

Abstract
Objective. To investigate the risk factors for chronic anterior uveitis in patients with juvenile idiopathic arthritis (JIA).
Methods. The clinical charts of patients followed between January 1987 and December 2011 were reviewed to establish whether they had uveitis. Inclusion criteria were a diagnosis of JIA and a disease category of persistent oligoarthritis, extended oligoarthritis, rheumatoid factor-negative polyarthritis, psoriatic arthritis, or undifferentiated arthritis. Risk factors included sex, age at arthritis onset, disease category, and antinuclear antibody (ANA) status. The association of risk factors with occurrence of uveitis was evaluated by survival analysis, with first episode of uveitis as the event of interest, and Cox regression analysis.
Results. Of a total of 1189 patients, 278 (23.4%) had uveitis a median of 1.1 years after onset of arthritis. There was no difference in the cumulative probability of developing uveitis between males and females and between patients belonging to different JIA categories, whereas uveitis was strongly associated with age at arthritis onset ≤ 3.5 years and positive ANA. Patients possessing the latter 2 factors in combination had a greater probability of having uveitis than patients who had either of them alone.
Conclusion. In our patients, the risk of uveitis was related to younger age at onset of arthritis and presence of ANA, but not to female sex and disease category. This finding suggests that the patients who require the most intensive ophthalmologic screening are those who have early-onset JIA and are ANA-positive, regardless of their sex or disease subtype.
Juvenile idiopathic arthritis (JIA) is the most frequent cause of chronic anterior uveitis in childhood1,2, and uveitis is the most common form of extraarticular organ involvement in JIA3. The onset of chronic anterior uveitis in JIA is insidious and often entirely asymptomatic, which contrasts with painful, acute iridocyclitis that can be seen in juvenile spondyloarthropathies4. Patients with systemic disease or rheumatoid factor (RF)-positive arthritis rarely develop uveitis. Uveitis is discovered in less than 10% of patients before the onset of arthritis, whereas in most cases it occurs in the earlier years after disease presentation5.
Uveitis is a serious condition and has the potential to cause sight-threatening ocular complications, which include posterior synechiae, band keratopathy, cataract, glaucoma, ocular hypotonia and phthisis bulbi, and cystoid macular edema6,7. Prevention of eye morbidity relies very much on early diagnosis and treatment. Routine implementation of ophthalmologic screening procedures and development of better therapeutic protocols have led to a marked improvement of prognosis in JIA-related uveitis, with a decrease in the reported rate of visual loss from 22–66% in studies before 1990 to 3–25% in recent studies3. However, although guidelines for ophthalmologic surveillance have been proposed, none of them is universally embraced8,9,10,11,12.
Early diagnosis of ocular involvement and optimal design of ophthalmologic screening programs may be facilitated by a thorough knowledge of the risk factors for uveitis development. This information may help to select the patients who need the most careful and intensive monitoring. It may also help to provide appropriate counseling to the family about the probability of the child developing this worrisome complication. A number of independent risk factors for uveitis have been reported, including young age at onset of arthritis, presence of antinuclear antibodies (ANA), oligoarticular disease category, and female sex4. However, the relative contribution of each individual risk factor or of their presence in combination is still uncertain. Several inconsistencies, particularly regarding the association with female sex and oligoarticular subtype, have been observed in different patient series. Further, epidemiology studies made in various geographic areas have suggested that the traditional risk factors may not apply in patients of Asian, Central American, Indian, or Arab origin13.
The aim of the present study was to investigate the risk factors for chronic anterior uveitis in a large sample of patients with JIA seen in a tertiary care Italian setting.
MATERIALS AND METHODS
Study design and patient selection
This was a retrospective cohort study involving patients who were followed up between January 1987 and December 2011. Although the study was conducted at the Istituto Giannina Gaslini of Genoa, the older patients were followed completely or partially at the Fondazione IRCCS Policlinico San Matteo of Pavia, where the group of pediatric rheumatologists who performed the study practiced until December 2001. Thus, all patients were followed by the same group of investigators throughout the study, although in 2 different hospitals. Inclusion criteria were a diagnosis of JIA based on the International League of Associations for Rheumatology (ILAR) criteria14 and a disease category of persistent oligoarthritis, extended oligoarthritis, RF-negative polyarthritis, psoriatic arthritis, or undifferentiated arthritis. Patients were excluded if they met the ILAR criteria for systemic arthritis or RF-positive polyarthritis, owing to the rarity of uveitis in those disease categories. Patients with enthesitis-related arthritis were also excluded because uveitis in this JIA category is usually acute and symptomatic. Patients who developed uveitis before onset of arthritis were excluded.
Included and excluded patients had their ILAR category classified independently by 2 investigators based on the review of clinical charts. Patients seen before December 2008 were classified in a previous study15. Patients seen after that date were classified by investigators SC and MCG. Discordances were resolved, after discussion, by consensus on the final diagnosis among the 2 investigators and the senior investigator (AR). All patients seen before the publication of ILAR criteria for JIA were reclassified using such criteria.
The study protocol was approved by the independent ethics committee of the Istituto Giannina Gaslini of Genoa.
Diagnosis of uveitis
In each patient, the entire clinical history from onset of arthritis to last followup visit was examined to establish whether uveitis had or had not occurred. In patients who developed uveitis, the followup was censored at the time when uveitis was first diagnosed, whereas in patients who did not have uveitis, the followup was censored at last followup visit. Patients without uveitis who had a disease duration of less than 6 months were excluded.
