Article Text

Abstract
Objectives To compare the immunogenicity and safety of the bivalent human papillomavirus (HPV)16/18 vaccine between female patients with juvenile idiopathic arthritis (JIA) and healthy female adolescents.
Methods 68 patients and 55 healthy girls aged 12–18 years were included in a prospective controlled observational cohort and were vaccinated at 0, 1 and 6 months. Primary outcomes were immunogenicity expressed as seropositivity rate after three vaccine doses at 7 and 12 months and HPV-specific geometric mean antibody concentrations. Secondary outcomes were HPV16/18-specific memory B cell responses in a subset of participants and safety, defined as adverse events and the effect of vaccination on JIA disease activity.
Results All participants were seropositive for HPV16 and HPV18 at 7 months. One patient turned seronegative at 12 months for HPV16/18. No significant differences were found between patients and controls in HPV-specific antibody concentrations; however, antibody concentrations were consistently lower in patients. No effect of methotrexate on HPV16 antibodies (p=0.79) or HPV18 antibodies (p=0.37) was detected. All patients on anti-TNFα treatment were seropositive after vaccination. The kinetics of HPV16/18 memory B cell responses was comparable between patients and controls, but the magnitude of B cell responses at 7 and 12 months appeared lower in patients. No relevant differences in adverse events were found. HPV vaccination did not aggravate JIA disease.
Conclusions The bivalent HPV16/18 vaccine is immunogenic and well tolerated in JIA patients. However, HPV-specific antibodies and B cell responses tended to be lower in patients compared with healthy controls.
Clinical trial listing NCT00815282
Statistics from Altmetric.com
Effective and safe vaccination is essential in individuals whose function of the immune system is affected by chronic disorders because these individuals are at an increased risk of infections due to the immunosuppressive effect of the disease or its treatment.1 Current mass immunisation strategies via national immunisation programmes have greatly reduced the burden of childhood infections, but do not take into account the efficacy of vaccinations in these high-risk patients.2
The most common chronic rheumatic disease in childhood associated with increased susceptibility to infections is juvenile idiopathic arthritis (JIA).3 The treatment of JIA involves immunosuppressive drugs and biologicals, increasing the susceptibility to infections.4 In order to prevent infections, effective and safe vaccination is vital for these patients. One of the vaccines included in national immunisation programmes of countries worldwide is the human papillomavirus (HPV) vaccine to prevent cervical cancer. In healthy young women, the bivalent HPV vaccine is safe and immunogenic, and induces a high degree of protection against HPV16/18 infection and their associated premalignant laesions.5–7 However, the efficacy, immunogenicity and safety of HPV vaccination in patients with JIA are yet unknown.8
We conducted a prospective controlled observational cohort study in order to assess the immunogenicity and safety of HPV vaccination in female JIA patients compared with healthy female adolescents. Vaccine-induced serological and cellular immune responses were analysed during 12 months. The safety of the HPV vaccine was assessed by comparing adverse events between patients and controls and by analysing the effect of vaccination on JIA disease activity.
Methods
Study design and participants
In the Netherlands, the bivalent HPV vaccine was included in the national immunisation programme in 2010 for girls aged 12 years. A nationwide catch-up vaccination campaign was performed in 2009 for girls aged 13–16 years. From the start of this vaccination campaign in March 2009 until May 2011, a prospective controlled observational cohort study was performed in which female JIA patients and healthy controls aged 12–18 years were enrolled. Patients were recruited from the paediatric rheumatology unit of the University Medical Centre Utrecht. All patients met the International League of Associations for Rheumatology criteria for JIA.9 No restrictions regarding medication use were applied. Controls were recruited from two secondary schools in the Netherlands. All patients and controls who voluntarily opted for HPV vaccination were eligible for participation. Written informed consent was obtained from participants and their parents/guardians. The study was approved by the medical ethics review committee of the Central Committee on Research involving Human Subjects (CCMO, The Hague, The Netherlands) and was conducted in accordance with good clinical practice guidelines.
