

Abstract
Objective.To investigate the pharmacokinetic and pharmacodynamic interaction between probenecid and oxypurinol (the active metabolite of allopurinol) in patients with gout.
Methods.This was an open-label observational clinical study. Blood and urine samples were collected to measure oxypurinol and urate concentrations. We examined the effects of adding probenecid to allopurinol therapy upon plasma concentrations and renal clearances of urate and oxypurinol.
Results.Twenty patients taking allopurinol 100–400 mg daily completed the study. Maximum coadministered doses of probenecid were 250 mg/day (n = 1), 500 mg/day (n = 19), 1000 mg/day (n = 7), 1500 mg/day (n = 3), and 2000 mg/day (n = 1). All doses except the 250 mg daily dose were divided and dosing was twice daily. Estimated creatinine clearances ranged from 28 to 113 ml/min. Addition of probenecid 500 mg/day to allopurinol therapy decreased plasma urate concentrations by 25%, from mean 0.37 mmol/l (95% CI 0.33–0.41) to mean 0.28 mmol/l (95% CI 0.24–0.32) (p < 0.001); and increased renal urate clearance by 62%, from mean 6.0 ml/min (95% CI 4.5–7.5) to mean 9.6 ml/min (95% CI 6.9–12.3) (p < 0.001). Average steady-state plasma oxypurinol concentrations decreased by 26%, from mean 11.1 mg/l (95% CI 5.0–17.3) to mean 8.2 mg/l (95% CI 4.0–12.4) (p < 0.001); and renal oxypurinol clearance increased by 24%, from mean 12.7 ml/min (95% CI 9.6–15.8) to mean 16.1 ml/min (95% CI 12.0–20.2) (p < 0.05). The additional hypouricemic effect of probenecid 500 mg/day appeared to be lower in patients with renal impairment.
Conclusion.Coadministration of allopurinol with probenecid had a significantly greater hypouricemic effect than allopurinol alone despite an associated reduction of plasma oxypurinol concentrations. Australian Clinical Trials Registry ACTRN012606000276550.
Allopurinol is widely used for the treatment of hyperuricemia and gout. Allopurinol has a short half-life (1.1 ± 0.3 h) in blood and is rapidly metabolized to its active metabolite, oxypurinol, which has a considerably longer half-life (23 ± 7 h)1. Oxypurinol is largely responsible for the plasma urate reduction2,3. Current treatment guidelines for gout recommend maintaining plasma urate concentrations below 0.30 mmol/l4 to reduce the frequency of recurrent attacks of gout5,6 and to increase the rate of dissolution of tophi7,8.
Probenecid is an effective hypouricemic agent that inhibits active renal reabsorption of urate by the transporter URAT1 in proximal tubular epithelial cells9,10,11. In patients with renal impairment the linked hypouricemic and uricosuric effect of probenecid is reduced12,13,14,15.
Concomitant use of allopurinol and probenecid has been advocated in patients with tophaceous gout or for patients responding inadequately to monotherapy with allopurinol16,17. The rationale for the combination is that allopurinol inhibits the production of urate while probenecid increases the elimination of urate. However, there has been limited and somewhat conflicting data on the hypouricemic effect of this combination18,19,20. Probenecid has been shown to decrease plasma oxypurinol concentrations by 50% in healthy volunteers18, by increasing the renal clearance of oxypurinol21. However, despite this reduction of plasma concentrations of oxypurinol, studies in healthy volunteers18 and in patients with gout with adequate renal function (estimated creatinine clearance > 50 ml/min)19 have demonstrated a greater urate-lowering effect of the combination than use of either allopurinol or probenecid alone18, although the hypouricemic effect of the combination was less marked in another study that included gouty patients with renal impairment20.
We investigated the effects of the addition of probenecid on the plasma concentrations of urate and the pharmacokinetics of oxypurinol in patients with gout, and varying degrees of renal function, who were being treated with allopurinol.
MATERIALS AND METHODS
Study population
Patients aged ≥ 18 years with a confirmed diagnosis of gout (American Rheumatism Association criteria22) and who had been receiving allopurinol at a stable dose for at least 1 month were eligible for participation. They were recruited by referrals from rheumatologists on St. Vincent’s Hospital Sydney campus and advertisements in the hospital.
All patients provided written informed consent. The study was performed in accord with good clinical research practice standards and in accord with the Declaration of Helsinki, 1996. The study was approved by the St. Vincent’s Hospital Human Ethics Committee (H06/141) and registered in the Australian Clinical Trials Registry (ACTRN-01260-6000276550).
