Article Text

Abstract
Objectives Information on mortality in ankylosing spondylitis (AS) is scarce. Our study therefore aimed to assess: (1) mortality in AS versus the general population, and (2) predictors of death in the AS population.
Methods Nationwide cohorts of patients with AS diagnosed at rheumatology or internal medicine outpatient clinics (n=8600) and age-matched, sex-matched and county-matched general population comparators (n=40 460) were identified from the National Patient Register and the census register, respectively. The follow-up period began on 1 January 2006 or at the first date of registered diagnosis thereafter and extended until death, emigration or 31 December 2012, whichever occurred first. Socioeconomic variables, AS-related clinical manifestations, joint surgery, comorbidities and medication were identified from other national registers. Cox regression models were used to determine mortality and predictors for death in the AS cohort.
Results There were 496 deaths in the AS cohort and 1533 deaths in the control cohort resulting in an age-adjusted and sex-adjusted HR of 1.60 (95% CI 1.44 to 1.77), with increased mortality for men (age-adjusted HR=1.53, 95% CI 1.36 to 1.72) and women (age-adjusted HR=1.83, 95% CI 1.50 to 2.22). Within the AS cohort, statistically significant predictors for death were a lower level of education, general comorbidities (diabetes, infections, cardiovascular, pulmonary and malignant diseases) and previous hip replacement surgery.
Conclusions Mortality was increased for male and female patients with AS. Predictors of death within the AS cohort included socioeconomic status, general comorbidities and hip replacement surgery.
- Ankylosing Spondylitis
- Epidemiology
- Outcomes research
- Spondyloarthritis
Statistics from Altmetric.com
Introduction
Ankylosing spondylitis (AS) is a chronic, potentially disabling, inflammatory disorder with skeletal and systemic manifestations.1 The disease usually starts early,2 and poses a long-standing burden on the patient and the society.3
Increased mortality compared with the general population has consistently been shown for some other chronic inflammatory diseases, such as rheumatoid arthritis4 and severe psoriasis,5 whereas for other conditions such as psoriatic arthritis6 and inflammatory bowel diseases,7 results are less consistent.
Mortality studies in AS are relatively few and in general of limited size.8–15 Previous small, hospital-based or clinic-based cohort studies have shown increased mortality in patients with AS compared with the general population with standardised mortality ratios (SMRs) ranging between 1.33 and 1.80, with cardiovascular disease (CVD) being the leading cause of death.9–13 No increased risk for malignancy16 ,17 or malignancy-related deaths in AS have been demonstrated, with the exception of a few older studies of patients exposed to spinal irradiation.8 ,14 ,15 Moreover, only a few studies have addressed possible risk factors for increased mortality and sex-specific mortality rates (MRs).11 ,13
Given the scarcity of the data on mortality in AS, the small size of the previous cohort studies and the lack of contemporary AS mortality estimates, we conducted a nationwide, population-based study with the aim to assess the mortality in patients with AS compared with the general population, overall and by sex, and to investigate factors associated with death in the AS population.
Methods
Study design
This is a population-based cohort study of patients with AS and matched general population comparators, with mortality as the primary outcome.
Setting
Provision of healthcare in Sweden is independent of the individuals’ financial and insurance situation, and largely based on a public, tax-funded system, with an upper limit to the individuals’ yearly expenses for medical consultations and prescription medications. Patients with AS in Sweden typically, at least once, get diagnosed in public specialised care18 and are thus registered in the Swedish National Patient Register (NPR). The unique personal identification number that all citizens in Sweden have enables linkage of information from several national registers.
Data sources
The NPR19 is an individual-based register that comprises the Inpatient Register (IPR) and the Outpatient Register (OPR). The IPR was launched in 1964 and complete national coverage (almost 100%) was reached in 1987.20 It contains data (medical and administrative) from all patients discharged from hospitals in Sweden. The OPR for specialised care was started in 2001. The coverage is generally lower than that for the IPR (approximately 73% in 2008 and 87% in 2011), mainly due to missing data from private caregivers.21 ,22 Primary care visits are not covered by the NPR. Main and auxiliary diagnoses are registered according to the WHO International Classification of Disease (ICD) codes.23 In the present study, the NPR was used for the identification of AS cases as well as the identification of general comorbidities and AS-related clinical manifestations, assessed as possible predictors for mortality (for ICD-codes see online supplementary table S1).
