Article Text

Statistics from Altmetric.com
C reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are traditional markers of disease activity in rheumatoid arthritis (RA). Although the two tests show a relatively high degree of correlation and follow the same reaction pattern, the variance of CRP is independent of ESR to some extent.1 Apart from mirroring inflammation, ESR is affected by immunoglobulin levels, sex, and abnormal size or shape of red blood cells.2,3 CRP, which correlates more significantly than ESR with disease activity,1,3,4 is a predictor of functional status/outcome and joint damage in RA.5–7 Although CRP is the better marker of inflammation, ESR adds information reflecting disease severity,4,8 and a combination of the tests may be worthwhile.
To create a simple instrument for assessment of disease activity in RA, Prevoo et al developed a disease activity score (DAS28) based on the number of tender and swollen joints (n=28), ESR, and the patient’s self estimated general health.9 DAS28 has become an important tool for rheumatologists to monitor disease activity. However, considering its better indication of disease activity, it would be preferable if the CRP value could be used as an alternative to ESR for calculation of the DAS. Paulus et al constructed a nomogram to convert CRP values to ESR,10 which in turn could be successfully used to calculate the traditional DAS.
In our study we investigated whether it was possible simply to use the numerical value of CRP concentration (mg/l) instead of ESR (mm/1st h) for the calculation of DAS28. Seventy patients with recent onset RA (⩽1 year) were included from the ongoing Swedish early RA cohort designated “TIRA”. Each patient was seen by the same rheumatologist at inclusion and after 3, 6, 12, 18, and 24 months. The patients’ assessments of general health assessed by a visual analogue scale (mm), the number of swollen and tender joints respectively (28 joint counts), ESR (mm/1st h), and plasma CRP (mg/l) were registered at all visits. CRP was analysed by turbidimetry at the hospital laboratory and the results presented as <10 or a value without decimals from 10 with no upper limit. CRP <10 was given the value 5. In comparing ESR and CRP, 398 cases were analysed. The traditional DAS28 (DAS28/ESR) was calculated using the formula presented by Prevoo et al.9 A DAS28 based on CRP instead of ESR was also calculated by substituting the numerical value of ESR in the formula by plasma CRP (DAS28/CRP).
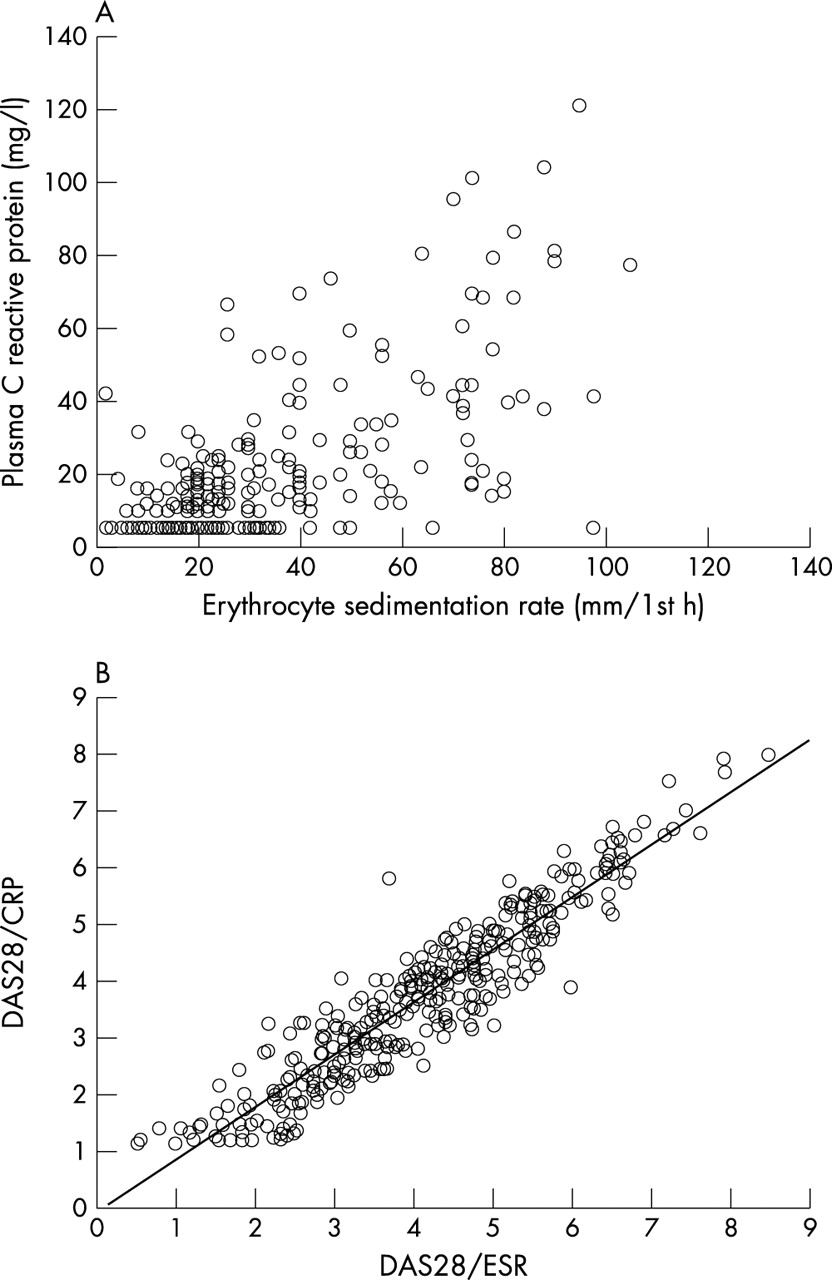
The mean (SD) ESR was 25.4 (2.73) mm/1st h (range 2–105). CRP ranged from 5 to 122 mg/l with a mean (SD) value of 15.65 (19.16). Figure 1A illustrates the correlation between individual CRP and ESR values (Spearman’s correlation coefficient, rs=0.69). Figure 1B illustrates the linear correlation between the two modes of DAS28 calculation (rs=0.93). DAS28 based on ESR ranged from 0.50 to 8.50 (mean (SD) 4.04 (1.48)) and DAS28/CRP ranged from 1.14 to 8.00 (mean (SD) 3.68 (1.46)). Thus the mean (SD) DAS28/ESR of 4.04 (1.48)was not statistically different from DAS28/CRP (3.68 (1.46)).
To conclude, the correlation between ESR and plasma CRP in this study was within the same magnitude as that reported in previous studies on RA.1,4 Although the two values were by no means interchangeable, the correlation between the “orthodox” DAS28 and DAS28 based on plasma CRP was remarkably high, because the weight of the laboratory test is low and thus has only a small impact on the disease activity score compared with the other measures.
These findings may be useful to all rheumatologists who prefer CRP as a laboratory marker of inflammation in RA, and who do not have access to ESR values for the calculation of the DAS28.

{kind=link}
Comparison of ESR and plasma CRP (A), and DAS28 calculated with CRP and ESR respectively (B).
Acknowledgments
We thank Ylva Billing and Ingrid Thyberg for helpful collaboration. This study was financed by grants from the Health Research Council in the southeast of Sweden and by the Swedish Rheumatism Association.