Article Text

Statistics from Altmetric.com
Systemic-onset juvenile idiopathic arthritis (sJIA) is a chronic childhood disease associated with many complications.1–5 Treatments comprise non-steroidal anti-inflammatory drugs, corticosteroids, disease-modifying antirheumatic drugs and biologics,6–9 including tocilizumab, an interleukin-6 receptor monoclonal antibody.10
Results of a randomised, placebo-controlled, phase III trial of tocilizumab in sJIA patients at eight Japanese hospitals, as well as the first 48 weeks of an open-label extension, have been published.3 Protocols and amendments for this extension phase were approved by the Japanese Ministry of Health, Labor and Welfare and the institutional review board at each centre. Of 56 patients initially enrolled, six withdrew during the open-label, lead-in phase (anti-tocilizumab antibodies, three; anaphylactoid reaction, one; gastrointestinal haemorrhage, one; non-efficacy, one). During the double-blind phase, one patient from each treatment arm withdrew because of adverse events (AEs) but re-entered the open-label extension after the resolution of AEs. In total, 50 patients responding to tocilizumab and needing further treatment entered the open-label extension; two patients subsequently withdrew within the first year because of AEs. Herein, the long-term efficacy and safety of treatment through 144 weeks are presented.
American College of Rheumatology Pediatric 30/50/70 response rates were 82.1% (95% CI, 69.6% to 91.1%)/80.4% (67.6% to 89.8%)/75.0% (61.6% to 85.6%), respectively, at week 24 (start of open-label extension) and 83.9% (71.7% to 92.4%)/83.9% (71.7% to 92.4%)/75.0% (61.6% to 85.6%), respectively, at week 144 (last-observation-carried-forward; withdrawals counted as non-responders). Inactive disease11 was achieved in 32 of 56 patients (57.1%) at week 144. Mean daily corticosteroid doses were 0.51 mg/kg at baseline and decreased by ≥50% in 75.6% of patients and by ≥70% in 57.8% of patients completing week 144. Initially observed clinical improvements were maintained through week 144.
Growth was expressed as an SD score (SDS) for height (number of SDs higher/lower than the mean growth curve for same-age general Japanese population) at each time point. Mean baseline SDS-height was −2.67 (SD 1.97), indicating overall growth impairment. Growth impairment correlated with disease duration and was more prominent in patients with long-standing disease (figure 1). Mean change overall (Δ) in SDS-height from baseline to week 144 was minimal (0.04 (SD 1.06)), indicating no difference across the study population; however, individual changes varied widely, with some patients improving (positive ΔSDS-height). Instudy corticosteroid exposure was the most significant factor affecting ΔSDS-height. Adjusted mean ΔSDS-height (95% CI) at week 144 was significantly higher among patients with mean daily prednisolone-equivalent doses below (0.36 (–0.22 to 0.95); n=22) versus above (–0.30 (–0.87 to 0.27); n=23 (p=0.04) figure 2) the median dose of 0.22 mg/kg.
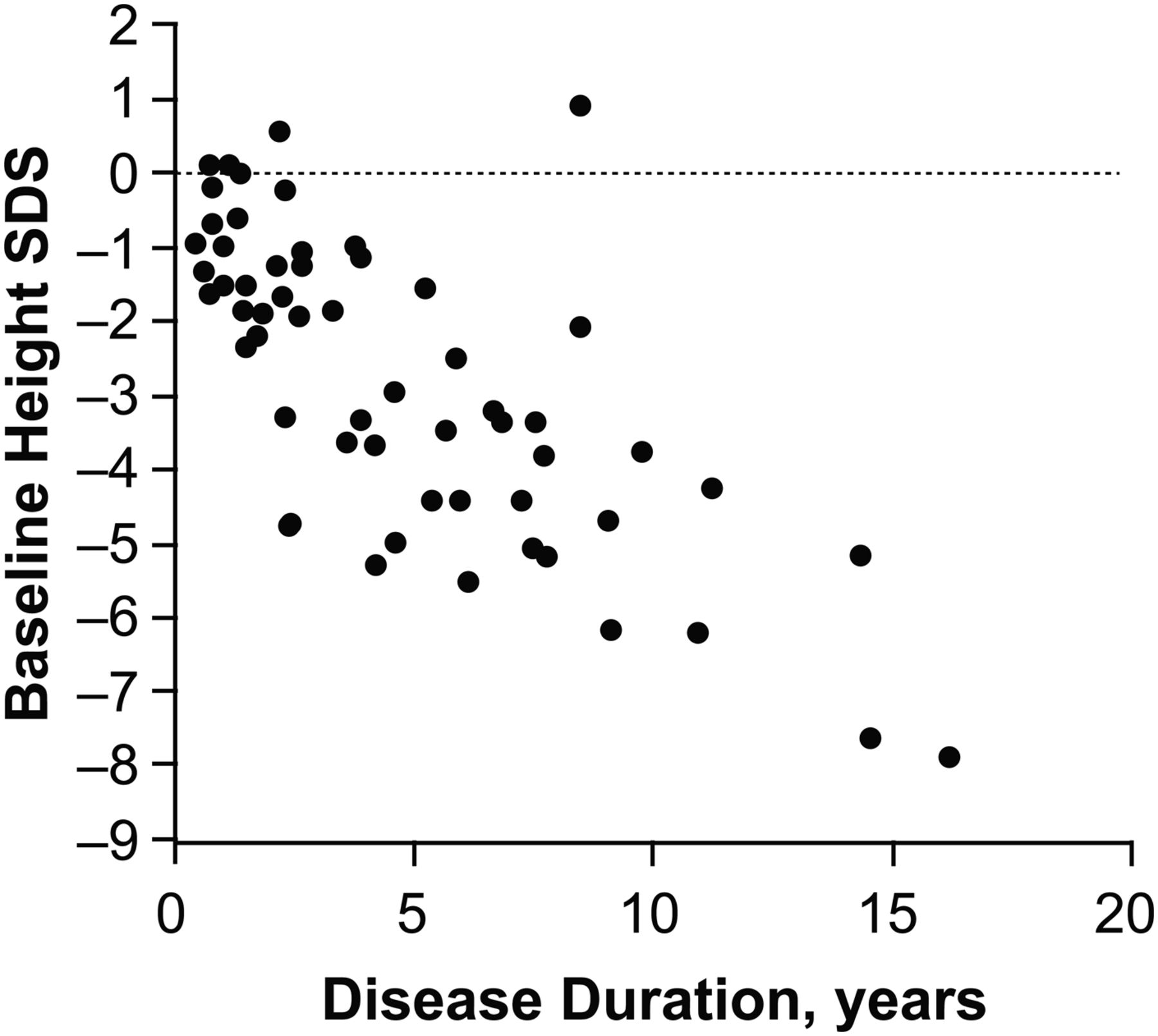
Relationship between baseline-height SD score (SDS) and disease duration (n=56). SDS calculated from the general Japanese population.

{kind=link}
{kind=link}