Statistics Sweden,24 which is also responsible for the census register, was used for the identification of the reference cohort, the retrieval of data on place of birth, immigration, emigration and residency, as well as data on level of formal education.
The Swedish Prescribed Drug Register (PDR)25 contains information on dispensed drugs for ambulatory care from Swedish pharmacies since July 2005, with an estimated coverage close to 100%.26 The PDR was used to determine exposure to non-steroidal anti-inflammatory drugs (NSAIDs), oral glucocorticosteroids and synthetic disease modifying antirheumatic drugs in AS and control cohorts prior to the study start and during follow-up, as well as to ascertain dispensed medications for certain comorbidities (ie, CVD and diabetes mellitus (DM)) at start of follow-up (for Anatomical Therapeutic Chemical codes see online supplementary table S2).
The Swedish biologics register (Anti-Rheumatic Therapy in Sweden Register; ARTIS)27 was used to ascertain use of tumour necrosis factor inhibitors (TNFi) prior to the study start and during follow-up. ARTIS includes prescribed subcutaneous TNFi, and intravenous therapies, which to a lower extent are captured by the PDR. ARTIS captures over 85% of administered therapies with TNFi for AS.28
Information regarding the vital status and the assigned cause of death for AS cases and population comparators until December 2012 was retrieved from the Cause of Death Register,29 which entails information on dates and cause(s) of death for all deceased residents since 1961.
Study population
AS cohort
We used the OPR to identify patients with at least one visit to a physician at a rheumatology or internal medicine department with an AS diagnosis (according to ICD-codes) registered between 1 January 2001 and 31 December 2009. Only those 18 years or older at the date of first diagnosis registration in the OPR were included in the study.
Reference cohort
For each AS case, five reference subjects were selected from the population register (ie, census register) to serve as controls. The cases and controls were matched on age, sex and county at the time of the first spondyloarthritis (SpA) diagnosis (AS, undifferentiated SpA or psoriatic arthritis) registration in the NPR, a time point that could occur several years before the start of the follow-up period for the present study. Matching at the time of the first SpA diagnosis, rather than the first AS diagnosis, was chosen as a number of cases were expected to first receive another SpA diagnosis, before development and subsequent documentation of a diagnosis of AS. At the start of the follow-up period each AS case thus had between zero and five controls, with the majority (96%) having five controls.
Follow-up and outcome
The follow-up for AS cases (N=8600, 65.5% men), began on 1 January 2006 for the cases with an AS diagnosis registered in the OPR before this date, and at the date of the first AS diagnosis registration for those diagnosed after 1 January 2006. The follow-up period for the controls (N=40 460, 65% men) started simultaneously with their matched AS cases. Those who had died (165 AS cases, 394 controls) or emigrated (15 AS cases, 293 controls) between the time for first SpA diagnosis and the start of follow-up were excluded. Controls who were diagnosed with AS during the follow-up period (n=28) served as controls until the date of diagnosis, after which they were included in the AS cohort. The follow-up period for both cohorts ended at the earliest of death, emigration or 31 December 2012.
All-cause mortality based on information retrieved from the national Cause of Death Register was our primary outcome. Cause(s) of death were also categorised in seven categories: cardiovascular, malignancy, infections, renal disease, suicide, spinal trauma and other (for ICD-codes see online supplementary table S1).