Study design
This was an observational open-label prospective clinical study conducted between April 2008 and August 2009 in patients with gout who were being treated with allopurinol.
Patients attended a screening visit, then a first or baseline visit if eligible and within 14 days of the screening visit. Subsequent visits were 1–3 weeks apart with the number of visits determined by the plasma concentrations of urate achieved up to a maximum of 5 visits. The last of these visits was designated the final visit, which was followed by an exit visit within 7 days.
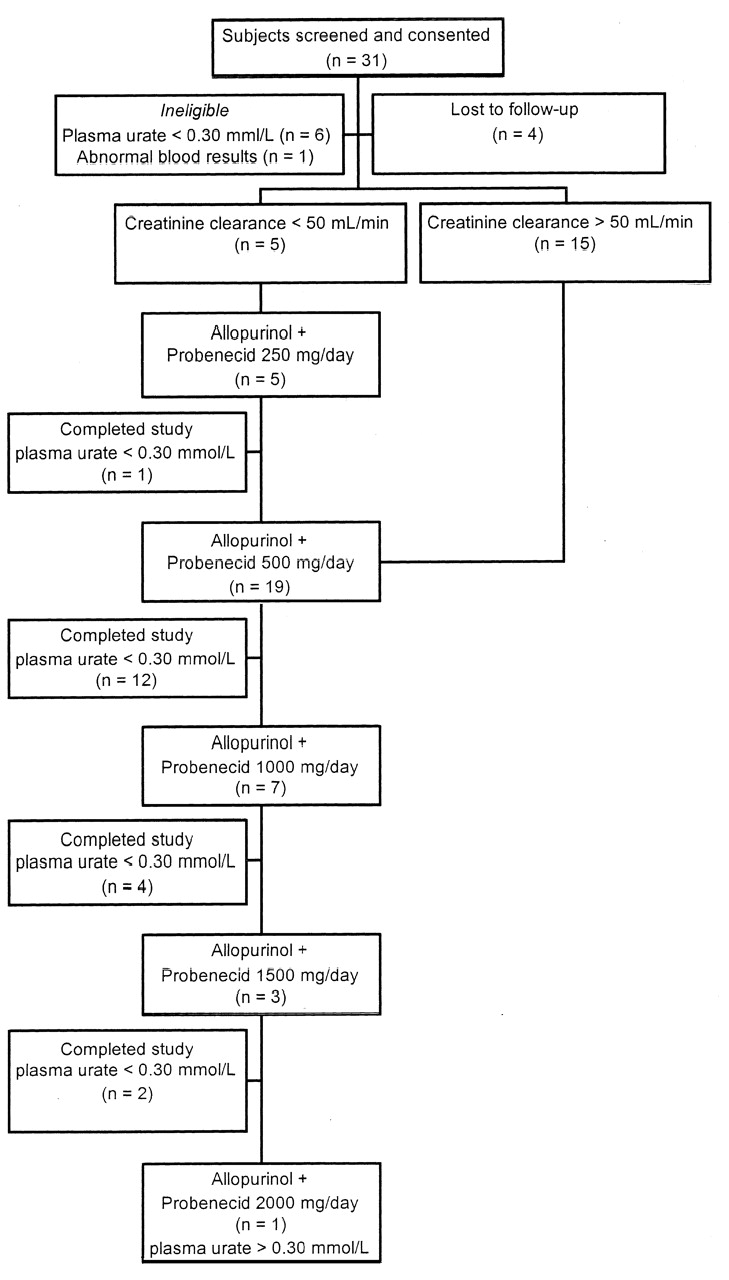
Patients continued their baseline, daily dose of allopurinol as prescribed by their referring physician throughout the study period. Daily doses of allopurinol ranged from 100 to 400 mg/day and all patients were dosed once daily. After the first visit patients were dosed to steady-state (minimum 7 days) with probenecid 250 mg twice daily or once daily if the patient’s estimated creatinine clearance was < 50 ml/min23 (Figure 1). This creatinine clearance cutoff was chosen as it identifies a subgroup of patients where most clinicians consider probenecid to be less effective, a view supported by most guidelines. The dose of probenecid was increased at intervals of 1 to 3 weeks to a possible maximum of 2 g daily or until plasma concentrations of urate were ≤ 0.30 mmol/l. Patients with severe tophaceous gout were included in the study and dosed with probenecid even if their plasma urate concentrations were ≤ 0.30 mmol/l because lowering the plasma urate as much as possible was considered to be good clinical practice. Concomitant low-dose colchicine 0.5 to 1.0 mg/day depending on renal function (n = 18) or a nonsteroidal antiinflammatory drug (naproxen, ibuprofen; n = 2) was prescribed for the duration of the study in all patients as prophylaxis against acute attacks of gout. Patients were allowed an unrestricted diet throughout the study but were asked to abstain from alcohol and caffeine-containing beverages for 12 h prior to each study visit.

