Article Text

Abstract
Aim: Severe uveitis is potentially associated with visual impairment or blindness in young patients. Therapeutic strategies remain controversial. The efficacy of interferon alpha-2a (IFN-α2a) in severe uveitis, refractory to steroids and conventional immunosuppressive agents, was evaluated.
Patients and methods: Patients were included after a major relapse of uveitis following corticosteroids and immunosuppressants. IFN-α2a (3 million units three times a week) was administered subcutaneously. Efficacy was assessed by improvement in visual acuity, decrease in vitreous haze, resolution of retinal vasculitis and macular oedema, assessed by fundus examination and fluorescein angiography, and decrease in oral prednisone threshold.
Results: 45 patients were included. Median age was 32.3 years (range 8–58) and sex ratio (F/M) was 0.66. Uveitis was associated with Behçet’s disease in 23 cases (51.1%) and with other entities in 22 cases (48.9%). Median duration of uveitis before interferon therapy was 34.9 months (range 3.4–168.7) and an average of 3.26 relapses following corticosteroids and immunosuppressants was noted. Uveitis was controlled in 82.6% of patients with Behçet’s disease and 59% of patients with other types of uveitis (p = 0.07). During a mean follow-up of 29.6 months (range 14–55), median oral prednisone threshold decreased significantly from 23.6 mg/day (range 16–45) to 10 mg/d (range 4–14) (p<0.001). Interferon was discontinued in 10 patients (22.2%) with Behçet’s disease and in four patients without Behçet’s disease. Relapses occurred in four and one cases, respectively.
Conclusions: Interferon therapy appears to be an efficient strategy in severe and relapsing forms of Behçet’s disease but also in other uveitic entities. However, it seems to act more to suspend rather than cure the disease. Therefore, IFN-α2a may be proposed as a secondline strategy after failure of conventional immunosuppressants.
- IFN-α2a, interferon alpha-2a
- logMar, logarithm of the minimum angle of resolution
- TNF, tumour necrosis factor
Statistics from Altmetric.com
- IFN-α2a, interferon alpha-2a
- logMar, logarithm of the minimum angle of resolution
- TNF, tumour necrosis factor
Conventional treatment of inflammatory disorders involving the posterior segment of the eye remains a challenging issue for ophthalmologists.1 Steroids remain the cornerstone, associated with immunosuppressive agents in cases proven to be highly steroid dependent. Recent results with anti-tumour necrosis factor (TNF) agents highlight their significant, but transient, efficacy with potential side effects.2 Interferon alpha-2a (IFN-α2a) seems to be an alternative to anti-TNF drugs. Its efficacy and tolerance have been analysed in patients with Behçet’s disease.3–5 Uveitis is one of the most severe complications of the disease. As many as 50% of patients with ocular involvement became legally blind within 5 years after the onset of symptoms in the 1980s.6 The prognosis has improved in recent years with the increasing use of steroids and immunosuppressive agents.7 Based on our experience, the percentage of eyes with a visual acuity less than 20/200 showed limited progression from 14% to 16% in patients with Behçet’s disease receiving sustained therapy with a mean follow-up of 6 years.8 Nevertheless, in a few cases uveitis remains refractory to conventional therapy. Recent reports seem to emphasise the efficacy and tolerance of IFN-α2a in this group of patients.9–12 Other types of chronic uveitis often require corticosteroids and immunosuppressants. We have previously reported on the potential complications and the visual outcome of patients with chronic severe uveitis.13 As in Behçet’s disease, these alternatives are sometimes inefficient and side effects may occur during treatment. Our preliminary encouraging results obtained with IFN-α2a in Behçet’s disease9 led us to enlarge the use of interferon to other chronic uveitic entities.
PATIENTS AND METHODS
The clinical records of patients presenting with severe and chronic uveitis and referred to the Ophthalmology and Internal Medicine Departments of the Pitié-Salpêtrière Hospital, Paris, France, between February 1995 and November 2001, for therapeutic management with interferon alpha 2a, were retrospectively reviewed. To be included, patients had to present with one of the following conditions: Behçet’s disease (according to the International Study Group’s classification criteria),14 pars planitis,15 Vogt–Koyanagi–Harada disease (according to criteria proposed by the American Uveitis Society),16 other idiopathic panuveitis, uveo-papillitis or retinal vasculitis. All patients had clinical evidence of sight threatening intermediate, posterior or panuveitis, resistant to different types of immunosuppressants or requiring sustained high doses of steroids. An extensive work-up was performed in all cases to confirm the aetiology of uveitis and, in particular, to exclude an infectious condition requiring a specific strategy as a firstline therapy.