Predictors for mortality within the cohort of patients with AS
Level of formal education was grouped as ≤12 years vs >12 years. Those with birthplace other than Sweden were defined as having foreign origin. Disease duration was dichotomised as short versus long based on whether a first AS diagnosis registration in the OPR occurred before or after 1 January 2006 (start of follow-up). Clinical manifestations related to AS (anterior uveitis, psoriasis, inflammatory bowel disease, peripheral arthritis, aortic valve insufficiency), hip replacements, other surgery and general comorbidities (CVD, DM, chronic pulmonary disease, malignancy, infections) were identified via supporting registered ICD-codes in the NPR at any moment prior to the start of follow-up (see online supplementary table S1). In addition, for the ascertainment of CVD and DM, either a supporting ICD-code in the NPR or dispensing of pharmacological agents suggesting such diagnosis prior to the start of follow-up, was used (see online supplementary table S2).
Sensitivity analyses
First, since an increase in mortality may be expected the first months after a diagnosis of a disease, analyses were also performed with a delay in the start of follow-up of 6 months and for tertiles of follow-up time. Second, to explore the possible effect of misclassification in AS diagnosis, analyses were also performed based on the assumption that 20% of the AS cohort had either the same MRs as the control cohort or doubled MRs compared with those primarily estimated for the AS cohort.
Statistics
Demographics and disease characteristics for AS and control cohorts at start of follow-up are presented as frequencies. Crude age-specific and sex-specific MRs in 10-year age strata for both cohorts were expressed as the number of deaths per 1000 person-years at risk. Crude incidence rate ratios and 95% CIs are presented in total and by sex in all age strata. Survival curves using the Kaplan-Meier method are presented for AS and control cohorts in total and stratified by sex, as well as for tertiles of follow-up period. Cox proportional hazards (PH) regression models were used to calculate overall age-adjusted and sex-adjusted HR, as well as separate age-adjusted HRs for men and women. Cox PH regression models were also used in our sensitivity analyses. Age-adjusted and sex-stratified HRs were also calculated for possible predictors of death in the AS cohort. Interactions between the covariates were tested for and included in the models if statistically significant. The PH assumptions for Cox regression analysis were evaluated graphically in survival curves and log-minus-log plots and were estimated to be fulfilled. All analyses were performed with the use of IBM SPSS Statistics V.20 and Microsoft Excel V.2010.
Results
Characteristics of the AS and control cohorts at start of follow-up
Demographics and disease characteristics of the AS and control cohorts at start of follow-up are shown in table 1. Due to the matched design of the study, the age and sex distributions were similar in the AS and controls cohorts. The mean duration between the first SpA diagnosis registration in the NPR and the start of follow-up period was 6.8 years (SD 8.1) for the AS cases. The AS cases had a slightly lower proportion with higher level of education (>12 years) and foreign origin at start of follow-up, whereas the proportions for all general comorbidities, including CVD, DM, infections, malignancies and chronic pulmonary disease were substantially higher in the patients with AS. The frequencies of AS-related clinical manifestations, joint surgery and pharmacological treatments were low in the control population, with the exception of dispensed NSAIDs and oral glucocorticosteroids.
Demographics and disease characteristics of the AS and control cohorts at start of follow-up
Mortality rates
During the observation period 496 deaths occurred in the AS cohort and 1533 in the control cohort during 52 031 and 275 698 person-years, respectively, resulting in crude MRs of 9.5/1000 person-years in the AS cohort and 5.6/1000 person-years in the control cohort. The estimated MRs were higher in the AS cohort compared with the control cohort in all age and sex strata (table 2). In the AS cohort, men had higher MRs compared with women up to the age of 79 years, and the MRs increased with age in both sexes.