Vaccination and follow-up
Participants received three doses of the bivalent Cervarix vaccine (GlaxoSmithKline Biologicals, Rixensart, Belgium) in a 0-, 1- and 6-month schedule. Study visits occurred before the first vaccination, and at 3, 7 and 12 months.
Immunogenicity measures
Immunogenicity was analysed by measuring the level and avidity of HPV-specific immunoglobulin (Ig)G antibodies and memory B cell responses. The level of IgG antibodies against HPV L1 virus-like particle (VLP)16 and VLP18 was measured in all participants at each time point using a VLP-based multiplex immunoassay.10 Sera were incubated with VLP-conjugated beads. HPV-specific antibodies were detected using R-phycoerythrin-conjugated goat antihuman IgG (Jackson ImmunoResearch laboratories Inc, West Grove, Pennsylvania, USA) and analysed using the Bioplex system 200 with Bioplex software (Bio-Rad Laboratories, Hercules, California, USA). Sera were considered HPV antibody seropositive at a cut-off of 9 Luminex Units/ml (LU/ml) for HPV16 and 13 LU/ml for HPV18.
In serum samples from 18 JIA patients and 18 controls, avidity of HPV16/18-specific IgG antibodies at 12 months was assessed by using a modification of the abovementioned multiplex immunoassay. HPV16/18-specific antibody concentrations were adapted to 6000 Median Fluorescent Intensity. Ammonium thiocyanate (NH4SCN; Sigma-Aldrich St. Louis, Missouri, USA) was used to dissociate low-avidity antigen-to-antibody binding.11 After incubation of VLP-conjugated beads with serum, 2.5 M NH4SCN in PBS or PBS only was added for 10 min at room temperature. Residual bound IgG antibodies were detected and analysed as described above. The percentage of antibodies that remain bound to the VLP-conjugated beads after treatment with NH4SCN defines the avidity index.
At each time point, HPV16/18-specific memory B cells were measured in a random subset of 5–10 participants. Heparinised blood samples were obtained for isolation of peripheral blood mononuclear cells using Ficoll density-gradient centrifugation (Amersham Pharmacia, Uppsala, Sweden). B cells were purified and polyclonally stimulated as described previously.12 HPV16/18-specific ELIspot assays were performed by coating multiscreen-IP plates (MISPS4510, Millipore) with PBS containing either 10 µg/ml antihuman total IgG-Fc (MP Biomedicals, Ohio, USA), 30 µg/ml VLP16 or 20 µg/ml VLP18. For the detection of plaques appearing as blue spots, alkaline phosphatase-conjugated goat antihuman IgG was added. Spots were analysed using an ELIspot reader.12 Geometric mean (GM) numbers of HPV16/18-specific memory B cells were expressed per 105 B cells. When no HPV16/18-specific spots were measurable, these samples were set at a value of 0.1.
Safety measures
Safety outcome measures were analysed using a standardised diary for 14 days after each vaccine dose. Serious adverse events were systematically registered in all participants. The effect of HPV vaccination on JIA disease activity was assessed. Disease activity was measured by the Juvenile Arthritis Disease Activity Score including 27 joints (JADAS-27),13 a composite score based on four of the six American College of Rheumatology core criteria for JIA.14 The JADAS-27 is calculated as the sum of the scores of its four components and ranges from 0 (low disease activity) to 57 (high disease activity).
Statistical analysis
A sample size calculation based on the primary outcome immunogenicity revealed that with 55 healthy controls and 55 patients there was 81% power with a two-sided α of 0.05 to detect a 15% lower seropositivity rate in JIA patients compared with healthy controls, with an expected seropositivity rate of 99% in healthy controls.7
Comparison of seropositivity rate after three vaccine doses at 7 and 12 months was performed by Pearson's χ2 test. HPV-specific antibody concentrations were reported as geometric mean concentrations (GMCs) with 95% CI. Differences between patients and healthy controls in HPV-specific GMCs over the total study period were analysed using a linear mixed model. This model takes into account all available samples and allows repeated measurements on the same individual with unequal time periods between measurements. The model, with fixed effects for disease and time, was adjusted for the number of vaccinations and time elapsed since vaccination. It included a random effect of time for each individual to account for clustering of observations within individuals. A likelihood-ratio test was performed to test the effect of JIA disease on the levels and course of HPV-specific antibody concentrations. A preplanned subgroup analysis was performed to assess the effect of methotrexate or biologicals by comparing GMCs between patients with and without medication using the Student t tests. GM numbers of memory B cells were compared between the time points by the Mann–Whitney U test.