All patients had received a routine ophthalmologic monitoring by slit-lamp evaluation. In ANA-positive patients, eye examinations were performed every 3–4 months for the first 5–7 years after disease onset and every 6–12 months thereafter. In ANA-negative patients, eye examinations were performed every 6–12 months throughout the whole followup period. In all patients, the diagnosis of chronic anterior uveitis was confirmed by an ophthalmologist and was defined according to the Standardization of Uveitis Nomenclature Working Group criteria16. All eye examinations were performed in the study centers. When the patient underwent combined rheumatologic-ophthalmologic evaluation in the clinic, that evaluation was performed by the same ophthalmologist (Dr. A.M. Broglia in Pavia and author RDM in Genoa) throughout the entire study period. Ophthalmologic screening outside the study centers was carried out by the personal ophthalmologist of each patient.
Assessment of risk factors
Patients were identified through existing databases and/or clinic files. The medical charts were reviewed for the following information: sex, age at onset of arthritis, ILAR category, and disease duration (time from onset of arthritis until first episode of uveitis or last followup visit). The date of arthritis onset was defined as the date when the first symptoms of arthritis were noted, obtained by history as recorded in medical charts.
Patients had their ANA status defined if they had at least 2 ANA determinations made at least 3 months apart. Our gathering of this information was facilitated by our policy of repeating ANA determinations several times in patients with the JIA categories under study. Patients were defined as being ANA-positive if they had at least 2 positive results on indirect immunofluorescence at a titer of ≥ 1:160, and as ANA-negative if they had negative results in all determinations. The substrate used for the ANA determinations was rat liver during the first 2 years of the study and human epithelial cell line 2 (HEp-2) cells thereafter. ANA positivity or negativity was confirmed in at least 2 HEp-2 cell assays in all patients for whom the initial assays were done using rat liver as substrate. Patients who had no or 1 ANA determinations available or who had ≥ 2 ANA determinations but who did not meet the criteria for ANA positivity or negativity were classified as having an “indeterminate” ANA status.
Clinical data for each patient were collected by investigators SC, MCG, BL, and VM using a standardized form developed specifically for our study. Data were then entered into an electronic database.
Statistics
Descriptive statistics were reported as medians and interquartile ranges (IQR) for continuous variables and as absolute frequencies and percentages for categorical variables. Comparisons of quantitative variables between the 2 groups were made by means of Mann-Whitney U test. Categorical data were compared by the chi-square test, or by Fisher’s exact test in case of expected frequencies < 5. Survival analysis in each group, with the first episode of uveitis as the event of interest, was conducted by means of the Kaplan-Meier method. Survival curves were compared by the log-rank test. Before the application of survival analysis, the age at arthritis onset was dichotomized to a binary variable. The cutpoint was obtained through receiver-operating characteristic (ROC) curve analysis. The association of risk factors with occurrence of uveitis was then tested in a Cox proportional hazards regression model. The likelihood ratio test was used for comparisons, and p < 0.05 was considered as statistically significant. The software Statistica (release 6.0, StatSoft Corporation) and Stata (release 7.0) were used for data analyses.
RESULTS
A total of 1250 patients fulfilled the criteria for inclusion in our study. Four patients were excluded because they developed uveitis before onset of arthritis, and 57 patients without uveitis were excluded owing to a disease duration of less than 6 months. The demographic and clinical characteristics of the remaining 1189 patients are presented in Table 1. Overall, the series was overly represented by females with early disease onset and positive ANA status. About half of patients had the ILAR category of persistent oligoarthritis; RF-negative polyarthritis was more common than extended oligoarthritis. Patients with an indeterminate ANA status were excluded from the analysis of the association between uveitis and ANA. The large majority of patients (80–90%) were of Italian ancestry. Because both study centers are large tertiary care referral hospitals whose catchment area extends to the entire country, the study sample is likely representative of the overall Italian pediatric population.
Demographic and clinical characteristics of study patients, considered as a whole and by occurrence of uveitis. Data are the number (percentages) unless otherwise indicated.
A total of 278 patients (23.4%) had uveitis a median of 1.1 years (IQR 0.2–2.5 yrs) after onset of arthritis. The median (IQR) age at occurrence of uveitis was 4.0 years (2.7–5.8 yrs). Table 1 shows the comparison of risk factors for uveitis between patients who developed or did not develop uveitis. Compared with the group without uveitis, patients who had ocular disease had a younger age at onset of arthritis and a greater frequency of ANA positivity. The 2 patient groups were comparable for the proportion of females and the distribution of ILAR categories. The median (IQR) disease duration of the 911 patients who did not develop uveitis was 4.8 years (2.3–8.7 yrs). Of these patients, 204 (22.4%) had a disease duration < 2 years, and 479 (52.6%) had a disease duration < 5 years.
