Article Text

Abstract
A group of therapies with exciting potential has emerged for children and young people with severe juvenile idiopathic arthritis (JIA) uncontrolled by conventional disease modifying drugs. Theoretical understanding from molecular biologic research has identified specific targets within pathophysiological pathways that control rheumatoid arthritis (RA) and JIA. This review identifies the pathways of autoimmunity to begin to show how biologic agents have been produced to replicate, mimic, or block culpable molecules and so promote or inhibit cellular activity or proliferation. Of these agents, cytokine antagonists have shown greatest promise, and early clinical studies of tumour necrosis factor (TNF) blockade have identified dramatic clinical benefit in many children with JIA. However, as will also be discussed, overlap of pathways within a complex immune system makes clinical response unpredictable and raises additional ethical and administrative concerns.
- IL, interleukin
- JIA, juvenile idiopathic arthritis
- RA, rheumatoid arthritis
- TNF, tumour necrosis factor
Statistics from Altmetric.com
- IL, interleukin
- JIA, juvenile idiopathic arthritis
- RA, rheumatoid arthritis
- TNF, tumour necrosis factor
Juvenile idiopathic arthritis (JIA) affects 1 in 1000 children.1 For the majority of children with polyarticular disease, methotrexate2–4 and other second line agents5 have improved the prognosis of the disease. However, a significant number of children, who do not respond adequately to conventional management, experience severe and aggressive disease, compounded by the cumulative side effects of long term medication that often includes steroids. Such disease activity results in chronic pain and stiffness, irreversible joint damage, possibly requiring joint replacement, growth retardation, and notable functional disability. There is also a significant impact on emotional and psychological development, lifestyle, and employment.6,7 Biologic therapy is currently targeted at this group of vulnerable patients.
AUTOIMMUNITY
Autoreactivity is the failure of B and T cells, pivotal to the immune response, to differentiate between foreign and self antigen; autoimmune diseases are the result of the ensuing tissue damage. Current understanding acknowledges that a low level of autoreactivity is crucial to normal immune function,8 including the survival of naïve T and B cells and establishment of a repertoire of mature lymphocytes following exposure to autoantigens.9,10 However, since there is no fundamental difference between the structure of self and foreign antigen, differentiation requires alternative strategies and is thought to depend on the microenvironment of antigen presentation governed by the lymphocyte, inflammatory proteins, or cytokines, and antigen presenting cells, such as dendritic cells and macrophages.11–13
The chronic arthridies are generally considered to be T cell mediated,14 although the contribution of B cells is debated.15 T cells are activated by antigens presented in molecular grooves (class II MHC) of dendritic cells in the presence of co-stimulatory molecules on both the dendritic cell (for example, CD 80 and CD86) and on the T cell (for example, CD28). The T cell subsequently undergoes differentiation into cells that either tend to promote inflammation, TH1 response, by activating B cells, macrophages, synoviocytes, and osteoclasts, or downregulate inflammation, a TH2 response. This differentiation is determined by the cytokine milieu, including interleukins, interferon γ, and transforming growth factor β (TGFβ),13 and by T cell maturity, the presence of T suppressor cells, dendricyte lineage, and the degree of co-stimulation. In appropriate cytokine microenvironments TH1 cells may also switch to become TH2.
CYTOKINES
Cytokines are signalling molecules that orchestrate host defence, tissue remodelling, angiogenesis, and control of neoplasia. Most are low molecular weight glycoproteins or peptides and include interleukins, chemokines, interferons, some growth factors, and other independently named molecules such as TNF. They share some of the characteristics of hormones, but unique features form the basis of a sophisticated means of intercellular communication and explain why modulation of a single cytokine produces variable clinical results.
In general, baseline cytokine production is low, with just transient rises during an event. The radius of action is mostly short, but each cytokine has multiple target cells and multiple actions (pleiotropy), and different cytokines have similar or overlapping actions (redundancy). Cytokines may act as antagonists to or synergists with another, or may have a combined action altogether disparate to the individual agents. The action of cytokines is exerted via specific high affinity cell surface receptors resulting in changes in gene expression of the target cell. A cell may express more than one type of receptor to the same cytokine, each with a different action, and receptors may be cleaved from the cell membrane to become “soluble” receptors binding cytokines in solution. Receptors of different cytokines share common signal transduction pathways allowing “cross over” effects.