Disposition of gout patients in the study and probenecid dosing rates.
A heparinized venous blood sample (8 ml) was obtained just before or at least 4 hours after the last dose of allopurinol. At each study visit (including screening and exit visits) patients provided a timed (2 h) urine collection, starting 1 hour prior to and finishing 1 hour after collection of the blood sample. Plasma was separated and stored at −20°C for analysis of urate, oxypurinol, and probenecid concentrations. Urine samples were collected for determination of oxypurinol, urate, and creatinine concentrations. Routine hematological, biochemical, and urine tests were conducted at the screening and exit visits. Patients were supplied with a diary to record time of dosing of all gout medications, including the intermittent use of medications for any joint pain. Dosing details of any concomitant medications were also recorded. After discharge from the study, a letter summarizing the patient’s study results and recommendations regarding their gout management was sent to their primary care physician. Any adverse effects were documented.
Oxypurinol and probenecid assays
Plasma concentrations of oxypurinol and probenecid were analyzed using validated high-performance liquid chromatography methods18. Concentrations of oxypurinol in urine were measured by LC-MS/MS24. Adherence was established by examining plasma drug concentrations.
Pharmacokinetic and pharmacodynamic analysis
Renal clearances of oxypurinol [CLR(OXY)], urate [CLR(UA)], and creatinine [CL(CR)] were calculated from the 2 h urine collections according to CLR = U.V/P, where U is urinary concentration (mmol/l), V is the rate of production of urine (ml/min), and P is the plasma concentration of the compounds (mmol/l). Creatinine clearance was also estimated using the Cockcroft-Gault equation based on lean body weight23. In order to account for renal function and its effects on renal clearance of urate and oxypurinol, the fractional renal clearances of urate (CLR(UA/CR)) and oxypurinol (CLR(OXY/CR)) were estimated from the quotient of their renal clearances and the renal clearance of creatinine for each participant. A fractional renal clearance of urate < 0.06 was considered low25. The mean steady-state plasma oxypurinol concentrations (Cav,ss) and apparent total-body clearance of oxypurinol (CL/F) were estimated using nonlinear mixed-effects modeling (implemented by NONMEM version 6.1.0; ICON Development Solutions, NONMEM 7 Project Team; Ellicott City, MD, USA) and a one-compartment pharmacokinetic model with first-order absorption and elimination.
Statistical analyses
All data are presented as means and 95% confidence intervals. Paired t tests or one-way analysis of variance tests with repeated measures were used to compare pharmacokinetic (oxypurinol disposition) and pharmacodynamic (plasma urate concentrations) data while taking allopurinol alone and the combination of allopurinol and probenecid (500 or 1000 mg/day). Statistical analyses were not conducted on the data from patients receiving 1.5 or 2 g probenecid daily because of low subject numbers in these groups. Statistical analyses were conducted using GraphPad version 5 software (GraphPad Software, San Diego, CA, USA).
RESULTS
Patient characteristics
Thirty-one gout patients taking allopurinol were screened and gave consent to enter the study, but only 20 of these patients went on to receive concomitant doses of probenecid as 6 had plasma urates < 0.30 mmol/l, 1 failed pathology screening, and 4 did not return for a second visit (Figure 1). All patients were male and allopurinol doses were 100 mg/day (n = 3), 200 mg/day (n = 4), 300 mg/day (n = 12), or 400 mg/day (n = 1) and all doses were taken once daily. Most patients were receiving other drugs, cholesterol-lowering drugs being the most common, and some took medicines known to affect plasma urate concentrations (Table 1). These concomitant medicines were continued without change of dose throughout the study period. Twelve patients had had gout for < 10 years; 2 patients reported having gout for over 20 years. Five patients had tophi. More than half the patients had experienced 2 or more acute attacks of gout in the previous 2 years, with 35% (n = 7) of patients experiencing more than 5 acute attacks of gout within this period, despite being prescribed allopurinol.
Characteristics of the gouty patients who received probenecid (n = 20).