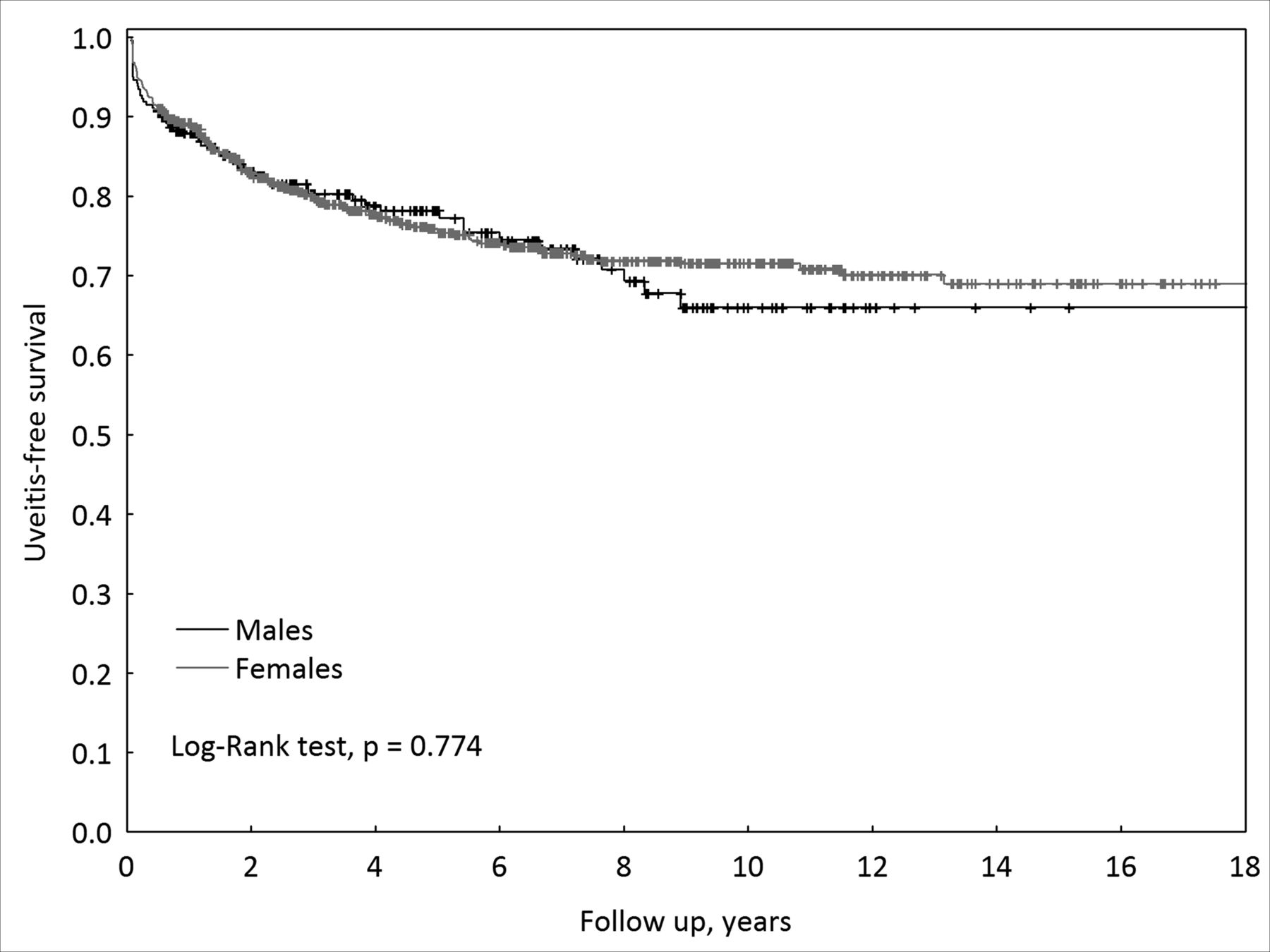
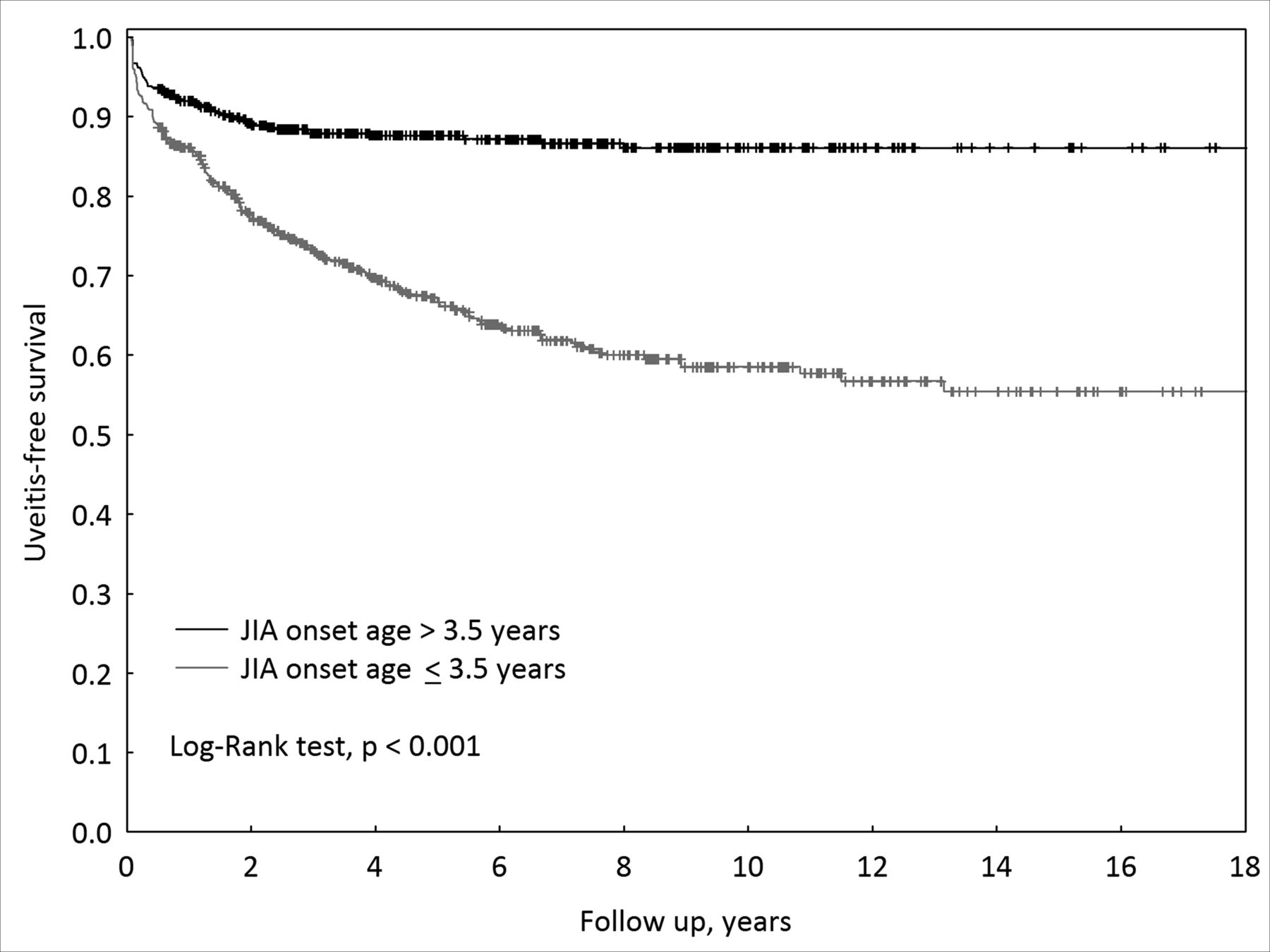
The survival analysis, with the first episode of uveitis as the event of interest, in patients stratified by the absence or presence of each risk factor is presented in Figures 1 to 4. There was no difference in the cumulative probability of developing uveitis between males and females (Figure 1) and between patients belonging to each of the 3 main ILAR categories of JIA (persistent oligoarthritis, extended oligoarthritis, and RF-negative polyarthritis; Figure 2). Patients with an age at onset of arthritis ≤ 3.5 years had a cumulative probability of having uveitis about 3 times greater than patients with an age at onset of arthritis > 3.5 years (Figure 3). Notably, for the purpose of this analysis, the cutpoint for age at onset of arthritis was not selected on clinical grounds but was obtained through ROC curve analysis. Patients with a positive ANA status had a cumulative probability of experiencing ocular involvement about 5 times greater than patients with negative ANA (Figure 4).