Adverse events were reported as absolute frequencies or as median values with IQR. Differences in adverse events between patients and controls were tested by the two-sided Mann–Whitney U tests for quantitative parameters, and by the Pearson's χ2 test for categorical parameters. JIA disease activity, presented as median values with IQR, was compared before and after vaccination by the Wilcoxon matched-pairs signed-ranks test. Effect modification was assessed in patients with high baseline disease activity (JADAS-27≥6.0) and in patients using methotrexate. Statistical analysis was carried out with SPSS V.20.0.0 (SPSS Inc, Chicago, Illinois, USA). All reported p values were based on two-sided tests for significance, and p<0.05 was considered statistically significant.
Results
Baseline characteristics
Of 55 healthy female adolescents and 68 female patients with JIA enrolled in the trial, 49 (89%) healthy controls and 63 (93%) JIA patients could be analysed in the primary immunogenicity analysis (figure 1). In all, 8 (7%) participants dropped out from the study (table 1). The full three-dose vaccination schedule was administered to 50 (91%) healthy controls and 66 (97%) JIA patients, whereas HPV vaccination was postponed in seven patients because of the use of biologicals (n=5) or for personal logistic reasons (n=2). These patients were excluded from the on-protocol immunogenicity analysis. In JIA patients, median disease activity at time of inclusion was low (JADAS-27 of 3.1 points).
Baseline characteristics and serious adverse events during follow-up
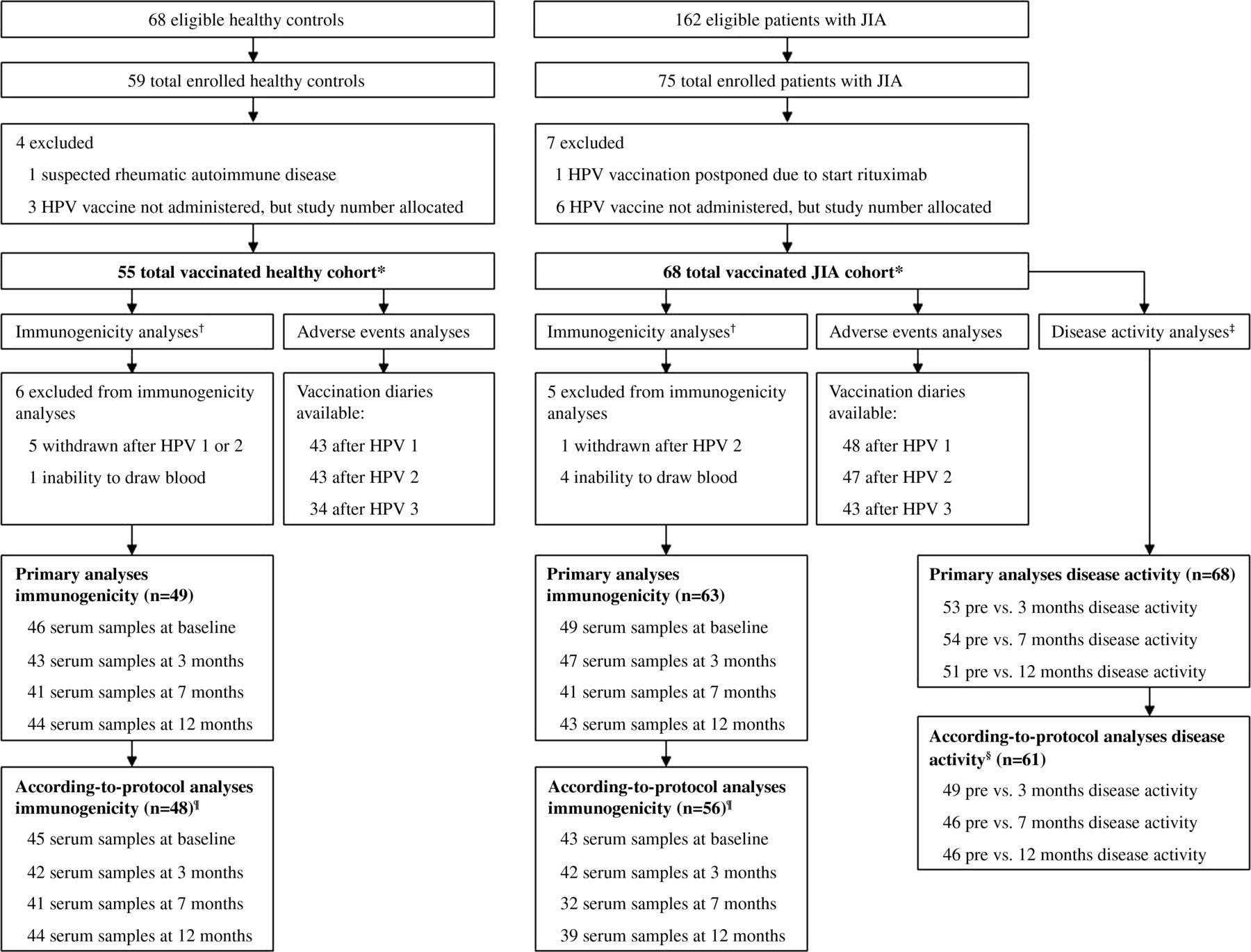
Enrolment of healthy controls and patients with JIA. *Includes all female adolescents who received at least one HPV vaccine dose. †Includes all female adolescents with at least one serum sample after the first HPV vaccine dose. ‡Disease activity was measured using the Juvenile Arthritis Disease Activity Score involving 27 joints; this could be assessed in 68 patients in whom a disease activity score could be calculated before and at least once after HPV vaccination. §Includes only the disease activity scores calculated in patients who were vaccinated and clinically assessed according to protocol. Compared with the primary analyses, HPV vaccination was