Patients with renal impairment (estimated creatinine clearance < 50 ml/min) were started on a low dose of probenecid (250 mg daily, n = 5, Figure 1). One of these patients, who had tophaceous gout, had achieved the target plasma urate concentration of < 0.30 mmol/l before probenecid treatment but started probenecid because even lower plasma urate concentrations were considered beneficial. The remaining 4 patients progressed to higher doses of probenecid. Thus, of the 20 patients who received the combination, 19 received 500 mg probenecid daily in addition to their fixed dose of allopurinol (Figure 1). Seven of these patients failed to achieve target plasma urate concentrations and, therefore, received higher doses of probenecid (1000 mg/day). The dose of probenecid was increased to 1500 mg/day in 3 of these patients and 1 patient failed to achieve the target plasma urate concentration on the maximal allowed dose of probenecid, 2 g daily. The increments in plasma oxypurinol and probenecid concentrations with all doses of medicines suggested our patients were adherent to their therapy.
Pharmacokinetics of oxypurinol
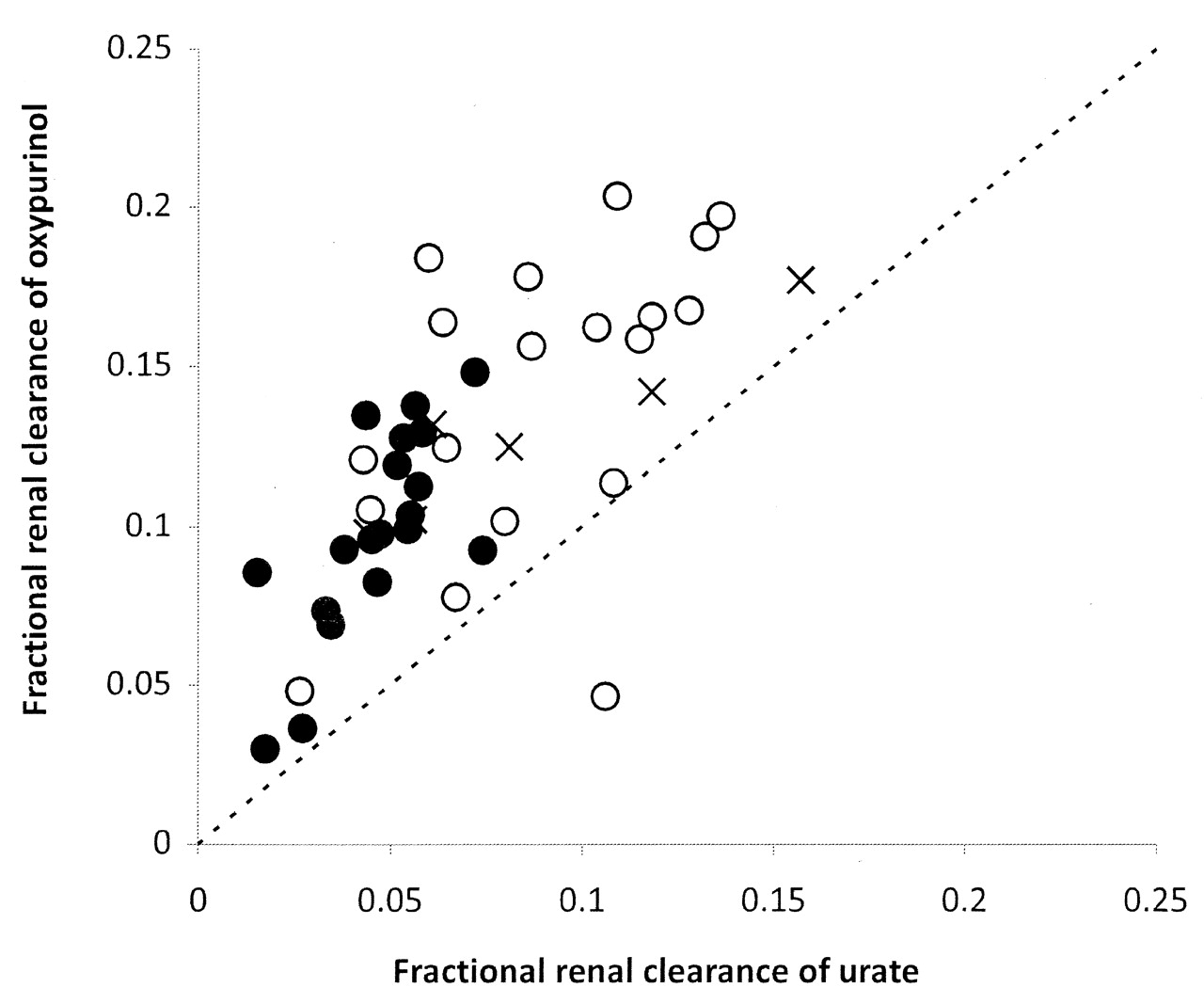
The addition of probenecid 500 mg/day to allopurinol therapy significantly decreased the average steady-state oxypurinol concentrations by 26% compared to allopurinol alone (Table 2). This is because probenecid significantly increased the apparent total, renal, and fractional renal clearances of oxypurinol by 35%, 27%, and 40%, respectively (Table 2). Doubling the dose of probenecid to 1000 mg daily (n = 7) did not alter the plasma concentrations of oxypurinol further when compared to the coadministration of allopurinol and 500 mg probenecid daily. However, the apparent, renal, and fractional renal clearances of oxypurinol increased by a further 8%, 27%, and 20%, respectively. The fractional renal clearances of oxypurinol and urate were highly correlated (p < 0.001, r2 = 0.52; Figure 2).