Cumulative probability of not developing uveitis by sex; Kaplan-Meier method. Among females, the number who had uveitis/total subjects was 219/930 (23.6%) and the incidence rate (IR; 95% CI) of uveitis was 45.9 (40.2–52.5). Among males, the number who had uveitis/total subjects was 59/259 (22.8%) and the IR (95% CI) of uveitis was 53.2 (41.2–68.6).

Cumulative probability of not developing uveitis by International League of Associations for Rheumatology category; Kaplan-Meier method. Among patients with persistent oligoarthritis, the number who had uveitis/total subjects was 146/628 (23.2%) and the incidence rate (IR; 95% CI) of uveitis was 47.9 (40.8–56.4). Among patients with extended oligoarthritis, the number who had uveitis/total subjects was 46/173 (26.6%) and the IR (95% CI) of uveitis was 51.1 (38.3–68.3). Among patients with rheumatoid factor (RF)-negative polyarthritis, the number who had uveitis/total subjects was 66/276 (23.9%) and the IR (95% CI) of uveitis was 50.2 (39.5–64.0).

Cumulative probability of not developing uveitis by age at onset of arthritis; Kaplan-Meier method. Among patients with age at arthritis onset ≤ 3.5 years, the number who had uveitis/total subjects was 212/636 (33.3%) and the incidence rate (IR; 95% CI) of uveitis was 68.8 (60.2–78.7). Among patients with age at arthritis onset > 3.5 years, the number who had uveitis/total subjects was 66/553 (11.9%) and the IR (95% CI) of uveitis was 23.6 (18.5–30.0).