In simple terms, cytokines influential in RA and JIA may be divided into those that are proinflammatory, such as TNFα, IL-1β, and IL-6, and those that are anti-inflammatory, such as IL-10 and IL-1 receptor antagonist (IL1-ra). Proinflammatory cytokines are produced by numerous cell types and have actions as diverse as T cell activation, induction of acute phase proteins and inflammatory chemical pathways, stimulation of cell growth and differentiation, and control of apoptosis. This is to preserve cellular and biochemical homoeostasis, but overproduction has been shown to be harmful. In other diseases proinflammatory cytokines have been associated with the development of septic shock, adult respiratory distress syndrome, heart failure, and brain injury. Conversely, IL-10 inhibits the production and action of these and other cytokines and directly inhibits proinflammatory cells such as lymphocytes and macrophages.
THERAPEUTIC CYTOKINE MODULATION
Cytokine modulation presumes an imbalance of cytokines, and evidence of this in JIA includes the positive correlation of serum and synovial cytokine concentrations with disease activity,16–18 an increase of antagonists or soluble receptors with a flare,19 demonstration that cytokines induce synovial macrophages and osteoclasts, and other animal20 and genetic studies.21 In addition it appears that established therapies may exert an effect via cytokine modulation. Corticosteroids and cyclosporin A inhibit cytoplasmic nuclear factors important to chemokine gene expression,22,23 whereas thalidomide enhances TNFα mRNA degradation,24,25 and leflunomide inhibits tyrosine phosphorylation important to signal transduction pathways.26
Biologic agents have been developed to restore immune homoeostasis via several strategies including direct cytokine infusion (for example, recombinant IL-10), stimulation or blockade of production (as with steroids), binding of soluble cytokines (for example, TNFα blockade), interference with receptor binding (for example, recombinant IL-1ra), and inhibition of signal transduction (as with leflunomide). Cytokine blockade has become the mainstay and this has been achieved by using monoclonal neutralising antibodies, recombinant soluble cytokine receptors, and other cytokine binding proteins called immunoadhesins.
TNF BLOCKADE
TNFα is considered to be at the fulcrum of many inflammatory pathways (fig 1) and, as such, targeting it is thought to manipulate this wide influence. However, despite considerable knowledge of TNF action, the precise nature of control exerted by blockade remains unclear. Two anti-TNF inhibitors are licensed in the UK, and are under investigation in children (table 1).
Comparison of etanercept and infliximab

TNFα activity. Macrophages and monocytes are a major source of TNFα, which in turn acts on these and other cells to stimulate the production of biochemical, enymatic, and cytokine mediators of inflammation. Further cellular activity ensues. Specifically TNFα acts on synoviocytes resulting in pannus formation and together with the activation of osteoclasts this results in articular erosions and reduced bone density.