Mortality rates in the ankylosing spondylitis (AS) and the control cohorts in total and by sex and age and incidence rate ratios by sex and age
Kaplan-Meier survival curves and HRs
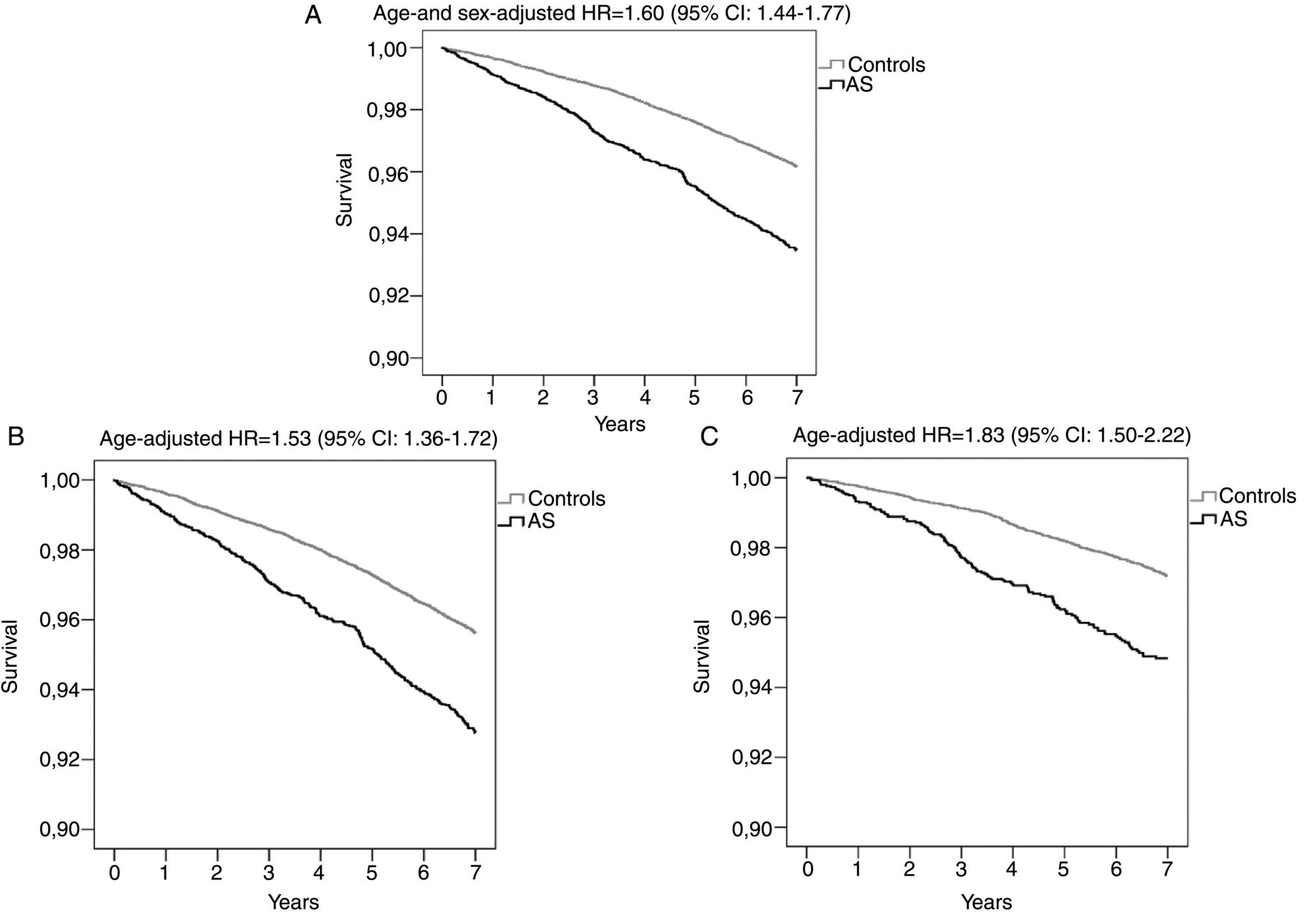
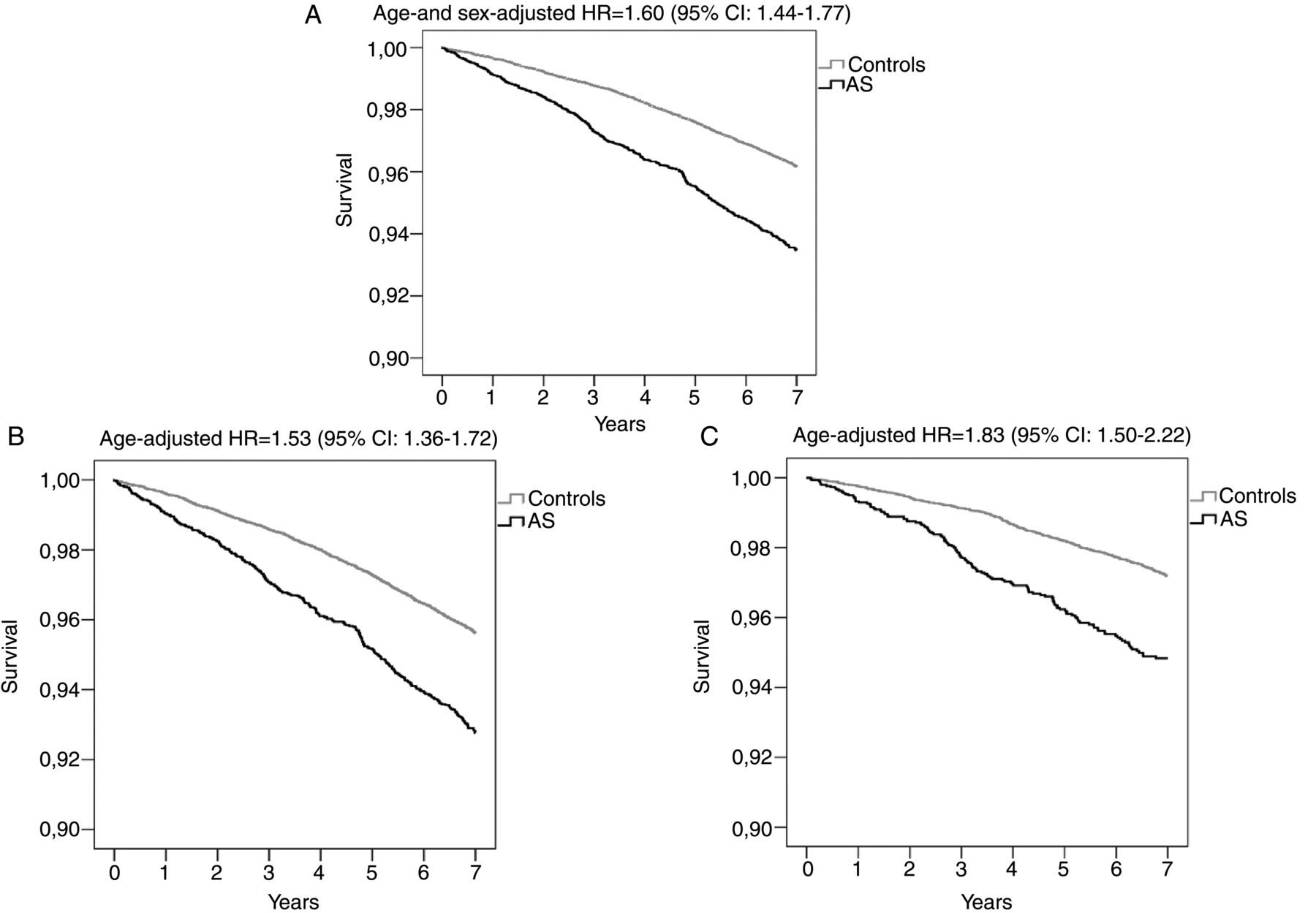
All-cause mortality was overall increased in patients with AS (age-adjusted and sex-adjusted HR=1.60; 95% CI 1.44 to 1.77) (figure 1A) and for men (age-adjusted HR=1.53; 95% CI 1.36 to 1.72) (figure 1B) and women (age-adjusted HR=1.83; 95% CI 1.50 to 2.22) (figure 1C). The estimated 6-year survival was 94.5% (95% CI 93.9% to 95.0%) in the AS cohort and 96.9% (95% CI 96.7% to 97.1%) in the control cohort.
{kind=link}
Kaplan-Meier survival curves and HRs for the ankylosing spondylitis (AS) and control cohorts in total (A), for men (B) and for women (C).