Relationship between the fractional renal clearance of oxypurinol and urate (p < 0.001, r2 = 0.52). Closed circles represent allopurinol monotherapy, open circles allopurinol coadministered with probenecid (500 mg daily); crosses represent allopurinol coadministered with probenecid (1000 mg daily). Broken line represents the line of unity.
Pharmacokinetics of oxypurinol and the pharmacodynamic effects of allopurinol alone or with probenecid for at least 7 days (500 or 1000 mg/day) in patients with gout. Data are mean (95% CI).
In 1 patient, the concentrations of probenecid at 1000 mg and 1500 mg daily were lower than at 500 mg daily probenecid, indicating poor adherence. Otherwise the plasma probenecid concentrations for individuals across the doses of probenecid they received rose with dose, as expected (data not shown).
Pharmacodynamics
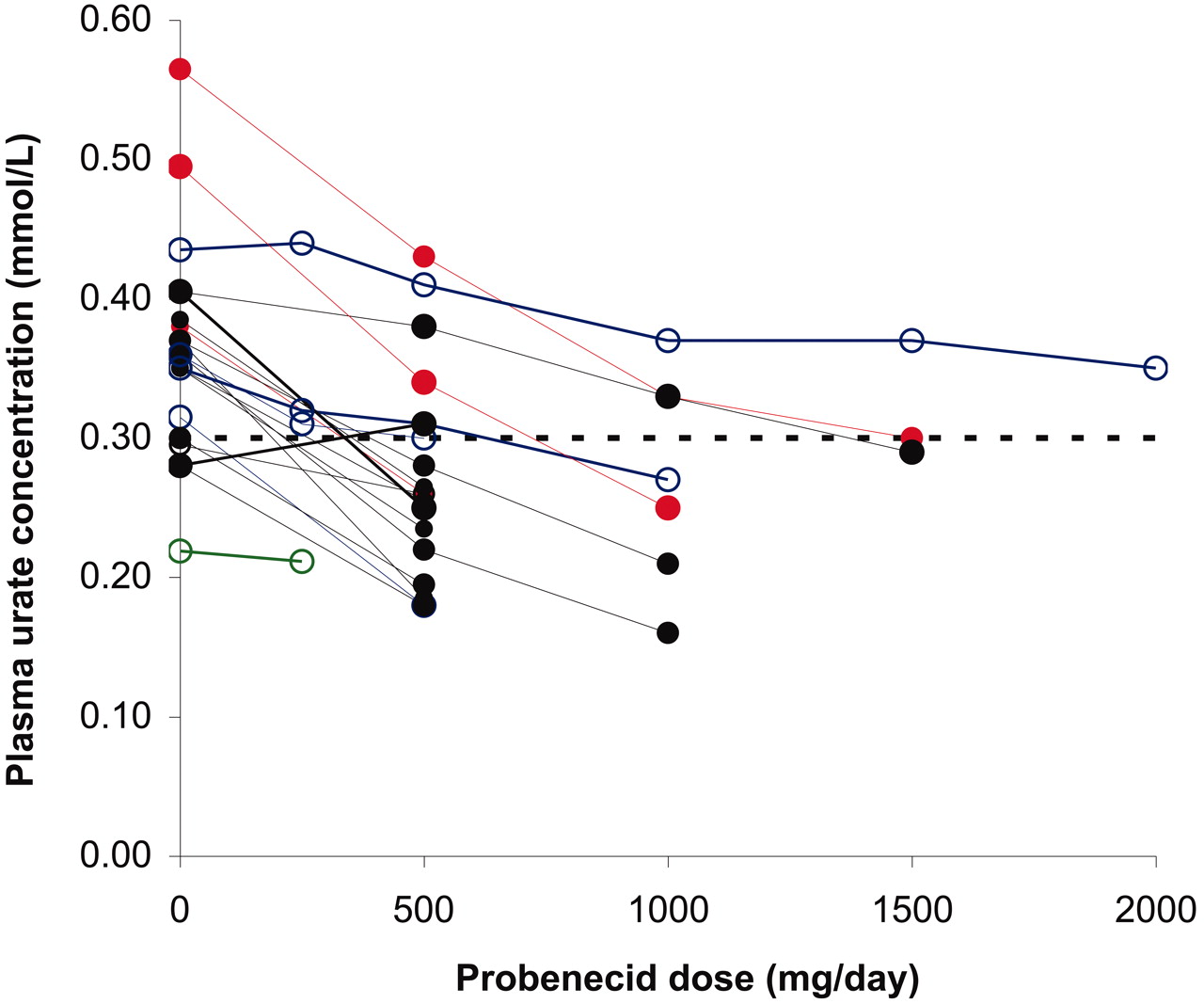
Overall, the plasma concentrations of urate decreased by 25% with the addition of probenecid (Table 2); the exception was 1 patient with tophaceous gout whose plasma urate increased slightly with addition of probenecid 500 mg/day (Figure 3). In 1 other patient, plasma concentrations of urate did not fall below 0.30 mmol/l despite adequate plasma concentrations of probenecid and oxypurinol. Patients with renal impairment (n = 5) showed similar reductions in plasma urate concentrations with the increases in probenecid dose compared to those with relatively good renal function (Figure 3). For the majority of patients (n = 12), the target plasma concentration of urate was reached with 500 mg probenecid per day. Seven patients received doses of probenecid > 500 mg daily. These patients had higher plasma urate concentrations during allopurinol monotherapy [mean 0.42 mmol/l (95% CI 0.35–0.50)] compared to patients who required only up to 500 mg probenecid daily [n = 13; mean 0.34 mmo/l (95% CI 0.31–0.37)] (p < 0.01).