Cumulative probability of not developing uveitis by ANA status; Kaplan-Meier method. Among ANA-positive patients, the number who had uveitis/total subjects was 253/873 (29.0%) and the incidence rate (IR; 95% CI) of uveitis was 58.2 (51.4–65.8). Among ANA-negative patients, the number who had uveitis/total subjects was 12/228 (5.3%) and the IR (95% CI) of uveitis was 10.1 (5.7–17.8). ANA: antinuclear antibody.
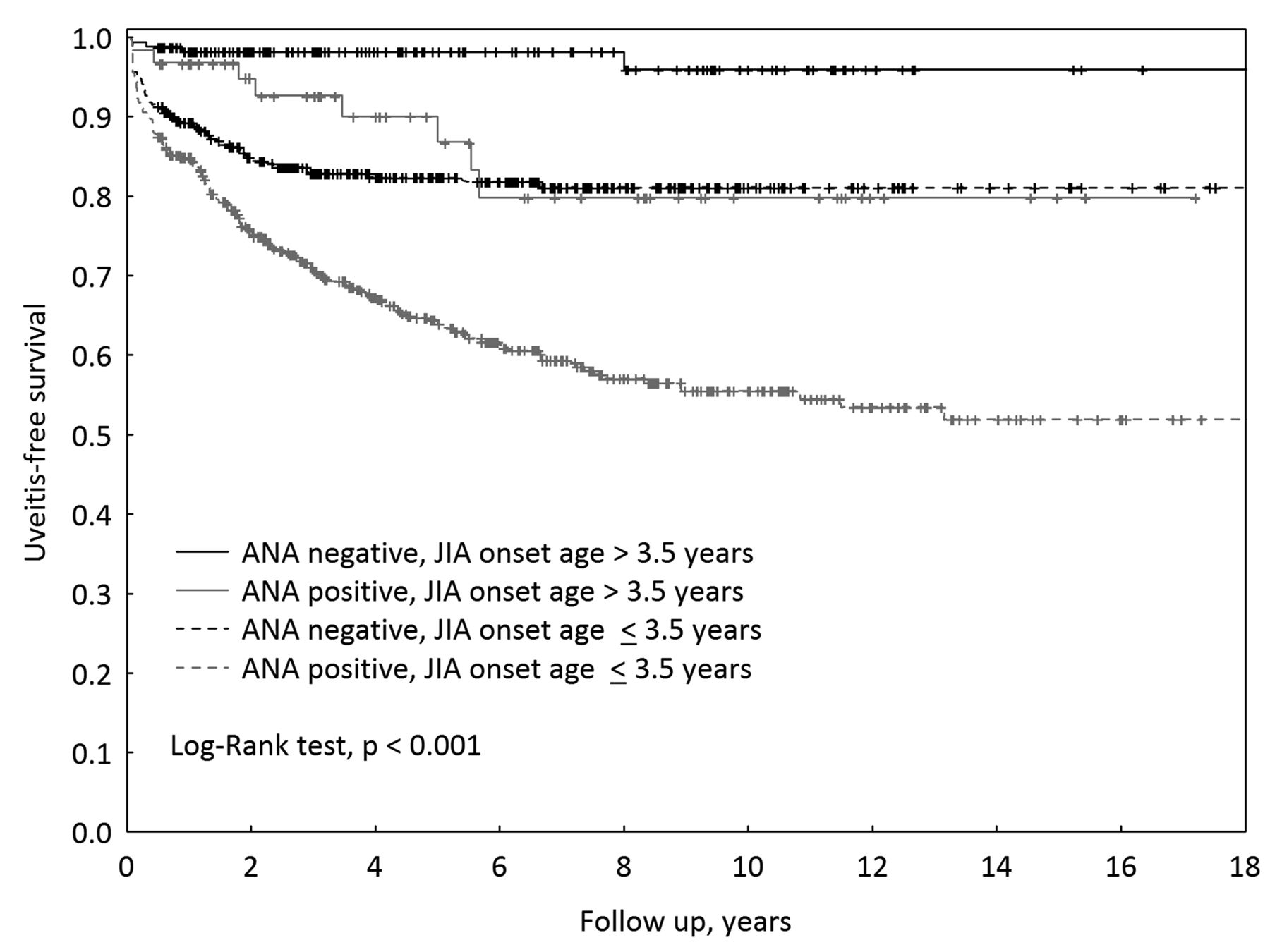
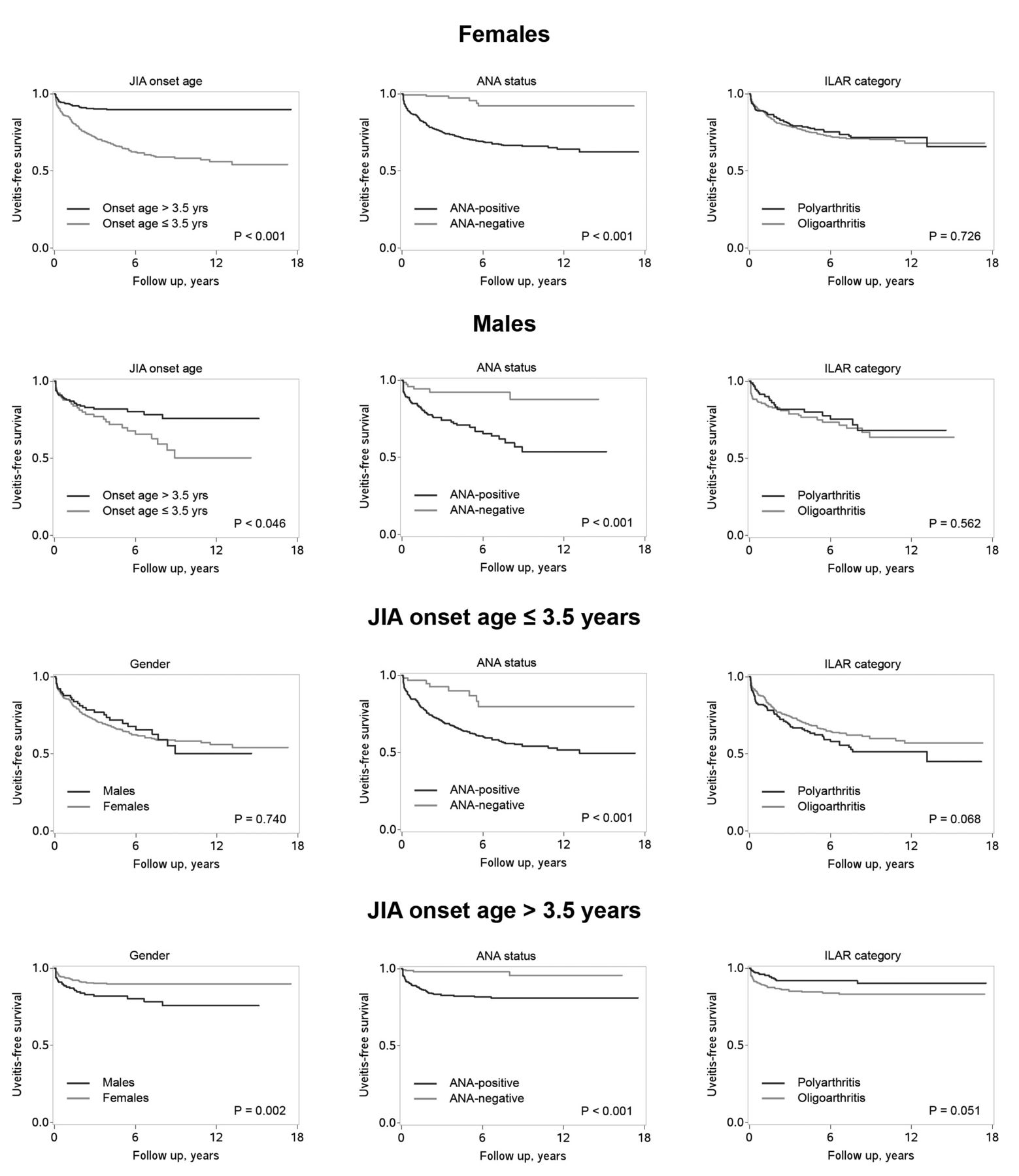
The evaluation of the presence of age at arthritis onset ≤ 3.5 years and ANA positivity in combination (Figure 5) revealed that patients possessing both these characteristics had a greater probability of having uveitis than did patients who had either of these characteristics alone. Around one-third of patients who had both these clinical features developed ocular disease during followup. Conversely, the risk of uveitis among patients with age at arthritis onset > 3.5 years and negative ANA was negligible. The simultaneous presence of age at arthritis onset ≤ 3.5 years or ANA positivity with either the female sex or the oligoarthritis category did not lead to a noticeable increase in the cumulative probability of uveitis (Appendix 1 and 2). However, in the patient subgroup with age at arthritis onset > 3.5 years, the frequency of uveitis was higher in males than in females. The predictive role of younger age at onset and positive ANA status was confirmed by Cox proportional hazard regression analysis (results not shown).

