

Abstract
Objective. To assess the diagnostic value for axial spondyloarthritis (SpA) of unilateral sacroiliitis in scintigraphy in daily clinical practice.
Methods. In 207 patients with chronic back pain, the diagnostic value of scintigraphy was assessed retrospectively. The diagnosis made by the rheumatologist (axial SpA vs no axial SpA) was the standard.
Results. Sensitivities of scintigraphy for any (unilateral or bilateral), bilateral, and isolated unilateral sacroiliitis were 64.9%, 40.2%, and 24.7%, respectively. Respective specificities were 50.5%, 57.7%, and 92.8%, resulting in likelihood ratios of 1.3, 1.0, and 3.4.
Conclusion. Scintigraphy of the sacroiliac joints is of limited value for the diagnosis of axial SpA. Unilateral compared to bilateral sacroiliitis is slightly superior, but is associated with a low sensitivity.
A recent systematic literature search showed that scintigraphy of the sacroiliac joints (SIJ) is of limited value for the diagnosis of axial spondyloarthritis (SpA)1. In daily clinical practice, an isolated unilateral sacroiliitis in bone scintigraphy is often regarded to be of better diagnostic value because the negative side acts as an internal control, while in the case of bilateral sacroiliitis the definition of positive/negative is more difficult. We retrospectively analyzed a cohort of patients who were referred because of suspected SpA to a specialized tertiary rheumatology center with special interest in SpA, and considered whether unilateral sacroiliitis would have a higher diagnostic value compared to bilateral sacroiliitis.
MATERIALS AND METHODS
Patients
We retrospectively analyzed patients with chronic low back pain who were seen in our back pain clinic2 and who had undergone a bone scintigraphy examination for the evaluation of sacroiliitis. A diagnosis of axial SpA was made by experienced rheumatologists according to the modified New York criteria for ankylosing spondylitis (AS)3 or for nonradiographic axial SpA2,4–6. Importantly, for the diagnosis of axial SpA, scintigraphy findings were not taken into account. Controls were defined as those patients in whom the expert excluded the diagnosis of axial SpA.
Scintigraphy
Bone scintigraphy findings were classified into unilateral or bilateral sacroiliitis, and suspicion for or exclusion of sacroiliitis. Where available, we collected information about the exact value of the SIJ-sacrum-index (SIJ-S-index), which quantifies the uptake of the radio-tracer in the SIJ compared to the sacrum as a reference point. The decision about whether a scintigraphy result showed active sacroiliitis was based on the judgment of the radiologist who had performed the scintigraphy examination.
Statistics
Sensitivity, specificity, and likelihood ratio (LR) of scintigraphy for the diagnosis of axial SpA were calculated.
RESULTS
Out of 1202 patients who have been referred to our clinic for the evaluation of back pain, in 207 cases (17.2%) a scintigraphy examination of the SIJ had been performed before referral for the evaluation of sacroiliitis. Out of these 207 patients, we classified 97 as having axial SpA (56 as AS and 41 as nonradiographic axial SpA), 13 as suspicious for axial SpA, and 97 as controls2,4,5. Demographic and clinical data are shown in Table 1.
Demographic and clinical data for the different patient groups who underwent a scintigraphy examination for the evaluation of sacroiliitis. In the patient group with axial SpA, patients with AS and patients with nonradiographic axial SpA are pooled.
Discriminative property of scintigraphy of the SIJ between patients and controls
All 207 scintigraphy examinations had been performed using 99m technetium-labeled radio-tracers. The mean radiation dose was 568.9 mBq (SD 94.8). In 50.2% (104/207) of scintigraphy examinations, absolute values for the SIJ-S-index were provided.
First, we analyzed whether there was a difference between patients with axial SpA and controls regarding tracer uptake, independent of bilateral or unilateral sacroiliitis. There was no statistically significant difference between patients with axial SpA (mean uptake left SIJ/right SIJ 1.48/1.46; mean cutoff 1.33) and controls (mean uptake left SIJ/right SIJ 1.48/1.41; mean cutoff 1.30).