Clinical and laboratory findings of all patients were analysed both by ophthalmologists and internists before final inclusion into the protocol. Patients with sarcoidosis were not included because of the potential risk of worsening disease associated with IFN-α. Fertile women not using contraception, pregnant women, and patients with evidence of active infection, blood abnormalities, liver function abnormalities, mental disorders or other serious medical diseases were also excluded.
Ophthalmological screening
Patients were regularly followed in both the Ophthalmology and Internal Medicine Departments. Ophthalmological examination included measurement of the best corrected visual acuity, tonometry and slip-lamp examination. Funduscopy was performed to assess vitritis (grading of vitreous haze according to the Nussenblatt classification),17 pars planitis, retinal haemorrhages, vasculitis, papillitis and retinal ischaemia. Fluorescein angiography was performed in all cases. Laboratory tests, including blood cell counts, liver transaminases, antithyroperoxidase antibodies and thyroid stimulating hormone measures were performed at regular intervals.
Treatment
Initiation of IFN-α2a therapy was performed during a short hospitalisation. Patients received 3 million units of IFN-α2a (Roferon; Roche, Neuilly-Sur-Seine, France) subcutaneously three times a week. Interferon therapy was always initiated in association with intravenous pulses of methylprednisolone over 3 days followed by oral prednisone (1 mg/kg/day). Doses of steroids were tapered based on clinical improvement of uveitis and were always started 1 month after initiation of IFN-α2a. All other immunomodulating therapies were discontinued when IFN-α2a was introduced. However, colchicine and topical steroids were allowed. Oral paracetamol was administered to prevent IFN-α2a induced fever or flu-like symptoms.
The steroid threshold was evaluated according to the dose which, if tapered, led to relapse. After 1 month of IFN-α2a therapy, if no improvement was observed, the dose of IFN-α2a was increased to 6 million units three times per week. If no improvement occurred within 2 months, we concluded that treatment was a failure, and a new immunosuppressive strategy was proposed. Likewise, if two severe inflammatory relapses occurred during IFN-α2a treatment, or if steroids could not be tapered, we concluded that interferon therapy was a failure. Uveitis associated with a decrease in visual acuity below 20/100, increase in vitreous haze ⩾2+, relapse of cystoid macular oedema or serous retinal detachment was defined as severe. Treatment was also interrupted in the event of poor compliance, if supervision was not correctly performed or if adverse events occurred.
Based on the criteria recently reported by the Standardisation of Uveitis Nomenclature Working Group, improved activity was defined as a two step decrease in the level of inflammation or decrease to grade 0.18 Evolution of visual acuity, control of intraocular inflammation (regression of retinal vasculitis and macular oedema) and levels of steroid dependence were evaluated as major criteria for drug efficacy.
The paired sample Student’s t test was used to compare mean corticosteroids doses and levels of visual acuity before interferon therapy compared with the end of the follow-up period. Visual acuity was transformed to the logarithm of the minimum angle of resolution acuity (logMar). The Mann–Whitney U test was used to compare visual acuities. A p value <0.05 was considered statistically significant.
RESULTS
Patients
Forty five patients were included in this retrospective study. Median age was 32.3 years (range 8–58) and sex ratio (F/M) was 0.66. Extraocular symptoms are reported in table 1. All patients had a chronic severe, intermediate, posterior or panuveitis. For 23 of the patients (51.1%), a diagnosis of Behçet’s disease was made according to the International Study Group’s classification criteria. The aetiological distribution of the other 22 patients (48.9%) is reported in table 2.