Cumulative probability of not developing uveitis by age at onset of arthritis and ANA status evaluated in combination; Kaplan-Meier method. Among ANA-positive patients with age at arthritis onset ≤ 3.5 years, the number who had uveitis/total subjects was 195/531 (36.7%) and the incidence rate (IR; 95% CI) of uveitis was 75.7 (65.7–87.1). Among ANA-positive patients with age at arthritis onset > 3.5 years, the number who had uveitis/total subjects was 58/342 (17.0%) and the IR (95% CI) of uveitis was 32.7 (25.3–42.3). Among ANA-negative patients with age at arthritis onset ≤ 3.5 years, the number who had uveitis/total subjects was 8/62 (12.9%) and the IR (95% CI) of uveitis was 23.4 (11.7–46.7). Among ANA-negative patients with age at arthritis onset > 3.5 years, the number who had uveitis/total subjects was 4/166 (2.4%) and the IR (95% CI) of uveitis was 4.7 (1.8–12.6). ANA: antinuclear antibody.
To further investigate the relationship between the risk of uveitis and age at onset of arthritis, sex, and presence of ANA, we calculated the rate of uveitis by sex and ANA status in patients grouped according to age at arthritis onset (using clinically meaningful cutpoints; Table 2). This analysis confirmed that the frequency of uveitis was comparable in males and females among patients with onset at < 3 years of age, whereas among patients who were older than 3 years at arthritis onset, uveitis was more common in males. A similar trend was seen when the analysis was restricted to only ANA-positive patients with uveitis.
Rate of uveitis according to age at onset of arthritis, sex, and ANA status. Data are number (%).
Because in our patient series uveitis was found to occur most frequently in the first 2 years after onset of arthritis and to become less common after 5 years5, we reexamined the role of each risk factor in sensitivity analyses after excluding patients without uveitis who had < 2 years or < 5 years of disease duration. Altogether, the results of these analyses were comparable to those obtained on the entire patient sample (results not shown). Only 13 patients (4.7%) developed uveitis 7 years or more after the onset of arthritis. All but 1 had an age at arthritis onset ≤ 3.5 years and were ANA positive, and 8 of them were females.
DISCUSSION
We investigated the risk factors for uveitis in an inception cohort of 1189 patients with JIA followed up by our group over a 25-year period. The study population is remarkable for the high prevalence of females, the very high rate of ANA positivity, and the very young age at onset of arthritis. The prevalence of uveitis observed in our sample (23.4%) is higher than the 12–16% frequency reported in most studies from Western countries3. This difference can be explained at least partially by our choice to restrict the analysis to the ILAR categories characterized by a high risk for the development of chronic anterior uveitis. The median/mean time from onset of arthritis to diagnosis of uveitis in our patients (1.1/1.9 yrs) is in the range of that reported in other recent series3,17.
Our finding of the lack of association with the female sex contrasts with the previous demonstrations of a higher cumulative incidence of uveitis in females than in males8. However, it has been argued that these observations may simply reflect the greater female predominance in the JIA group most at risk of uveitis (i.e., early onset, ANA-positive), and the low risk in older boys with JIA who frequently turn out to have enthesitis-related arthritis18. Sex was not found to be an independent risk factor for uveitis in a multivariate analysis of data of the German registry11. A study from Canada suggested an interrelation between age at onset of arthritis and sex in determining the risk of uveitis19. However, females were significantly more susceptible to ocular involvement than males only in the subgroup with early onset of arthritis (and ANA positivity). Conversely, we found that the prevalence of uveitis was comparable between the sexes in the subgroup with earlier onset of arthritis, whereas among patients with older onset age, the risk was greater in boys. Taken together, these findings do not indicate that female sex is an independent risk factor for uveitis in JIA. The reason for the higher risk for uveitis in older boys observed in our study is unclear, but did not depend on differences in the prevalence of ANA positivity between sexes.
Likewise, the similar distribution of uveitis across disease categories seen in our cohort diverges from the results of several previous studies, which found the risk of uveitis to be higher in patients with oligoarthritis and lower in patients with RF-negative polyarthritis8. In line with our findings, analyses from Scandinavian countries showed that the incidence of uveitis was highest in patients with polyarthritis and similar in patients with persistent and extended oligoarthritis20,21,22. These discrepancies may depend on differences in the characteristics of the patient populations, but may also reflect the inadequacy of the number of affected joints as a classification criterion for JIA23.
The association of uveitis with early-onset JIA was described as early as 195724, and was substantiated in a number of subsequent prospective investigations11,25. That uveitis was related to the presence of ANA was noticed about 20 years later, when ANA testing in children with arthritis became routine26. However, it has long been observed that ANA positivity was an independent risk factor for uveitis in close link with younger age at onset and the oligoarticular subtype. In the German registry, the cumulative incidence of uveitis was higher in ANA-positive than in ANA-negative patients in the oligoarthritis subgroup, but was comparable between ANA-positive and ANA-negative patients with polyarthritis8. Contrary to that report, we previously found that the frequency of ocular involvement was similar across ANA-positive patients belonging to different JIA categories15,27. This observation was confirmed in our present study, where the onset subtype did not affect the association of ANA positivity with uveitis. A large cohort study from Canada also found no difference in the risk of uveitis development in ANA-positive patients with different JIA subsets19. Altogether, these data support the hypothesis that patients with ANA-positive JIA constitute a homogeneous subgroup, irrespective of the course of joint disease23,27,28.