postponed in seven patients, and four clinical assessments of three patients were not in accordance with the protocol. ¶ Includes only the serum samples drawn according-to-protocol from 48 healthy controls and 56 JIA patients who were vaccinated according to the schedule 0, 1 and 6 months. Compared with the primary analyses, one healthy control was lost to follow-up after 3 months, and seven JIA patients were excluded because the second or third HPV vaccination was postponed. HPV, human papillomavirus vaccination; JIA, juvenile idiopathic arthritis.
Immunogenicity
The primary analysis for immunogenicity in the total vaccinated cohort showed that all patients and healthy controls were seropositive 7 months after the first vaccination. All controls were seropositive for HPV16 and HPV18 at 12 months, whereas one patient had turned seronegative for HPV16 and HPV18 after demonstrating HPV-specific antibody concentrations comparable with the total JIA population at 3 and 7 months. This oligoarticular JIA patient was vaccinated according to protocol. Four JIA patients had received only one vaccination after 3 months; two of these patients were still seronegative for HPV16 and three were still seronegative for HPV18 at that time point. These patients turned seropositive after the third dose. Thus, the full three-dose HPV vaccination schedule induced high seropositivity rates in JIA patients, comparable with healthy controls.
No statistical significant differences were detected in HPV-specific GMCs over time between JIA patients and healthy controls (figure 2). The likelihood-ratio test (4 degrees of freedom) for the effect of disease was 5.64 for HPV16 (p=0.23) and 2.27 for HPV18 (p=0.69). Although non-significant, HPV-specific GMCs were consistently lower in JIA patients compared with healthy controls. Similar results were found in the according-to-protocol analyses (data not shown). HPV16/18-specific GMCs in 52 serum samples of 32 patients using methotrexate were compared with GMCs in 71 samples of 31 patients without methotrexate. Methotrexate did not affect HPV16 antibodies (2578 LU/ml (95% CI 1338 to 4967) vs 2844 LU/ml (95% CI 2034 to 3976); p=0.79) or HPV18 antibodies (860 LU/ml (95% CI 963 to 3595) vs 1335 LU/ml (95% CI 951 to 1873); p=0.37).