Demographic characteristics and extraocular symptoms of the study population
Characteristics of uveitis prior to interferon therapy
Characteristics of uveitis
Ocular disease was bilateral in 41 of 45 patients (91.1%), representing 86 eyes. Chronic macular oedema and signs of retinal vasculitis were observed in 60.5% and in 87% of cases, respectively (table 2). Before interferon therapy, median duration of uveitis was 32.9 months (range 3.4–168.7), and an average of 3.26 relapses was noted (range 1–9). Visual acuity was evaluated before initiation of therapy and at the last follow-up (or at the end of treatment if it had to be interrupted due to failure). Mean initial visual acuity was 0.5 logMar (20/63). It was below 20/40 in 43 eyes (50%) and below 20/100 in 25 eyes (29.1%). Before initiation of IFN-α2a, all patients had received oral corticosteroids: 32 (71.1%) had intravenous pulses of methylprednisolone initially (mean 2.9 series of pulses per patient, consisting of three daily pulses per series). Immunosuppressants were previously used in 35 cases (77.7%) (table 3). A mean of two immunosuppressive regimens had failed before initiation of interferon therapy. Conventional treatment was followed for a mean period of 14 months before administration of IFN-α2a.
Therapeutic management before interferon therapy
Efficacy
After 4 weeks of treatment, based on clinical and imaging findings, we concluded that IFN-α2a was effective in 40 patients (88.9%). Five patients did not respond well to initial and then double doses of interferon, leading to rapid initiation of another immunosuppressant. Three patients who initially responded well to IFN-α2a were lost of follow-up. Of 37 patients who were monitored regularly until the end of the study, and who were initially good responders, five had more than two relapses during the treatment (fig 1). We considered that IFN-α2a had no or only partial efficacy in these patients. Two responders had one relapse during interferon treatment motivating an increase in dosage (6 million units, three times a week). Therefore, IFN-α2a was regarded as effective (grade 0–1 cell/inflammatory lesions) in 32 cases (71.1%) (ie, 19/23 with Behçet’s disease (82.6%) and 13/22 with other uveitic conditions (59%); p = 0.07). Among responders, control of retinal vasculitis and cystoid macular oedema was achieved in 36/38 and 20/22 eyes with Behçet’s disease (p<0.001), and in 18/22 and 14/16 eyes with other uveitic conditions (p<0.001). During a mean follow-up of 29.6 months (range 14–55), global visual acuity progressed from 0.5 logMar before treatment to 0.35 logMar after (p = 0.07). Median oral prednisone threshold significantly decreased from 23.6 mg/day (range 16–45) to 10 mg/day (range 4–14) at the end of follow-up (p<0.001).

{kind=link}
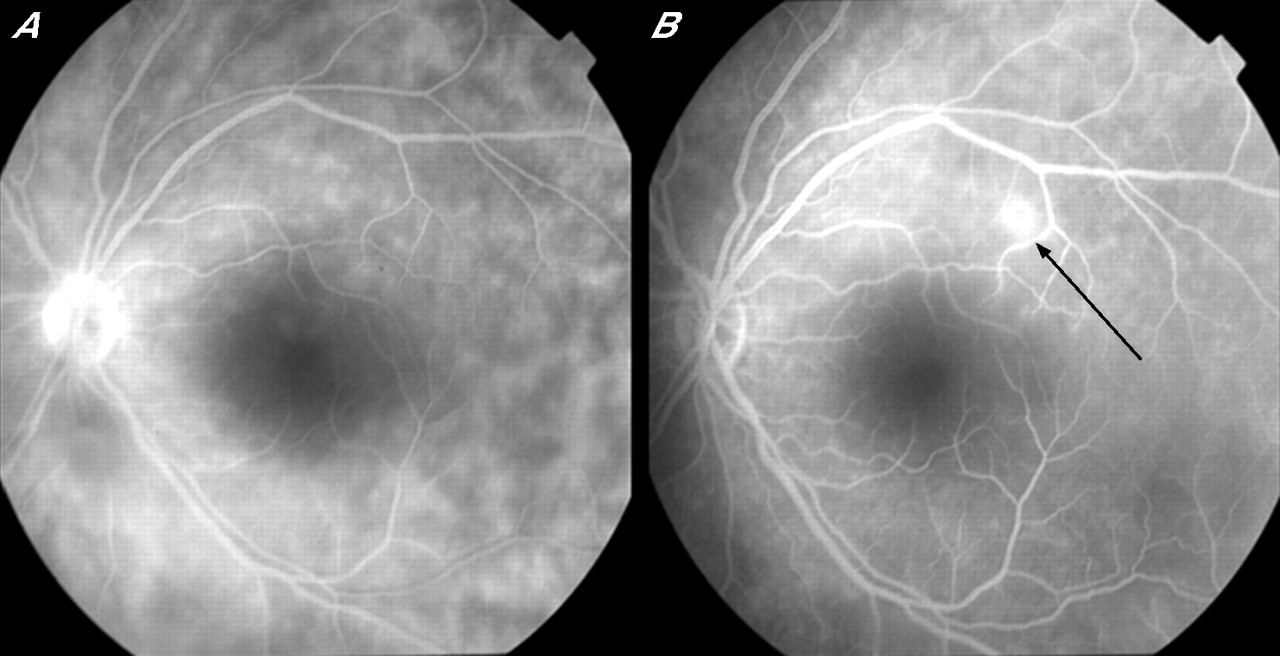