A recent analysis in a very large sample of children with JIA conducted by the Childhood Arthritis and Rheumatology Research Alliance (CARRA) found that children with uveitis (prevalence 11.6%) were younger at arthritis onset and more likely to be female, to have oligoarticular JIA, and to be ANA-positive29. The discordance between our results and those of the CARRA study and the inconsistencies in the risk factors reported in the literature underscore the need for a multinational, multicenter study aimed to compare the prevalence, characteristics, and predictors of JIA-associated uveitis in different geographic areas.
Our study should be interpreted in the light of several limitations, such as its retrospective nature. Because the duration of followup of patients without uveitis was not uniform, it is possible that some patients in our cohort will develop new-onset uveitis subsequent to the end of the study, and this would change the prevalence rate and the median time to diagnosis of uveitis, and might alter the relative effect of risk factors. However, survival curves obtained after the exclusion of patients with a followup shorter than 2 or 5 years showed trends similar to those seen in the entire patient population. Additional limitations of our study are the lack of assessment of the effect of medications and of HLA-B27 status on uveitis development. We acknowledge the relatively small size of the psoriatic and undifferentiated arthritis samples, which precluded a meaningful analysis of the risk of uveitis in these JIA categories. Nevertheless, similar trends in the association of uveitis with earlier age at arthritis onset and ANA positivity and lack of association with the female sex were detectable in both psoriatic and undifferentiated arthritis (results not shown). In the absence of agreed-upon criteria for positivity of ANA, we relied on tests performed on rodent or HEp-2 substrates30 and chose a cutoff of 1:160 to define positivity. However, we recognize that this cutoff is arbitrary and that other cutoffs may prove equally suitable in other centers or laboratories. Because the large majority of our study population was of Italian ancestry, it is not certain whether the ANA-positive phenotype of our patients is similarly seen in all genetic backgrounds. Notably, no association of uveitis with ILAR category, younger onset age, and female sex was seen among patients with undetermined ANA status (results not shown).
We found that the risk of uveitis in our patients with JIA was strongly related to younger age at onset of arthritis and presence of ANA, but not to sex and disease category. Based on our findings, we suggest that the patients who require the most intensive ophthalmologic screening are those who have onset of arthritis before 3 years of age and are ANA-positive, regardless of their sex or JIA subtype. In keeping with current recommendations, our results suggest that screening intervals be extended if uveitis has not developed 7 years from onset of arthritis, because occurrence of ocular disease after that time is rare.
APPENDIX 1

Cumulative probability of not developing uveitis in females and males and in patients with age at arthritis onset ≤ 3.5 years or > 3.5 years by the presence of each other risk factor; Kaplan-Meier method. Patients with persistent and extended oligoarthritis were combined in the oligoarthritis group. JIA: juvenile idiopathic arthritis; ANA: antinuclear antibody; ILAR: International League of Associations for Rheumatology.
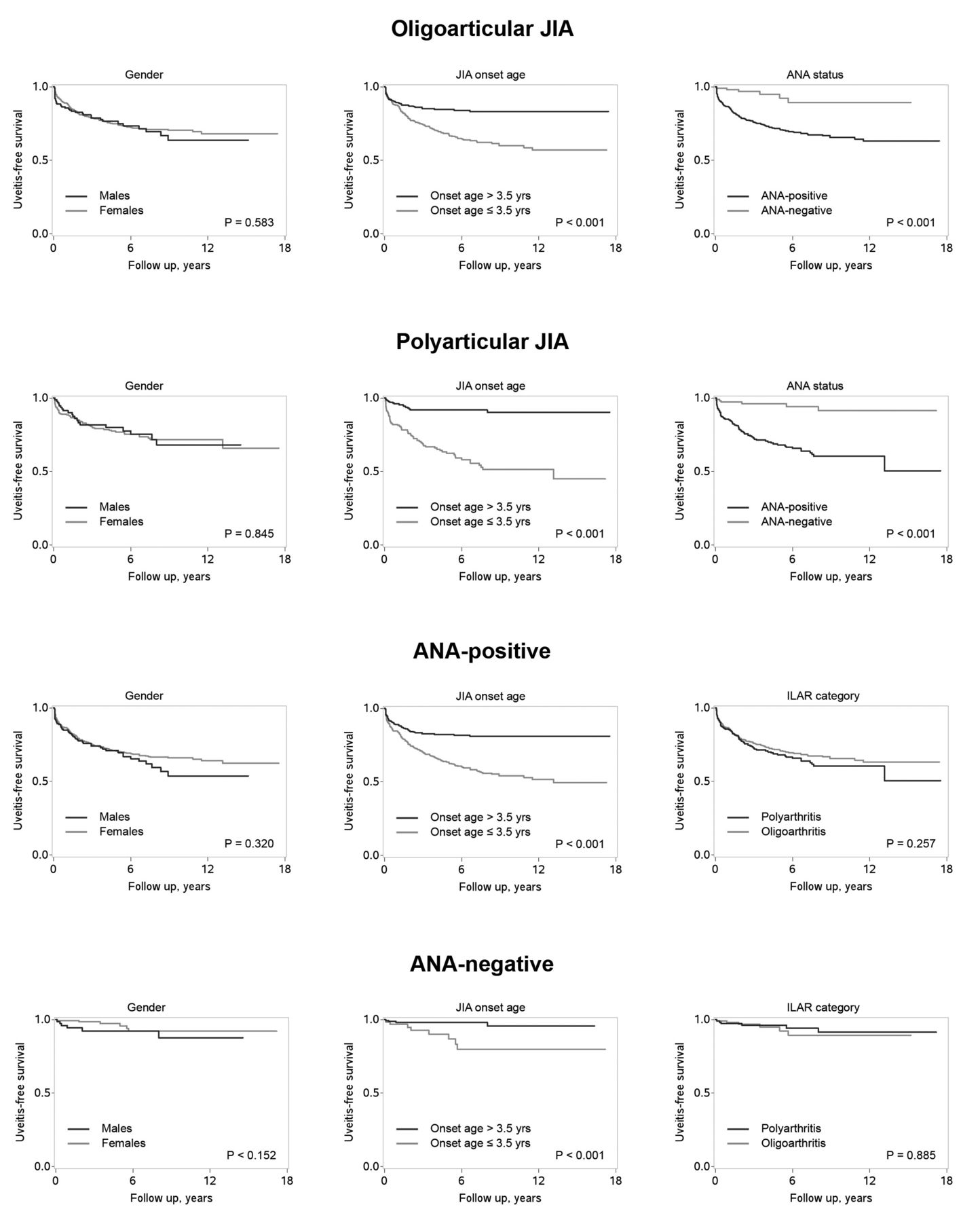
APPENDIX 2.