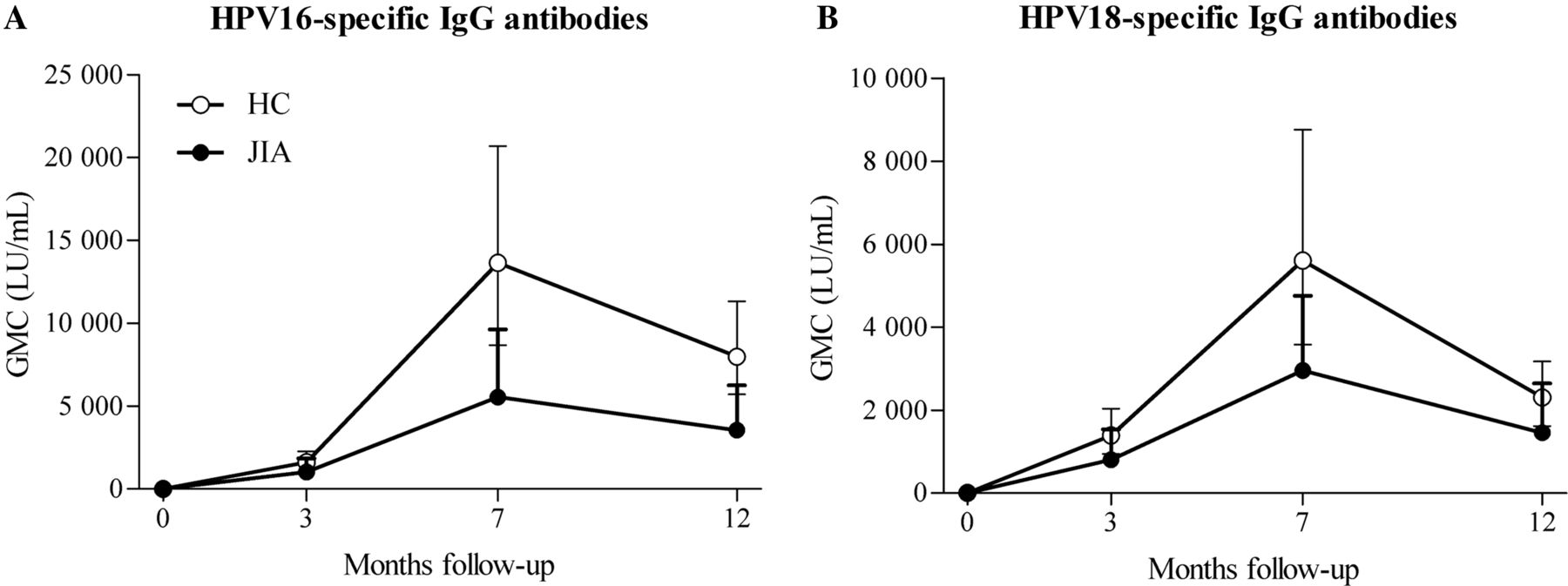
HPV16- and HPV18-specific geometric mean IgG antibody concentrations. Geometric mean HPV16/18-specific IgG antibody concentrations (with 95% CI) against HPV16 (A) and HPV18 (B) are indicated at baseline and during follow-up for healthy controls (open dots) and JIA patients (black dots) at baseline (0 month), 1 month after the second vaccination (3 months), 1 month after the third vaccination (7 months) or 1 year after the first vaccination (12 months). HC, healthy controls; HPV, human papillomavirus; JIA, juvenile idiopathic arthritis patients.