Diagnostic properties of scintigraphy for sacroiliitis
We next split scintigraphy findings into bilateral and unilateral sacroiliitis independently of quantification. Thus, for the following analysis, qualitative and quantitative scintigraphy findings were analyzed for 97 patients with axial SpA and 97 controls. Only positive or negative findings were counted, according to the radiologist who had performed the scintigraphy examination.
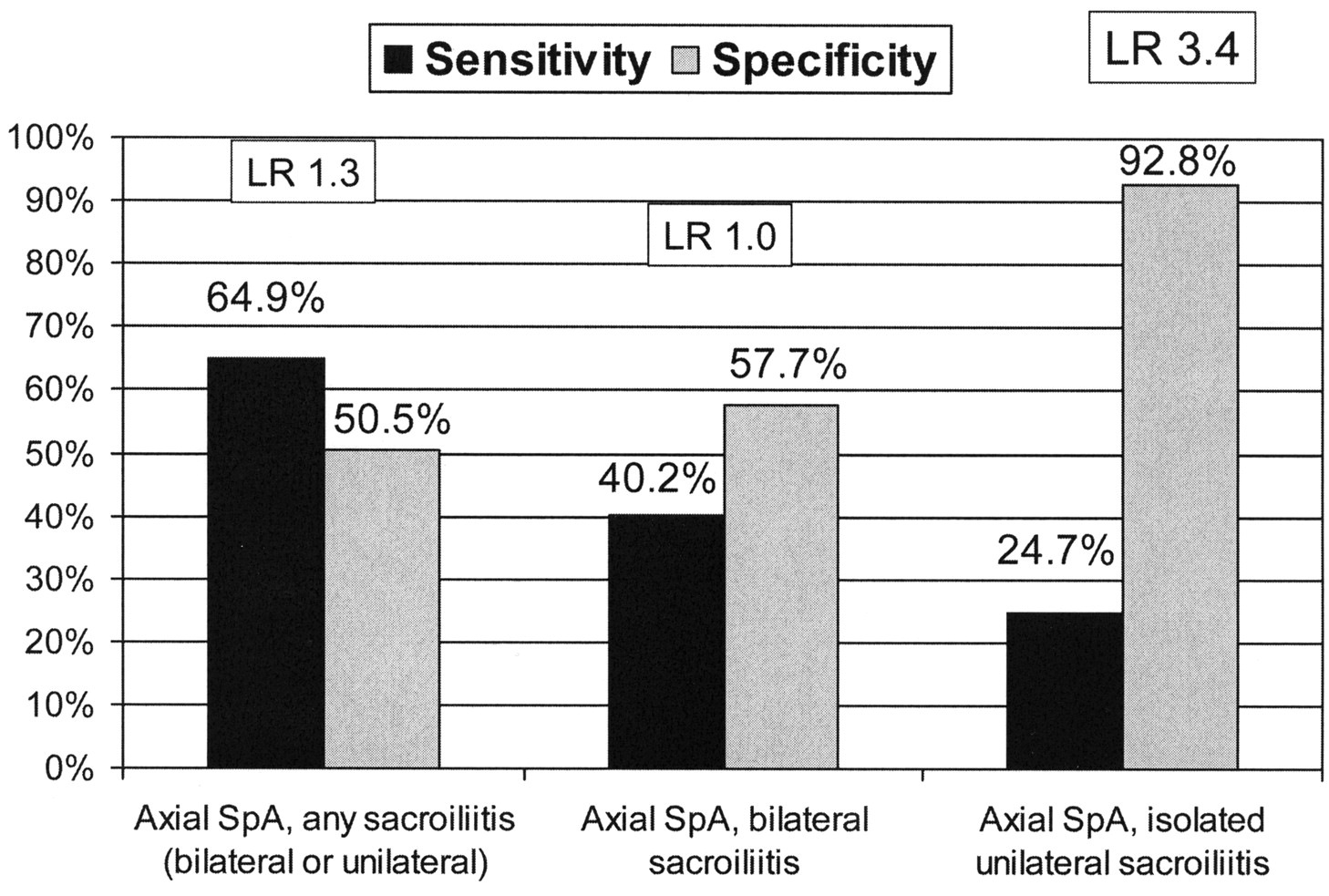
Among 97 patients with axial SpA, scintigraphy showed any sacroiliitis (bilateral or unilateral) in 64.9%, bilateral sacroiliitis in 40.2%, and unilateral sacroiliitis in 24.7%. Based on the analysis of the 97 controls, specificities of 50.5%, 57.7%, and 92.8% and LR of 1.3, 1.0, and 3.4, respectively, were found (Figure 1 and group A in Table 2).

