclear cells (PBMC) secreting IL2 and IFNγ, while patients with chronic RA showed increased numbers of PBMC secreting IL6, IL10 and TNFα.20
Correlations between joint score and number of PBMC, suggested that the number of PBMC secreting IFNγ is most relevant in new onset synovitis, while the number of PBMC secreting IL6, IL10, and TNFα is of greater relevance in chronic RA. Similarly, different serum cytokine sub-patterns have been associated with different clinical manifestations in SLE patients.19
The serum concentrations of IL6 and IFNγ were found increased in patients with SLE associated with lymphadenopathy (LN) or nephrotic syndrome (NS). In contrast, the serum concentrations of TNFα were increased in SLE patients with associated thrombocytopenia (TP) and normal in association with LN, NS or central nervous system involvement. SLE patients with associated humoral immunodeficiency disorder such as hypogammaglobulinaemia showed higher values of serum IL6.19
Recently, a polymorphism within the IL10 gene promoter that is associated with high IL10 serum concentrations, has been described in SLE patients and has been suggested as playing a part in the development of certain clinical features in this disease.23
Therefore, abnormal production of various cytokines in SLE, might be an intrinsic defect of PBMC and of the immune system that may explain the variety of clinical manifestations of the disease.
In conclusion, all these observations suggest that distinct cytokine secretion abnormalities may have a paramount importance in the triggering and/or maintenance of the different pathophysiological mechanisms and clinical aspects characterising RA, SLE, and probably other autoimmune disorders.24
Clinical relations between steroid hormones and cytokine patterns in RA and SLE
There is agreement that, the ability to make more or less of the critical immunoregulatory molecules, such as the cytokines, may have a crucial effect in determining susceptibility to the autoimmune diseases and their progression.
Therefore, patients with SLE reportedly have an increase in the Th2 cytokines and in particular, an increased IL10:IFNγ ratio compared with controls.25 26
However, it is intriguing to note that the IL10–819*C polymorphism is in a DNA motif forming also a putative oestrogen receptor element.23 It does not seem coincidental that SLE is almost 10-times more frequent in fertile women than men, and that women taking oral contraceptives are more susceptible to SLE development or have higher risk of disease flare.27 28
This finding suggests that the combination of both inheriting a higher producer IL10 haplotype and high oestrogen serum concentrations, might together be considerd related predisposing factors, at least in female SLE patients.
More specifically, pregnancy and the postpartum period, seem to represent a paradigmatic example of how changes in steroid hormone concentrations influence the female immune/inflammatory response, critical immunoregulatory molecule concentrations (that is, cytokines), and consequently the expression of autoimmune diseases.
A differential neuroendocrine control during pregnacy and postpartum seems to influence the Th1/Th2-type cytokine balance.22
Animal studies seem to suggest that pregancy is associated with the cytokine polarisation towards a Th2-type profile, with early increases in several cytokines, followed, as pregancy progresses, by a decrease in both IL2 and IFNγ (Th-1type cytokines), and IL4 (Th-2 type cytokines) increase.29 The physiological increased concentrations of cortisol, progesterone, oestradiol, and testosterone, observed during the third trimester, seem involved in the Th2-type cytokine polarisation.
In addition, an increased synthesis of Th2-type cytokines, has been observed at the maternal–fetal interface.30
High concentrations of Th2-type cytokines (IL10) have also been reported in placental tissues at term, and IL10 concentrations that are evaluable in all the amniotic fluids are particularly increased during the third trimester.31
Therefore, the suppression of Th1-type cytokines, such as IFNγ (cellular immunity) seems essential for fetal survival.
As a consequence, it is suggested that autoimmune diseases such as SLE, caused predominantly by antibody mediated damage (Th2-type cytokines, humoral immunity) tend to develop or flare during pregnancy and can improve in the postpartum period.22 Conversely, “Th1-driven” diseases, such as RA, tend to improve during pregnancy because of the increase of anti-inflammatory Th2-type cytokines (IL10), but commonly flare up or develop initially in the postpartum period (decrease of IL10).
Glucocorticoids are known both to inhibit IL1, TNFα, IFNγ, and IL2 production and to stimulate IL10, IL4, and IL13 production, confirming that this adrenal steroid hormone may exert an anti-inflammatory/immunosuppressive modulation in pregnancy (table1).32 Furthermore, the stress related activation of the HPA axis in disease, which usually results in increased systemic and local concentrations of cortisol might contribute to a polarised Th2-type cytokine milieu.