All patients on methotrexate were seropositive at 12 months after the first vaccination, except for one patient. Although antibody concentrations were non-significantly lower in patients on anti-TNFα treatment, all patients were seropositive after three vaccine doses. The number of patients on anti-TNFα was too small to draw definite conclusions.
Avidity of HPV16/18-specific antibodies was comparable in a random sample of 18 JIA patients and 18 healthy controls (figure 3). The avidity index of HPV16-specific antibodies was 86% (95% CI 84% to 88%) in patients and 83% (95% CI 77% to 89%) in controls. Similar indices were found for HPV18 in patients (86% (95% CI 83% to 90%)) and controls (86% (95% CI 82% to 89%)).

Avidity index of HPV16- and HPV18-specific IgG antibodies. Mean avidity indices (with 95% CI) for 18 healthy controls (open dots) and 18 JIA patients (black dots) at 12 months follow-up are indicated. HC, healthy controls; HPV, human papillomavirus; JIA, juvenile idiopathic arthritis patients.
Overall, the number of total IgG-producing B cells was similar in JIA patients (GM 7.9 (95% CI 6.8 to 9.2)) and healthy controls (GM 6.7 (95% CI 5.6 to 8.1)). In JIA patients, HPV16/18-specific memory B cell responses increased at 3 months (HPV16 p=0.004; HPV18 p=0.002) and 7 months (HPV16 p=0.15; HPV18 p=0.03) after vaccination, and subsequently declined (figure 4). The kinetics of the HPV16/18 memory B cell response was comparable in patients and controls, but the magnitude of B cell responses appeared lower in JIA patients at 7 and 12 months.

Geometric mean numbers of HPV16 and HPV18 memory B cells. Geometric mean numbers of HPV16 (A and B) and HPV18 (C and D) memory B cells are indicated per 105 B cells for JIA patients (black dots, A and C) and healthy controls (open dots, B and D). Each dot indicates one participant at baseline (0 month), 1 month after the second vaccination (3 months), 1 month after the third vaccination (7 months) or 1 year after the first vaccination (12 months). * p<0.05, ** p<0.01. HC, healthy controls; HPV, human papillomavirus; JIA, juvenile idiopathic arthritis patients.
Memory B cells against HPV16 could not be detected in five patients and two controls and against HPV18 in three patients and one control, although they all had detectable antibody concentrations. It remains unclear why these participants failed to mount a HPV16/18-specific memory B cell response. The treatment of the five patients was not severely immunosuppressive: only one used methotrexate with anti-TNFα, whereas two used methotrexate and two did not use any immunosuppressive drug.
Safety
Regarding vaccine safety, redness and bruising at the injection site were reported more frequently by healthy girls (see online supplementary table S1), while the duration of these local symptoms was similar. The frequency of general symptoms was comparable in patients and controls. In the context of chronic arthritis characterising JIA disease, new onset or worsening of pre-existing arthralgia is of special interest. The occurrence of arthralgia was similar in both groups, yet the mean duration was significantly longer in JIA patients (p<0.001). Serious adverse events occurred more often in JIA patients (table 1). The majority of these serious events were preplanned interventions, diagnostic hospital admissions for pre-existing complaints or adverse events associated with the treatment of JIA disease and were therefore judged to be unrelated to HPV vaccination.