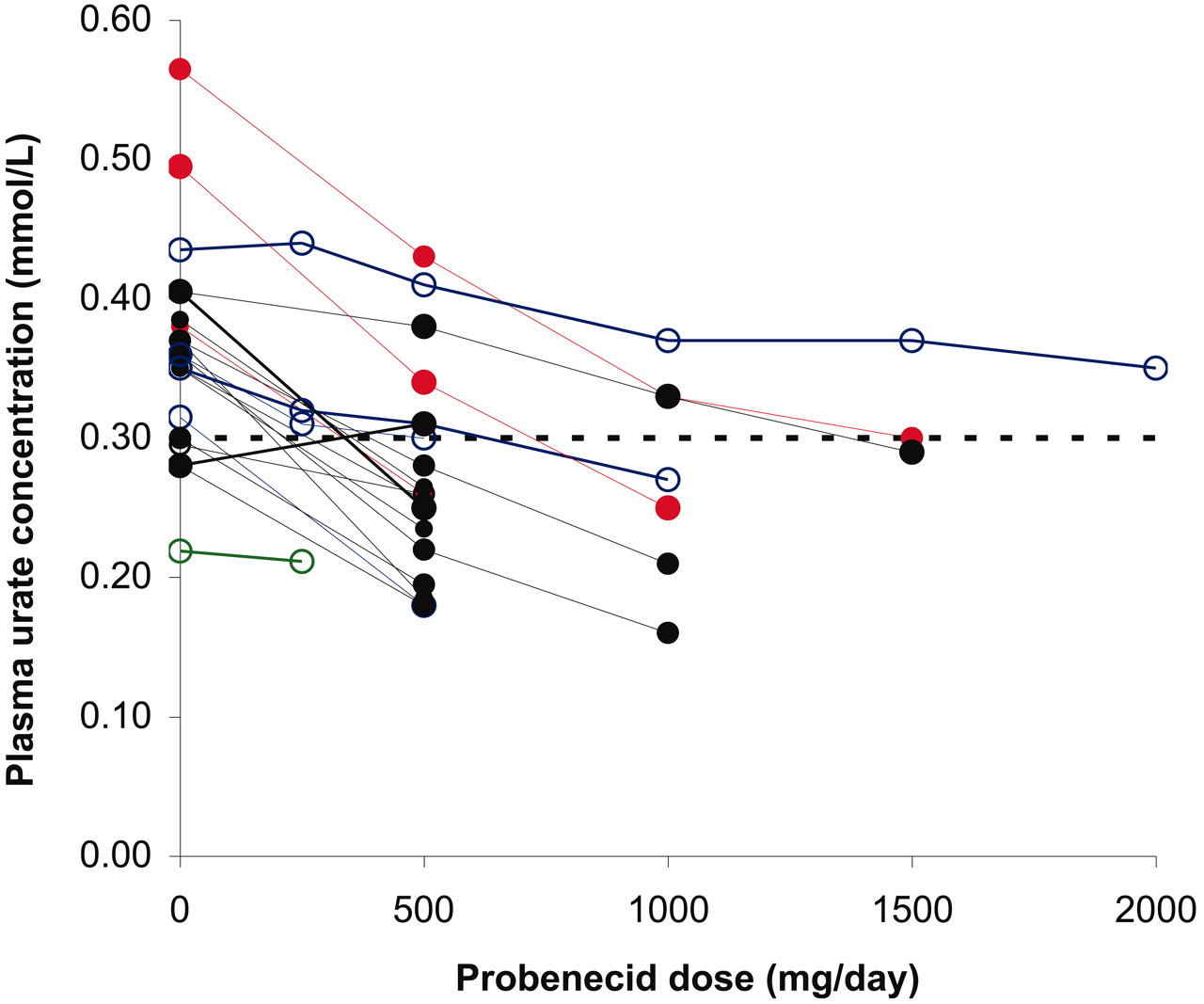
Plasma concentrations of urate in gouty patients (n = 20) during allopurinol monotherapy and with the addition of increasing doses of probenecid. Open symbols represent patients with creatinine clearance < 50 ml/min; closed symbols, patients with creatinine clearance > 50 ml/min. Allopurinol doses range from 100 to 400 mg/day: red, 100 mg/day; blue, 200 mg/day; black, 300 mg/day; green, 400 mg/day. Probenecid doses ranged from 250 to 2000 mg/day. Broken line represents the target plasma urate concentration of 0.30 mmol/l.
Consistent with the decreased plasma concentrations of urate, probenecid 500 mg/day increased the renal clearance of urate by 62% and the fractional renal clearance of urate by 91%. The reduction in plasma concentrations of urate was somewhat less than expected given the increase in the fractional renal clearance of urate. For patients who received both 500 mg and 1000 mg of probenecid daily (n = 7), the plasma concentrations of urate decreased by 21% and 37%, respectively, compared to allopurinol monotherapy. Correspondingly, the fractional renal clearance of urate increased by 57% and 60%, respectively. Interestingly, the fractional renal clearance of urate was less than 0.06 in the majority (68%) of patients in this study, indicative of the low urate clearance phenotype25.
No patient in this study reported an adverse event; in particular, no attacks of acute gout were reported.
DISCUSSION