Causes of death
The major cause of death in the AS cohort was CVD, being more frequent in the AS than in the control cohort (34.7% vs 30.6%). The proportion of deaths assigned to infections and renal disease was somewhat higher in the AS cohort compared with controls (5% vs 3.5% and 1% vs 0.4%), while those assigned to malignancy (23.4% vs 34.0%) and suicide (2.0% vs 3.5%) were lower. Although spinal trauma was never registered as the leading cause of death, it was a more common intermediate cause of death in the AS than in the control cohort (2.2% vs 0.3%).
Mortality predictors in the AS cohort
Male gender and higher age independently predicted mortality in the AS cohort. Therefore, all analyses of other possible predictors were adjusted for age and sex. Mortality was significantly predicted by a lower level of education (HR=0.67, 95% CI 0.53 to 0.85), occurrence of CVD (HR=1.99, 95% CI 1.58 to 2.49), DM (HR=1.92, 95% CI 1.51 to 2.45), chronic pulmonary disease (HR=3.03, 95% CI 2.27 to 4.04), malignancy (HR=1.67, 95% CI 1.32 to 2.12) and infections (HR=2.01, 95% CI 1.68 to 2.34) prior to the start of follow-up (table 3). Among factors reflecting disease manifestations or complications, only a history of hip replacement significantly predicted death (HR=1.65, 95% CI 1.29 to 2.12). Other joint surgery had no significant impact (table 3).
Predictors of mortality within the cohort of patients with ankylosing spondylitis (AS)
Sensitivity analyses
Introducing a delay in the start of follow-up of 6 months only marginally affected age-adjusted and sex-adjusted HR (1.57; 95% CI 1.42 to 1.74 vs 1.60; 95% CI 1.44 to 1.77). In addition, all-cause mortality was significantly increased in all the three tertiles of follow-up time, although a slightly higher HR was observed during the first tertile (see online supplementary figure S3). Finally, assuming a misclassification of 20% of the AS cases, the age-adjusted and sex-adjusted HR was 1.41 (95% CI 1.27 to 1.56) when setting the MRs in 20% of the AS cohort to the same level with the reference cohort, and 1.90 (95% CI 1.72 to 2.06) when 20% of the AS cohort had theoretically doubled MRs compared with those primarily estimated for the AS cohort.
Discussion
In this nationwide, population-based cohort study, we found that the all-cause mortality was significantly increased in patients with AS compared with the general population (HR=1.60), for men and women. Within the AS cohort, higher age, male sex, lower level of formal education (≤12 years), general comorbidities (CVD, DM, chronic pulmonary disease, malignancies and infections) and hip replacement surgery, were statistically significant predictors of death. CVD was the leading cause of death in patients with AS.
Substantially impaired survival has been demonstrated in patients with AS exposed to spinal irradiation.8 ,14 ,15 In patients with AS unexposed to radiotherapy, mortality has previously only been addressed in a few, small, hospital-based or clinic-based studies, which have demonstrated SMRs raging between 1.33 and 1.80.9–13 Because of the larger size of our study, we were able to specifically address mortality in women, in whom the mortality risk relative to controls was found to be at least as high as in men, but as expected with lower absolute rates. Furthermore, the relative mortality risk in AS that we observed was similar to that reported in rheumatoid arthritis (RA), where the mean SMRs of non-inception cohorts were 1.73.4
In our AS cohort, hip replacement surgery, which may partly reflect the burden of disease,30 was a predictor of death. Several smaller studies have shown that markers of disease activity or severity, such as higher erythrocyte sedimentation rate and C reactive protein levels, greater number of inflamed peripheral joints at the beginning of follow-up, and work disability are predictive of death in patients with AS.11 ,13 It has also been suggested that diagnostic delay and possibly the infrequent use of NSAIDs may predict death,13 although the latter may reflect channelling bias, as patients with CVD are less likely to receive such medication.31 In our study, general comorbidities, of which CVD was the most prevalent at baseline, were strong predictors of mortality in the AS cohort. This was expected given the strong impact of these comorbidities on mortality in the general population. Since the present analyses were not based on an inception cohort, it was not possible to determine clearly whether this observation can be explained by a shared aetiology between AS and CVD (or other comorbidities), or whether general comorbidities represent path variables that are partially caused by AS, or whether the observation reflects detection bias that relates to more frequent contact by the AS cohort with healthcare services. A lower education level was also a significant predictor of death in the AS cohort. This has also been shown for other rheumatic diseases (eg, RA) and for the general population.4 ,32 The role of pharmacological therapies (NSAIDs and TNFi) as mortality predictors in the AS cohort was beyond the scope of this study and thus not assessed, since it would require another study design and a set of sensitivity analyses to try to handle problems of channelling bias and unmeasured confounding.