Adjusted mean ΔSDS-height (±95% CI) by corticosteroid exposure. ΔSDS, change in SDS calculated from the general Japanese population; PSL, prednisolone (*categorised by median); SDS, SD score calculated from the general Japanese population.
All 56 patients reported ≥1 AE (795/100 patient-years (PY)); 93% were mild, and the most common were nasopharyngitis (132.1/100 PY), upper respiratory tract infections (79.4/100 PY) and gastroenteritis (37.1/100 PY). In all, 24 patients reported serious AEs (42.9%; 34.8/100 PY). All neutropenia cases (grade 3 (n=10), grade 4 (n=1)) were transient. Grade 3/4 elevations in liver transaminases occurred in 7/3 patients. No patient developed pulmonary hypertension. No cases of macrophage activation syndrome (MAS) were reported; however, two independently selected cases with possibly MAS-related AEs were adjudicated as one definite and one potential MAS arising from a previous infection/disease flare. Five patients (8.9%) developed anti-tocilizumab antibodies; one continued tocilizumab treatment without a reaction, and four experienced mild to moderate infusion reactions and withdrew from the study per study protocol.
Our findings demonstrate that long-term tocilizumab therapy results in sustained clinical improvements in patients with active sJIA. The growth data observed during the study reiterate the negative correlation between disease duration and growth retardation in >50 sJIA patients and underscore the importance of early intervention and corticosteroid-sparing treatment for catch-up growth.12 Furthermore, the long-term safety profile of tocilizumab was consistent with previous findings in sJIA and rheumatoid arthritis.
Acknowledgments
The authors thank Remi Ozawa, Rumiko Kurosawa, Yasuo Nakagishi, Junpei Kinoshita, Shu-ichi Ito (Yokohama City University), Yoshifumi Kawano, Hiroyuki Imanaka, Nobuaki Maeno, Yasuhito Nerome (Kagoshima University), Yoichi Kohno, Yuzaburo Inoue (Chiba University), Hiroshi Tamai (Osaka Medical College) and Kazuyuki Yoshizaki (Osaka University) for helpful discussions, outpatient care and involvement in the study procedures. The authors wish to acknowledge Bless Castro, PhD, and Maribeth Bogush, PhD, who provided writing services on behalf of F Hoffmann-La Roche.
References
Footnotes
-
Contributors Conception and design, acquisition of data or analysis and interpretation of data: SY, TI, MM (Masaaki Mori), TM (Takako Miyamae), ST, NI, HU, TM (Takuji Murata), MM (Mari Miyoshi), MT, NN, TK. Drafting the article or revising it critically for important intellectual content: SY. Final approval of the version to be published: SY, TI, MM (Masaaki Mori), TM (Takako Miyamae), ST, NI, HU, TM (Takuji Murata), MM (Mari Miyoshi), MT, NN, TK.
-
Competing interests None.
-
Ethics approval Protocols and amendments were approved by the Japanese Ministry of Health, Labour, and Welfare and the institutional review board of each centre. The parent or guardian of every child gave written informed consent, and the child gave assent when appropriate.
-
Funding This study was sponsored by Chugai Pharmaceuticals Co, Ltd. Editorial support was provided by Genentech Inc, a member of the Roche group.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Clinical Trial Registry Numbers: NCT00144599 and NCT00144612.