Effects of gonadal and adrenal (cortisol and DHEA) steroid hormones on macrophage, Th1-type and Th2-type cytokine production
Progesterone increases IL4 production (Th2-type cytokine) by human T cells, while oestradiol increases TNFα (Th1-type cytokine) secretion by clones at physiological concentration. However, it inhibits TNFα secretion at higher or pharmacological concentrations (late pregnancy) and increases the human IL10 production by T cell clones resulting in increased humoral immunity (table 1).33 34
Recent studies, have shown that testosterone also induces the immune responses towards the Th2 phenotype in the experimental autoimmune encephalomyelitis (EAE), which is a model for the human demyelinating disease multiple sclerosis.35
In fact, T lymphocytes derived from the spleen of men, during the effector phase of adoptive EAE and from dihydrotestosterone implanted EAE women, produced significantly higher concentrations of IL10 than those from women and placebo, respectively (table 1). Testosterone replacement therapy has been to improve clinical and laboratory parameters in male RA patients.36
On the basis of these steroid driven mechanisms, new explanations for the different age related incidence and behaviour of both RA and SLE might be suggested, at least in female patients.
The gradual decline of cortisol and oestrogens, observed around menopause, might explain the high incidence of RA at that time, with mechanisms similar to those realised in the postpartum period. Converserly, the same hormonal changes might explain the high incidence of SLE observed during the fertile ages and the decline around menopause.37
By acting through similar mechanisms, the increased serum oestrogen concentrations obtained by current use of oral contraceptives may protect the RA patients, but tend to exacerbate the disease in SLE patients as seen in clinical practice.28 38
Increased concentrations of oestrogens, as obtained after ovulation induction therapy, have been recently described to induce a severe or fatal exacerbation of the disease in several women with SLE, the concomitant presence of antiphospholipid antibodies being considered a further risk factor.39 40
Androgen modulation of cytokines in RA and SLE
Adrenal and gonadal androgens are considered natural immunosuppressors.41
Dehydroepiandrosterone (DHEA) is the most abundant andrenal steroid with androgenic properties and is present in about similar concentrations in both sexes. DHEA sulphate (DHEAS) is inactive and converted peripherally to DHEA, which exerts biological activity.
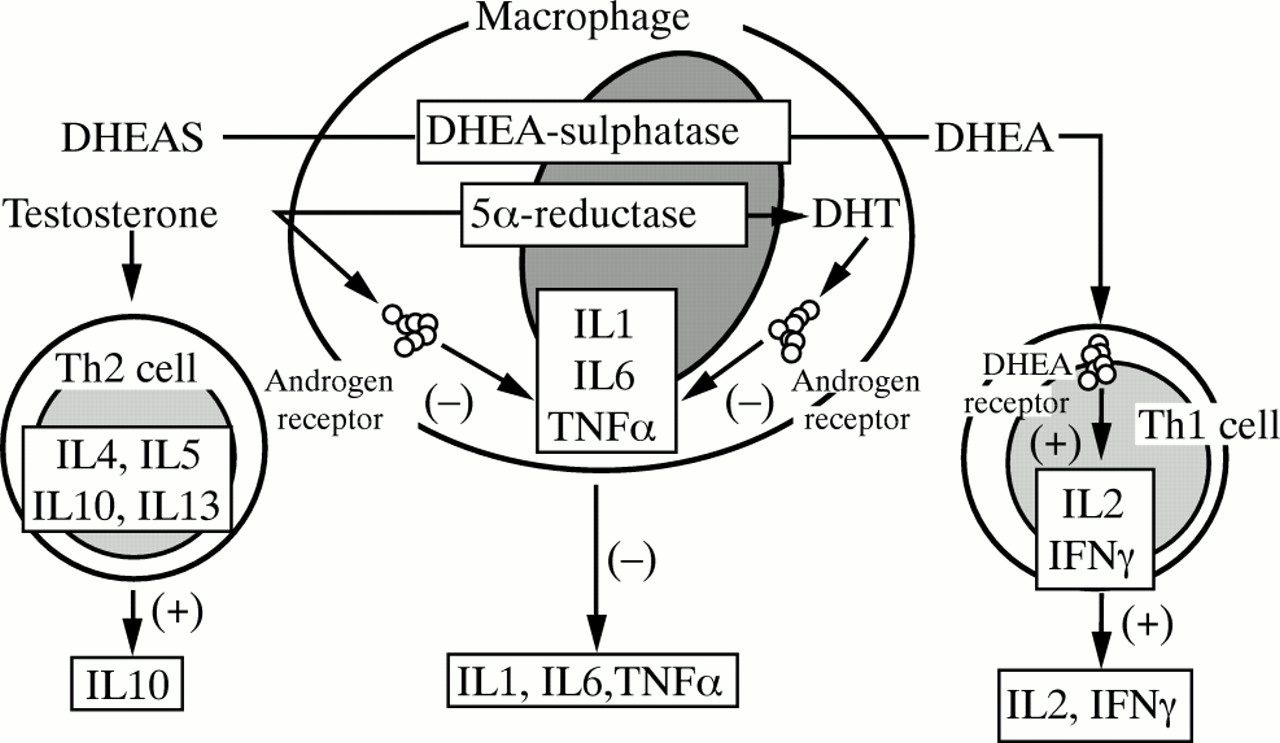
DHEA has been found to have immunomodulatory activities. In vitro studies showed that DHEA increases secretion of IL2 by activated T lymphocytes (even in SLE patients) and decreases production of IL4, IL5, and IL6, thus stimulating Th1-type cytokines (fig3).42 43

{kind=link}
{kind=link}
{kind=link}
Schematic representation of modulatory effects exerted by gonadal (testosterone) and adrenal (DHEA) steroid hormones on cytokine production, at the level of macrophages, Th1, and Th2 cells.