Etanercept (Enbrel, Wyeth), is a human soluble TNFα receptor, attached to human IgG. It neutralises TNF by binding with an affinity 50–1000 times that of the naturally occurring TNF receptors and may also exert its effect by binding other cytokines, including IL-1α and TNFβ. It is administered by subcutaneous injection twice weekly, for an indefinite period and may be used with or without methotrexate. It is licensed for use in children aged 4–17 years in accordance with specific guidelines (see Practical management below); early safety and efficacy data in those under 4 years are encouraging.27
Infliximab (Remicade, Schering Plough) is a chimeric human-murine monoclonal antibody that binds both soluble and cell bound TNFα. It is licensed for use in RA, but not for use in children, although the outcome of a multicentre European phase III trial of its use in polyarticular JIA may address this, together with anecdotal reports of its success in JIA.28–30 Infliximab is given by intravenous infusions, and in combination with methotrexate to avoid tachyphylaxis to the murine component. It has a longer half life than etanercept and may have a still more enduring effect by deleting TNFα producing T cells through apoptosis. This latter mechanism has been shown in Crohn’s disease and may be as effective as direct cytokine neutralisation.31
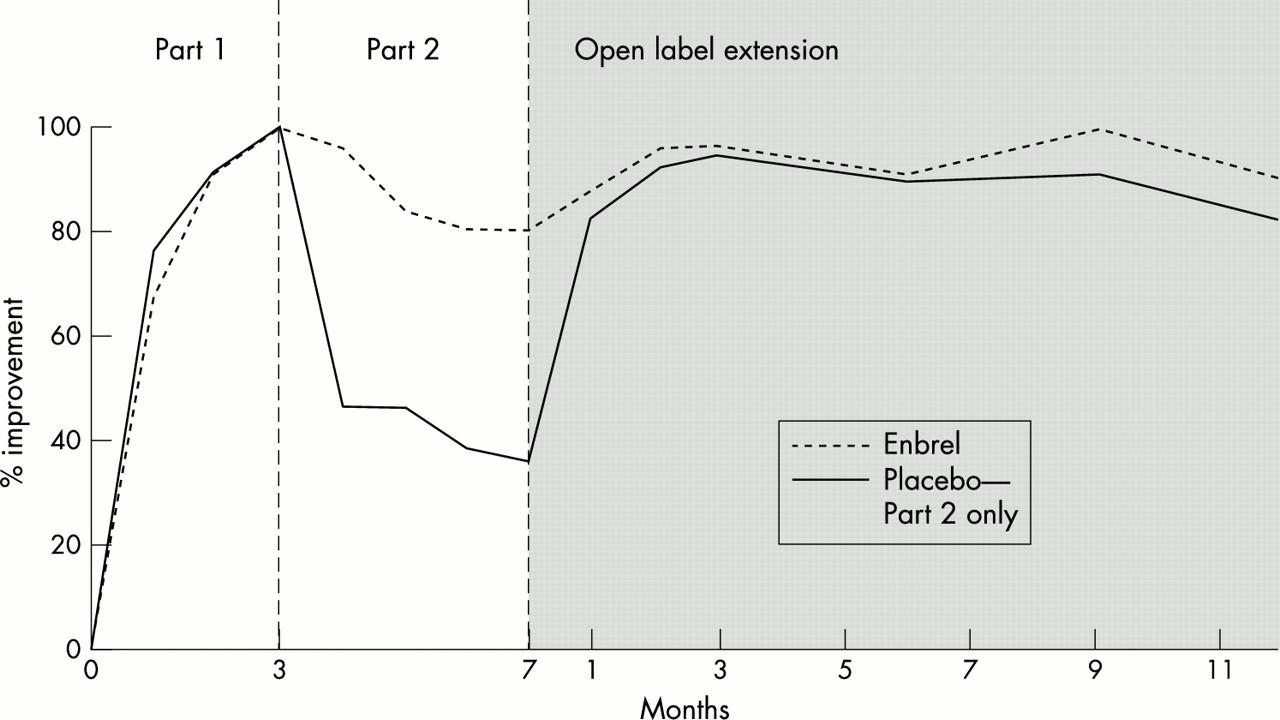
The most detailed trial of TNF blockade in JIA to date involved etanercept. The study, of a years duration32 with five year follow up data available,33 enrolled 69 patients with chronic polyarthritis of variable aetiology and unresponsive to maximum conventional treatment. Owing to ethical considerations a three part trial design was employed (fig 2), with all patients receiving etanercept for the first three months, to permit cessation of other medications, except low dose steroids and NSAIDs. Seventy four per cent of patients achieved a JRA30 response over these three months, this response being defined as a 30% improvement in three of six established measures.34,35 Randomisation occurred during stage two, to which only those who had responded to etanercept in stage one were admitted, the non-responders being withdrawn to receive alternative therapy. Eighty three per cent of those receiving placebo flared at a median of 28 days, whereas only 28% of those still receiving etanercept flared, at a median of 116 days. During the final phase patients from both arms of stage two received etanercept. Seventy four per cent of patients maintained or achieved a JRA30 response, 64% of patients improving by 50%, and 36% improving by 70%. Limitations to the interpretation of this study are apparent, but given the population (patients previously refractory to other medication), this is a remarkable response to treatment. At a median 2.3 years of subsequent treatment 67% of all patients had a 70% improvement in disease activity. Other smaller studies have found similar improvements in polyarticular JIA,36 juvenile dermatomyositis, and juvenile spondyloarthropathy,37 and there are reports of benefit from the simultaneous use of methotrexate.38 Early reports of high dose anti-TNF therapy in systemic disease are encouraging.39

{kind=link}
{kind=link}
The three phases of the trial of etanercept in children with polyarticular JIA. In part 1 both groups received enbrel. In part 2 patients were blinded and randomised to receive enbrel or placebo. Part 3 was again open label with all patients receiving the active agent.32
POTENTIAL RISKS FROM TNF BLOCKADE
Etanercept appears well tolerated by children. Although a higher incidence of headache, nausea, abdominal pain, and vomiting have been reported in children than in adults treated with etanercept for RA, this did not result in discontinuation of treatment. There are no reports of increased risk from infection, a theoretical possibility. For patients already on sulphasalazine the introduction of etanercept may increase the risk of leucopenia.40