In this study, concomitant probenecid reduced plasma concentrations of urate below 0.30 mmol/l in all but one of these 20 patients with gout. This is consistent with work in healthy volunteers18,21 and other patients with gout26. We found that probenecid 500 mg/day was sufficient in 12 of the 20 patients, and that those patients with higher plasma urate concentrations during allopurinol monotherapy required higher doses of probenecid. We also found that probenecid was effective in our few patients with renal impairment (creatinine clearance < 50 ml/min).
The reductions in plasma urate concentration occurred despite the significant fall in plasma concentrations of oxypurinol due to the probenecid-induced increase in the renal clearance of oxypurinol. Thus the uricosuric effect of probenecid more than compensates for the probenecid-induced reduction in plasma concentrations of oxypurinol, consistent with our observations in healthy volunteers18. Our results are also consistent with studies of the combination of allopurinol and another uricosuric agent, benzbromarone, which also added to the hypouricemic effect of allopurinol, despite decreasing the plasma concentrations of oxypurinol21,27,28,29,30.
The probenecid-induced increase in the renal clearance of both oxypurinol and urate is almost certainly due to inhibition of the reabsorption of the 2 compounds by the renal transporter URAT1. URAT1 is inhibited by probenecid and both urate and oxypurinol are substrates for URAT19,31 consistent with their similar chemical structures. The linear relationship between the fractional renal clearances of urate and oxypurinol (Figure 2) is also consistent with URAT1 being the major transporter of urate and oxypurinol.