In particular, DHEAS has been found to repress the expression and activity of the human IL6 gene promoter, thus supporting the concept of antiinflammatory/ immunosuppressive effects exerted by androgenic steroids (table 1).44
Specific receptors for the free active adrenal androgen DHEA, have been found in T cells and particularly in activated Th1 subtype of T-cells; however, further studies are needed to elucidate their significance.45
Furthermore, DHEAS is positively correlated with the IL2 soluble receptor in SLE patients.46
Serum DHEA has been found decreased in premenopausal RA patients and in SLE patients, irrespective of age, sex, and disease activity.47 48
Recent double blind and open label studies of SLE patients treated with daily DHEA, showed a clinical efficacy, with the benefits sustained for at least one year in those patients who maintained treatment.49 50
When testosterone was administered to cultures of RA synovial macrophages it was metabolised and inhibited IL1 production, at least.51-53 Similar inhibition of IL1 and IL6, was found on PBMC of RA patients in presence of testosterone.54
In contrast, oestradiol was found to increase IL1 secretion in rat peritoneal macrophages and IL1 and IL6 production in human PBMC.54 55
Low serum testosterone concentrations have been observed in male RA and SLE patients and related to the aetiopathogenesis of the diseases.56 57
Dihydrotestosterone (DHT), the active metabolite of testosterone, has been found to repress the expression and activity of the human IL6 gene promoter via inhibition of NFkB activity through maintenance of IkBa concentrations (fig 3).58 Human and murine macrophages exhibit functional cytoplasma and nuclear testosterone receptors, and both site I (high affinity, low binding) and site II (low affinity, high binding) androgen receptors were found in HLA-DR positive human synovial macrophages.59 60 Therefore, in RA, synovial macrophages appear to be the “link” between the sex hormone environment (testosterone) and the immune response effectors (cytokine modulation).61
Low concentrations of plasma DHEA and DHEAS, have been found significantly correlated with early morning low cortisol concentrations and high basal concentrations of IL6 in RA patients.62 The finding of reduced DHEA production, combined with unexpected normal cortisol production during oCRH and ACTH testing, further support the concept of the presence of an adrenal hypofunction in active RA patients.63
IL6 had a strong effect on steroid release and may be one of the factors controlling the long term adrenal response to stress, because this cytokine is able to act synergistically with ACTH on the adrenal cells to stimulate the release of corticosterone.64Therefore, the altered cortisol and adrenal androgen secretion observed during testing in RA patients not treated with corticosteroids, should be clearly regarded as an “adrenal insufficiency” in the setting of a sustained inflammatory process as shown by high IL6 concentrations.
Reduced concentrations of plasma DHEA and DHEAS, have been found significantly correlated in RA patients with high basal concentrations of IL12.62
Recent studies, indicate that IL12 may play an important part in the perpetuation of Th1 responses in chronic RA, not only by inducing INFγ secretion, but also by expanding Th1 cells.65
Therefore, the association of low DHEA and DHEAS and high IL12 concentrations in RA patients, might suggest their possible combined role in the Th1 cytokine balance.41
Conclusions
An intricate balance, with bidirectional interactions between steroid hormones released by the neuroendocrine system and cytokines released by activated cells of the immune/inflammatory system, mantains the homeostasis in presence of immune/inflammatory diseases, such as RA and SLE.
Pregnancy is considered the most evaluable natural and dynamic model to study the steroid hormone related changes induced on both cytokine patterns and clinical manifestations of these diseases.
Opinions are divided as to whether pregnancy increases risk of the flare of disease in patients with SLE. Patients with inactive disease at conception may be indeed have lower flare rate than controls—that is, pregnancy may be protective against a flare of the disease.66 Classically, it has been said that SLE tends to flare during the last part of pregnancy, however in most of the recent prospective studies, the percentage of flares in the third trimester falls.67 The rise of endogenous steroids and the related influences on cytokine patterns in the late pregancy, seem to explain why the majority of SLE women can have a successful pregnancy.
Further treatment strategies, eventually as combination therapy, may be based on steroid hormone administration, designed to shift antigen specific responses towards the desired Th-type cytokine production in RA and SLE affected patients.