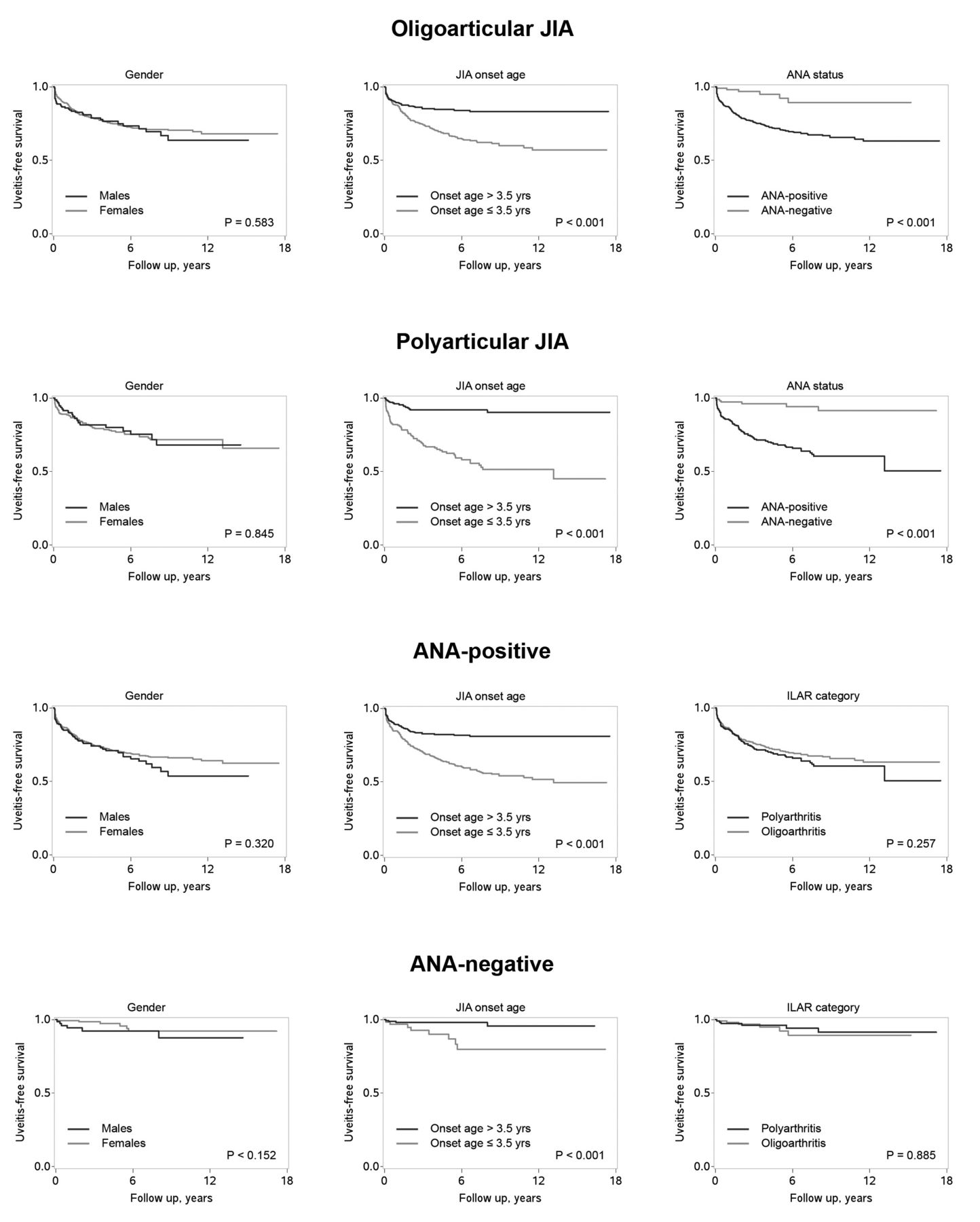
Cumulative probability of not developing uveitis in patients with oligoarthritis or polyarthritis and in ANA-positive or ANA-negative patients by the presence of each other risk factor; Kaplan-Meier method. Patients with persistent and extended oligoarthritis were combined in the oligoarthritis group. ANA: antinuclear antibody; JIA: juvenile idiopathic arthritis; ILAR: International League of Associations for Rheumatology.
- Accepted for publication March 4, 2014.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}