The 25% and 37% average decrease in the plasma concentrations of urate with addition of probenecid at 500 mg and 1000 mg daily, respectively, to a stable allopurinol dosing regimen is similar to that reported by others. Reinders, et al19 found that coadministration of allopurinol and probenecid (1000 mg daily) in gouty patients with reasonable renal function (glomerular filtration rate > 50 ml/min) decreased plasma urate concentrations by a further 33% compared to allopurinol alone. By contrast, Yu, et al20 reported only 10% reduction in plasma urate concentrations with the addition of probenecid to allopurinol therapy in patients with tophaceous gout. However, many of their patients had impaired renal function, which may explain the reduced hypouricemic effect of probenecid observed by these and other investigators13,32. Only a small proportion of our patients (n = 5) had creatinine clearances below 50 ml/min. Nevertheless we observed an effect of concomitant probenecid in these 5 patients, albeit somewhat diminished relative to those with better renal function.
A notable finding of our study was that the decrease in plasma concentrations of urate with the combination was less than predicted from the nearly 2-fold increase in the fractional renal clearance of urate (Table 2). The renal clearance of urate accounts for only two-thirds of its total clearance, the remaining one-third being cleared by the gastrointestinal tract33. By contrast, the decrease in plasma concentrations of oxypurinol was consistent with the changes observed in the fractional renal clearance of oxypurinol, suggesting that renal clearance accounts for the majority of its total clearance1.
The patients participating in this study generally had been diagnosed with gout within the last decade and were not well controlled on allopurinol alone. Tophaceous deposits and acute attacks of gout were common. Patients commonly stated that they had missed an “occasional” dose of allopurinol prior to participation in this study whereas others described taking allopurinol “holidays.” In this cohort, the first step to better outcomes would be to optimize the use of allopurinol and more consistent adherence to the drug.
There are a number of possible approaches to reducing plasma urate concentrations to satisfactory levels in patients already taking allopurinol. Improving the adherence of the patient to allopurinol therapy is the first option. The next is to increase the dosage of allopurinol, above 300 mg/day if necessary, until target plasma concentrations of urate are achieved. Despite concerns that this approach may increase the chance of hypersensitivity reactions to the drug34, other researchers have demonstrated that escalation of allopurinol dosage can be instituted safely and most patients can be treated successfully35,36. This approach is preferred as it is effective, safe, and less complicated for the patient. Another approach is to coprescribe probenecid (or benzbromarone if available) in addition to allopurinol to enhance the hypouricemic effect. Some rheumatologists select this approach when gout is not controlled or tophi are present. Although the combination has greater hypouricemic efficacy there are disadvantages. A second medication that is usually taken twice daily is a further challenge for patient adherence37,38. Another approach would be to use an alternative hypouricemic drug. Uricosuric monotherapy is efficacious if the patient does not have significant renal impairment. The new xanthine oxidase inhibitor febuxostat, which has similar efficacy to allopurinol if dosage of the latter is optimized, can be used. Although febuxostat is expensive and not available in a number of countries, it is a useful alternative if the patient is intolerant of allopurinol39.
We did not investigate the effect of oxypurinol on the pharmacokinetics of probenecid in detail. However, studies in healthy volunteers18 and hypertensive gouty patients17 clearly demonstrated that the addition of allopurinol to probenecid does not influence the pharmacokinetics of probenecid.
Our study demonstrated a significant pharmacokinetic and pharmacodynamic interaction between oxypurinol, the active metabolite of allopurinol, and probenecid. Coadministration of allopurinol and probenecid had a greater hypouricemic effect in gouty patients than allopurinol alone. Patients with renal impairment may still benefit from addition of probenecid to background treatment with allopurinol. This study, along with that of Reinders, et al19, establishes an additional treatment option for patients whose plasma urate concentrations are responding inadequately to allopurinol alone.
Acknowledgment
The authors thank Louise Greenup for help with patient recruitment and study visit coordination. They also thank the medical personnel involved in the study including Dr. Mona Manghani, Dr. Ed Park, Dr. Minh Duong, and Dr. Kevin Maruno.
Footnotes
-
Supported by an Arthritis Australia National Research Grant and a NH&MRC Program Grant 568612.
- Accepted for publication December 8, 2010.








{kind=link}
{kind=link}
{kind=link}