(A) Fluorescein angiography showing diffuse retinal choriocapillaropathy and papillitis in a patient with Behçet’s disease before interferon α2a (IFN-α2a) therapy. (B) Initial efficacy of IFN-α2a followed by moderate relapse of necrotising retinitis (arrow) occurring after major corticosteroid tapering despite maintenance interferon therapy.
In the group of patients with Behçet’s disease (group I), 19/23 responded to interferon therapy. During a median follow-up of 30 months (range 18–59), global visual acuity progressed from 0.45 to 0.3 logMar (p = 0.06). Mean oral prednisone threshold decreased significantly from 20.8 to 9.7 mg/day at the end of follow-up (p<0.001). Of the 38 eyes evaluated, 29 (76.3%) had stabilisation or improvement in visual acuity at the end of follow-up. Improvement was superior to two lines of visual acuity in 51.4% of cases.
Results were less spectacular in the group of 22 patients with uveitis unrelated to Behçet’s disease (group II). As in the Behçet’s disease group, ocular inflammation was resistant to initial conventional strategies as 85% of patients had an immunosuppressive treatment and 95% had corticosteroids. Despite previous associations, all patients had at least two severe (mean 3.8) inflammatory relapses during the course of disease (mean 43 months) before inclusion in the interferon protocol. After a median follow-up of 24 months (range 12–39), IFN-α2a was considered effective in 59% of patients (p = 0.07 compared with Behçet’s disease). All non-responders among non-Behçet’s disease uveitis patients had idiopathic panuveitis or posterior uveitis. The mean corticosteroids threshold was tapered from 25.6 to 10.5 mg/day. Of the 26 eyes evaluated, 17 (65.4%) had stabilisation or improvement in visual acuity at the end of follow-up. Improvement was superior to two lines of visual acuity in 49% of cases. Mean visual acuity progressed from 0.55 logMar initially to 0.4 logMar at the end of follow-up (p = 0.06) (table 4). The rate of relapse during interferon treatment was 0.3%/person-year in group I and 2%/person-year in group II.
Final outcome of patients treated with interferon alpha
Interruption and monitoring after discontinuation of IFN-α2a
Discontinuation was decided after at least a 9 month period of complete remission. Interferon was stopped in 10 of 19 responders with Behçet’s disease (52.6%) after a mean treatment period of 30.6 months (range 14–50). The mean follow-up of these 10 patients from IFN-α2a withdrawal was 18.5 months (range 12–25). Relapses occurred in four cases (40%) after a mean delay of 4 months (range 2–6). Reintroduction of IFN-α2a was effective in all cases with an initial increase in steroid doses. In the group of non-Behçet’s disease patients, treatment was interrupted in four of 13 responders (30.7%) after a mean follow-up of 24.2 months (9–27). One patient had a relapse after 5 months but the others experienced no relapse.