Sensitivity, specificity, and likelihood ratio (LR) of bone scintigraphy showing any sacroiliitis, bilateral sacroiliitis, or isolated unilateral sacroiliitis. Data are shown for the whole group of axial spondyloarthritis (SpA, n = 97) and non-SpA controls (n = 97). Specificities are calculated from 97 controls.
Sensitivity, specificity, and likelihood ratio (LR) of scintigraphy imaging for the diagnosis of axial spondyloarthritis (SpA). Scintigraphy examinations of the sacroiliac joints were performed in 207 patients. Of them, 97 patients were classified with axial SpA, 13 patients with suspicion for axial SpA, and 97 as controls.
In the 2 subgroups with established AS (n = 56, Group A1 in Table 2) compared to nonradiographic axial SpA (n = 41, Group A2 in Table 2), as well as in the AS subgroups with sacroiliitis grade 2/3 (Group A1a in Table 2) and sacroiliitis grade 4 (Group A1b in Table 2), the value of scintigraphy for the diagnosis of axial SpA was very similar compared to the pooled group of axial SpA. In the subgroup of patients with axial SpA in whom absolute values of the SIJ-S-index were given (26 patients with AS, 21 patients with nonradiographic axial SpA, and 48 controls, Group B in Table 2), it could be shown that quantitative scintigraphy was not superior to qualitative scintigraphy.
DISCUSSION
Our retrospective analysis shows that scintigraphy is still used in a proportion of patients for the evaluation of sacroiliitis. About 17% of referred patients with back pain had undergone a scintigraphic examination of the SIJ. Further, our study confirms data of a recent systematic literature search that showed that scintigraphy of the SIJ is at best of limited value for the diagnosis of axial SpA1. This is especially true for bilateral sacroiliitis, which showed only a +LR 1.0 in our study, meaning that it is of no use at all. Unilateral sacroiliitis as shown by scintigraphy showed a slightly higher LR of 3.4. At the same time, unilateral sacroiliitis on scintigraphy was associated with a very low sensitivity of about 25%. Further, an LR of 3.4 of scinti-graphic unilateral sacroiliitis is much lower than an assumed LR of around 10 for magnetic resonance imaging (MRI)5.
Our findings are in concordance with the few scintigraphy studies that have so far reported on unilateral sacroiliitis (6, including 104 patients with axial SpA and 36 controls)7–12. Sensitivities of unilateral sacroiliitis in these studies were low, ranging from 6.3%10 to 33.3%12, while specificities were high, ranging between 89.5%8 and 94.1%7, resulting in a pooled LR of 2.1.
In the diagnostic approach in our center, scintigraphy results are not included because there has been no proven value for this method for the diagnosis of axial SpA. The optimal study design would be a prospective study with patients with SpA and patients without SpA who are undergoing scintigraphy of the SIJ. Looking at all available data on the limitation of scintigraphy and the superiority of MRI, it is questionable whether such a study is still feasible.
The diagnostic value of scintigraphy of the SIJ might be better in clear cases of unilateral sacroiliitis shown by scintigraphy that correlates with the patient’s symptoms of unilateral buttock pain. This information was not available for our study, and such an analysis has not been performed in the literature.
Our analysis shows that scintigraphy of the SIJ is of quite limited value for the diagnosis of axial SpA. Unilateral sacroiliitis is slightly superior compared to scintigraphy showing a bilateral sacroiliitis, but is associated with a low sensitivity.
Footnotes
- Accepted for publication February 4, 2010.








{kind=link}