Randomised controlled trials of TNF blockade in approximately 900 adults with RA and clinical experience in over 100 000 adults in the USA provide data from which to make some assessment of the potential risk to children. There have been isolated case reports of aplastic anaemia, severe leucopenia, and pancytopenia, and a possible association with demyelinating diseases of the CNS.41,42 The theoretical increased risk of malignancy, over that of the disease itself, has not been reflected clinically,43 but the duration of follow up has been insufficient to determine long term risk. The risk of infection with etanercept, including tuberculosis reactivation, does not appear to be greater than from the disease itself,41,43–46 but increasing numbers of reports indicate a risk of developing antibodies to antinuclear antigen and dsDNA, precipitating a lupus-like syndrome.47–51
OTHER IMMUNOMODULATION
The early successes of anti-TNF therapy have not been mirrored by the use of other immunotherapy. Nor has the wider application of cytokine therapy in other medical disciplines been shown to be as successful. Recombinant colony stimulating factors may shorten periods of neutropenia following chemotherapy, but the long term effect on clinical outcome is unclear. Anti-cytokine treatment in infection, including overwhelming sepsis, has been particularly unrewarding, and the modest benefit of interferon in relapsing remitting multiple sclerosis versus the cost is debatable.
Studies in RA of supraphysiological doses of recombinant IL-1ra, a non-signalling peptide of the IL-1 family that blocks both IL-1α and IL-1β, have shown moderate clinical improvement52 with slowing of the rate of bony erosions and osteopenia.53 However, the short half life requires daily treatment at high levels in order to maintain an excess of IL-1ra over IL-1 at tissue level.53,55 Recombinant IL-10, similarly, has a short half life and studies have shown poor clinical efficacy and that high systemic doses are not well tolerated.56 Such results have led to the examination of alternative approaches to IL-1ra and IL-10 immunomodulation, including local infusion and gene therapy.57–60
Alternatively early results from recombinant anti-human IL-6 receptor monoclonal antibody studies in RA are encouraging, and a phase II therapeutic trial for systemic onset JIA is in process. Indications of its benefit in systemic JIA include an association between flares and increased concentrations of IL-6 and its receptor,17,61–64 associations between specific IL-6 genetic polymorphisms and disease,64 and the promotion of proinflammatory cellular activity by IL-6.65
Other biologic strategies have included direct cellular modulation, such as antibodies to a T cell marker CD4 to reduce a TH1 response.66 Experimental models were encouraging,66–68 but studies in RA and psoriasis have failed to show clinical improvement.69,70 Antibodies have also been targeted against CD-20 markers expressed by B cells.71 Future developments are likely to include targeting of other cytokines, TGFβ, interferon γ, and GM-CSF, combination therapy, and the use of cytokines to either deviate the immune response from one cell type to another (TH1 to TH2) or to control apoptosis. It may also be possible to displace the antigenic peptide from the MHC groove by using synthetic peptides, thereby avoiding cellular activation. Research will also continue to explore genetic applications, not only in terms of gene therapy, but also the identification of genetic populations most likely to respond to treatment.72,73
ETHICAL CONSIDERATIONS
The use of anti-TNF therapy in children has begun to address important ethical considerations. Trials of a novel drug in children with severe JIA must address questions of safety and efficacy in the context of a patient group previously receiving complex long term medication. Lovell et al32 stopped other disease modifying drugs to show that beneficial effects were attributable to etanercept alone. The authors were thus compelled to treat all recruits with the trial medication before randomisation, it being unethical to stop all disease modifying medication. Other concerns included the management of non-responders and interpretation of results in a chronic disease characterised by relapses and remission. This added to the complexity of trial design, an area likely to require further future innovation. Furthermore, the study only shows the value of etanercept as a rescue therapy, long term benefit having yet to be established.