Side effects
Of 45 patients who received interferon therapy, 2 (5.13%) had major side effects. One suffered from severe depression leading to permanent discontinuation of IFN-α2a after 3 weeks of treatment. The other developed major neutropenia after 8 weeks, leading to temporary interruption. Low dose IFN-α2a was reinitiated after normalisation of blood cell count. Apart from flu-like syndrome, almost constant at initiation of therapy, few minor clinical side effects were observed in other patients and they never led to treatment discontinuation (ie, depression requiring therapy (n = 2), and coughing, arthralgias, thyroiditis and Raynaud’s phenomenon (n = 1 each)). Except for one case of non-ischaemic optic neuritis, no ocular side effects occurred. In this case, interferon was discontinued and resolution was achieved after high dose methylprednisolone pulses. Within minor biological abnormalities, 13 patients (28.9%) had mild/moderate changes in blood cell counts and five patients (11.1%) had mild/moderate elevation of liver enzymes.
DISCUSSION
Recent publications have reported on the relevance of IFN-α2a in Behçet’s disease when used alone or associated with steroids and/or immunosuppressants.10,19–22 Initial treatment modalities (ie, doses ranging from 3 to 9 million units per injection and daily versus three times a week regimens) as well as duration of IFN-α2a administration vary widely among published studies. Kotter et al recently reported on the importance of rapid corticosteroid tapering after initiation of interferon therapy.23 Our approach was different, based on the potential severity of relapsing uveitis. Therefore, corticosteroid tapering was not initiated during the first month. Efficacy usually becomes obvious between 3 and 8 weeks after initiation. As with other treatments for patients with uveitis, IFN-α does not seem to have a frequent curative effect. Severe relapses occurred in 40% of our patients with Behçet’s disease after IFN-α2a discontinuation. In a major study,10 20 of 50 patients (40%) were reported as off treatment and disease free for a mean duration of 29.5 months after a mean observation period of 36.4 months (range 12–72). Initial interferon doses used in our study were relatively low compared with those proposed by other authors. However, the good initial response9 and the low rate of side effects observed during follow-up led us continue the same procedure. Whether the importance of interferon dose may influence the final visual outcome of patients remains to be seen.
IFN-α2a may be used as a secondline strategy in Behçet’s disease. It may or may not be associated with other immunosuppressive agents, such as azathioprine.24 The optimum duration of IFN-α2a administration remains to be determined. Finally, when interferon itself fails to improve ocular symptoms, new molecules, such as anti-TNF-α seem to be appropriate.25–29 Long term data and controlled studies are needed before drawing further conclusions about the firstline use of these compounds.
The mechanism of action of IFN-α in patients with uveitis is complex and multifactorial. Some of these aspects have been analysed recently.30,31
Based on encouraging results in patients with Behçet’s disease, we have enlarged our therapeutic strategy to other forms of severe uveitis, in particular cases of panuveitis and retinal vasculitis, disclosing aspects closely related to those observed in Behçet’s disease.
Even though case reports and small case series have been published on the efficacy of IFN-α in patients with serpiginous choroiditis, familial panuveitis or HHV-8 associated uveitis,32–34 this retrospective study included a larger number of patients.
We encountered side effects commonly reported in the literature. Flu-like syndrome was observed most frequently during the first weeks of therapy. The number of patients who developed leucopenia or thrombocytopenia was important (28.9%). However, side effects remained moderate and disappeared after dose tapering, as reported by others.35 A few cases of agranulocytosis and bone marrow fibrosis have been described.36,37 No case of interferon associated retinopathy was observed in this series. This complication has been described in patients treated for hepatitis C38,39 or for melanoma.40 We reported a case of unilateral non-ischaemic optic neuropathy after IFN-α2a which improved after interferon discontinuation and high dose corticosteroids. This is different from those usually associated with interferon therapy.41,42
These results confirm previous reports on the efficacy and safety of interferon therapy in patients with Behçet’s disease but also in other forms of severe posterior or intermediate uveitis. However, we remain cautious about the efficacy and side effects of this therapeutic strategy obtained in a limited case series. Controlled studies are necessary to identify the role of this immunomodulatory agent in the therapeutic arsenal, especially its optimum dose and duration of administration.
Acknowledgments
BB and GG collected all of the data, analysed the data and wrote the paper. BB, BW, NC, DLTH, CL, CF, PL and JCP were in charge of the patients, reviewed the charts, and gathered and collected the data.
REFERENCES
Footnotes
-
Competing interests: None.
-
Published Online First 18 October 2006
Linked Articles
- BJO at a glance