Disease activity measured by the JADAS-27 did not worsen after HPV vaccination (figure 5A). In fact, compared with baseline the JADAS-27 was significantly lower at 7 months (2.8 (IQR 0.2–6.0) vs 3.1 (IQR 1.2–6.8); p=0.007) and at 12 months after inclusion (1.8 (IQR 0.1–4.6); p=0.006). Similar results were found in the according-to-protocol analysis (data not shown); in the subgroup of 18 patients with high baseline disease activity (figure 5B); in 24 patients using methotrexate (figure 5C); and in nine patients using anti-TNFα treatment (data not shown). Overall, these data indicate that HPV vaccination does not negatively affect JIA disease activity.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disease activity in JIA patients during 12 months follow-up. Median (IQR) JIA disease activity, expressed as the JADAS-27, in the year following the first HPV vaccination is depicted in the total JIA population (A), in 18 patients with high baseline disease activity, defined as a JADAS-27 of at least 6.0 points (B), and in 24 patients using methotrexate at baseline (C). In the total JIA population (A), the disease activity was lower at 7 months (JADAS-27 2.8 (IQR 0.2–6.0) vs 3.1 (IQR 1.2–6.8); p=0.007) and at 12 months (1.8 (IQR 0.1–4.6); p=0.006). In patients with high baseline disease activity (B), disease activity was lower at 3 months (JADAS-27 6.9 (IQR 3.0–9.3) vs 9.5 (IQR 8.1–12.7); p=0.02), at 7 months (6.4 (IQR 4.1–8.9); p=0.008) and at 12 months (6.7 (IQR 2.6–10.7); p=0.004). In patients using methotrexate (C), disease activity was lower at 7 months (JADAS-27 4.0 (IQR 1.0–6.4) vs 4.1 (IQR 2.6–9.8); p=0.02) and at 12 months (3.0 (IQR 0.2–5.7); p=0.002). * p<0.05, ** p<0.01. HPV, human papillomavirus; JADAS-27, Juvenile Arthritis Disease Activity Score including 27 joints; JIA, juvenile idiopathic arthritis patients; MTX, methotrexate.
Discussion
This prospective controlled study shows that the bivalent HPV16/18 vaccine induces high seropositivity rates and strong HPV16/18-specific antibody responses in female adolescents with JIA, comparable with healthy female adolescents. The quality of the HPV16/18-specific antibodies measured by their avidity and the kinetics of HPV16/18-specific memory B cell responses were similar in patients and healthy controls, although the magnitude of B cell responses at 7 and 12 months tended to be lower in patients. Regarding safety, local injection site symptoms were more common in healthy controls whereas general symptoms tended to last longer in patients. HPV vaccination did not negatively affect JIA disease activity.
Vaccine-derived HPV-specific antibodies are considered largely responsible for the protection against persistent HPV infections and precancerous lesions.5 ,15 ,16 With regard to the avidity of HPV-specific antibodies, it is unknown whether high avidity antibodies play a critical role in protection against HPV infection.17 HPV-specific memory B cells are important determinants of long-term protection since they provide this rapid burst of antibody upon rechallenge and play a role in maintaining serological memory over time.18–22 The comparable strong HPV16/18-specific antibody response, avidity of HPV16/18-specific antibodies and kinetics of HPV16/18-specific memory B cell responses indicate that at least these surrogate endpoints for HPV vaccine efficacy are similar in JIA patients and healthy controls.
Despite the good short-term immunogenicity of the bivalent HPV vaccine in JIA patients, there is reason for cautiousness. Numerous studies have analysed vaccine responses in patients with rheumatic diseases up to 2 years after vaccination. Responses were generally comparable with healthy controls, although various studies found non-significantly lower antibody concentrations.8 Also in our study HPV-specific antibody concentrations were consistently lower in JIA patients, albeit non-significant. These lower responses may be due to underlying defects in the immune system of JIA patients. Premature ageing of the immune system resulting in low antibody responses to vaccinations has been described.23 Furthermore, a minority of patients with autoimmune diseases have associated primary immunodeficiencies.24 Besides the lower short-term responses, the long-term persistence of several vaccine-specific antibodies has been shown to be significantly lower in JIA patients compared with healthy controls.25 In addition, the magnitude of HPV-specific B cell responses tended to be lower in JIA patients at 7 and 12 months after vaccination. The lower serological and cellular responses might indicate that over time, protection against HPV infection is not guaranteed.
Since vaccinations may theoretically aggravate the course of autoimmune diseases via bystander activation or molecular mimicry,26 a JIA-specific measure for HPV vaccine safety is the effect of vaccination on JIA disease activity. Our study design, in which patients served as their own controls, enabled detection of worsening disease activity after vaccination if indeed HPV vaccination would have deteriorating effects. With data of 53 patients at 3 and 54 patients at 7 months, a minimum difference in JADAS-27 of 1.6 out of 57 points could be detected. No detrimental effect of HPV vaccination on JIA disease activity was detected, not even in patients with high baseline disease activity, or patients using methotrexate or anti-TNFα.