Etanercept is now being used in children with severe disease, and increasingly in those unable to tolerate conventional second line agents. In view of concern about the long term safety of this new group of drugs, and also to identify long term benefit, the British Paediatric Rheumatology Group has drawn up guidelines for prescribing biologic therapies in children and young people with JIA, and has ethical approval for prospective data collection of these patient details in a central registry.74 It is important that extensive data on its use in adults with different diseases does not detract from publication on the use of etanercept in children with JIA. The pharmacokinetics of drugs are different in children and need to be adequately assessed—JIA is a group of diseases which differ from RA and should be examined separately—and children require treatment during unique periods of physiological and psychological change.
PRACTICAL MANAGEMENT OF NEW THERAPIES
In addition to resources being available for national supervision, the success of these new drugs requires appropriate local support. The paediatric rheumatology nurse specialist is critical to the effective provision of practical and emotional support, and information for the child, family, and other staff members. Guidance on administration, blood test monitoring, management of side effects that may include injection site reactions, and appropriate response to infection are important aspects of continuing care. Effective education for both the patient and parents ensures understanding, appropriate expectations, and adherence with the new drug following many years of “ineffective” treatment, and uncontrolled disease activity. Cooperation will depend on a balance between their belief that this time “it may work”, and excessive faith in a new wonder drug. For adolescents already competent at giving medication by injection, the addition of etanercept causes few practical problems. However, many of these patients are in the process of transition, and improved wellbeing highlights a renewed importance of addressing transitional issues of generic health education, employment issues, and achieving the normal tasks of adolescence. A balanced view of potential, but not certain, success after years of difficult management and disability should be presented in the light of largely unknown long term outcome and adverse effects that may include malignancy.
The clinical experience of etanercept in the UK, albeit anecdotal, has been positive. A total of 101 children with JIA were initially identified to be in urgent need of the drug, and funding was made available for 25 children. Current estimates now reveal that 600 children may need treatment; in order to address persistent financial limitations and variation between health authorities, a report by the National Institute for Clinical Excellence has set out criteria for eligibility and withdrawal of treatment.75 Etanercept may be prescribed for a child or young person aged 4 to 17 years with chronic active polyarthritis who shows an inadequate response to, or is intolerant of, methotrexate. Specifically, five or more joints must have been swollen during the previous six months and three joints have limited motion and pain, tenderness, or both. Treatment is withdrawn if the child experiences an unacceptable adverse event or if the child does not respond during the initial six months of treatment or continue to respond thereafter.
Practical approaches to reduce the cost, thereby increasing availability, are also being sought. It is standard practice in the USA to use bacteriostatic water to reconstitute the drug, prolonging the shelf life and allowing multiple doses to be taken from each adult sized vial. This dramatically reduces costs. In the UK, use of bacteriostatic water is prohibited because it is potentially lethal if injected intrathecally. The Medicines Control Agency has now allowed one UK centre to reconstitute etanercept in this way, the drug being prepared by a homecare service to keep it out of the hospital pharmacy and minimise the risk of accidental intrathecal injection.
CONCLUSION
To date etanercept has been extremely beneficial for many children despite uncertainty about long term efficacy and side effects, and clinical studies of TNF antagonists raise hopes that biologic therapies will have a major impact on the long term outcome of arthritis. This is despite the failure of other biologic agents to reach their clinical potential. Refinement of the use of TNF blockade, combination therapies, and alternative biologics are now being investigated and in due course biologics may be used to treat a wider cohort of children with less severe disease. To this end vigilance and appropriate assessment of potential risks is paramount. Ultimately developments in biologic therapies may fundamentally alter the therapeutic approach to all chronic autoimmune diseases.