Adverse events were systematically documented in both patients and controls. Non-serious adverse events were generally similar in patients and controls, transient and of short duration. Serious adverse events occurred more frequently in JIA patients than in healthy controls, but none were deemed related to HPV vaccination. The majority of these serious events were associated with the treatment or diagnosis of (complicated) JIA disease. In all three patients diagnosed with inflammatory bowel disease during the study, the onset of complaints was prior to the first vaccination.
In case of at least 15% difference in seropositivity rate, the null hypothesis (ie, seropositivity rate in patients and controls is similar) would be rejected. In order to detect a 15% difference in seropositivity rate between patients and controls, we needed to include 55 patients and healthy controls. Although the number of healthy controls was too small (49 instead of 55), the difference in seropositivity rate between patients and controls was only 2%. As inclusion of the intended 55 healthy controls would not have led to a 15% difference in seropositivity rate, we believe that our conclusion that seropositivity rate after HPV vaccination is similar in patients and controls is justified. The low participation rate was partly due to the low HPV vaccination coverage (49.9% for the first vaccine dose) in the Netherlands.27
Safe and effective vaccination of individuals whose function of the immune system is affected by chronic diseases is a challenge in current immunisation strategies as these strategies may fail to target high-risk individuals.2 Since children with rheumatic diseases have high risks of infections,28 it is essential to know whether these patients benefit from HPV vaccination. The bivalent HPV vaccine does not aggravate JIA disease, and is well tolerated and immunogenic in the 12 months after the first HPV vaccination. Since our results do not exclude the possibility that long-term protection against HPV infection is inadequate in JIA patients, we recommend a proactive approach in the immunesurveillance of JIA patients, even though it is yet unknown what antibody concentrations are needed for protection against HPV infection.5 ,7 If antibody concentrations wane below antibody levels associated with natural infection, revaccination should be considered. Moreover, continued secondary prevention via cervical smears seems prudent in these patients.
Acknowledgments
We thank all JIA patients and healthy controls who volunteered for the study; Marjolein Musbach and Marjoleine van Opdorp, research managers in the University Medical Centre Utrecht, for trial coordination; the paediatric rheumatologists/immunologists in the University Medical Centre Utrecht for clinical assessments; Lia de Rond and Debbie van Rooijen, technicians at the National institute for public health and the environment, for technical assistance; and Maarten Schipper, PhD, statistician at the National institute for public health and the environment, for his expert partaking in statistical analyses.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Handling editor Tore K Kvien
-
MWH and MS shared first author, respectively NMW, FRMvdK shared last author.
-
Contributors MWH, GAMB, FRMK and NMW designed the study. MWH, CT, NG, FRMK and NMW gathered clinical data. MWH, MS, RMS, FRMK and NMW gathered serum samples. MS and RMS measured serology and performed avidity assays. AMB designed and refined B cell memory assays. MS performed B cell assays. MWH performed statistical analyses. All authors were involved in the interpretation of data. MWH and MS wrote the draft of this paper and all authors contributed to and approved the final version and had final responsibility for the decision to submit for publication.
-
Funding GlaxoSmithKline provided virus-like particles for laboratory assays and financially supported the purchase of HPV vaccines. The Dutch Arthritis Association (Project number 07-02-403) supported this study. The sponsors had no role in design and conduct of the study design; collection, management, analysis and interpretation of the data; and preparation, review or approval of the manuscript.
-
Competing interests NMW has received lecture fees from Novartis and an unrestricted educational grant through his institution from GlaxoSmithKline. All other authors declare no competing interests.
-
Patient consent Obtained.
-
Ethics approval The study was approved by the medical ethics review committee of the Central Committee on Research involving Human Subjects (CCMO, The Hague, The Netherlands). Written informed consent was obtained from participants and their parents/guardians.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Additional serology data on other HPV serotypes is available from the authors on request.