The distribution of causes of death differed slightly between the two cohorts, with deaths assigned to CVD or infections being more common in patients with AS. This is consistent with the higher baseline frequencies for such comorbidities in the AS cohort. Unlike several previous studies,10 ,11 ,33 we did not find any increase in deaths assigned to suicides in the AS cohort, but in concordance to these studies spinal trauma as intermediate cause of death was more common in the AS cohort.
The present study has several strengths. First, it is a nationwide study, and the largest to our knowledge, assessing all-cause mortality in AS using an unexposed comparator from the general population, thus avoiding less precise estimates using SMRs.34 The large size of our study also enabled more precise mortality estimates for women with AS. Second, by using independent national data sources we were able to reliably assess predictors of mortality in the AS population and to have virtually complete ascertainment regarding mortality and residency, which minimises possible selection bias due to loss of follow-up.
One potential limitation of this study is misclassification of exposure or outcome. The definition used for identification of the AS cohort has been previously shown to have high validity, with positive-predictive values for fulfilling the modified New York criteria and the Assessment of SpondyloArthritis International Society (ASAS) classification criteria for axial SpA of 80% and 86%, respectively.35 In addition, HRs remained significantly increased when assuming a wide range of mortality rates in 20% of the AS cohort. The Cause of Death Register is likely to introduce some misclassification with regard to cause of death,36 although this is likely to be non-differential between the two cohorts and thus unlikely to have significantly flawed our results.
Selection bias, due to the fact that patients with AS exclusively seen in primary or private care were not captured by our study, could be a limitation. According to a previous study from southern Sweden, only 3% of patients with AS are being followed exclusively in primary care.18 The proportion of AS cases seeking private healthcare is estimated to be 15%.37 Our own estimates from the biologics register show that only 4.6% of those receiving TNFi are treated exclusively by private practitioners (data not shown). Therefore, underascertainment of AS should be less than 10%, and unlikely to bias our results.
Another limitation is that our analyses are based on a prevalent AS cohort. According to previous estimations there is a time lag of 10–15 years between disease onset and diagnosis registration for AS in the NPR, which is compatible with our finding of a mean age of 42.2 years at first diagnosis by a rheumatology specialist.35 This may have also led to exclusion of mild, self-limited AS cases lost to follow-up or very severe AS cases with premature death.
Finally, the nationwide registers used herein offered limited access to important clinical (eg, disease activity measures, physical function, acute phase reactants) and lifestyle variables (eg, smoking) and thus precluded the assessment of their role on mortality in AS.
Conclusion
In conclusion, in the present study we found increased mortality in patients with AS compared with the general population for both sexes. Within the AS cohort, lower socioeconomic status, general comorbidities and hip replacement surgery were identified as predictors of death. Further studies are thus warranted to disentangle the effects of disease severity, comorbidities and medication on mortality risk.
REFERENCES
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Handling editor Johannes Bijlsma
Contributors SE, CT, LEK, LTHJ: designed the study; SE: performed the data analysis, wrote the manuscript, participated in the interpretation of the results and submitted the manuscript; EL, UL, JA, HF-dE, CT, LEK, LTHJ: participated in the interpretation of the results and the drafting of manuscript; All authors had full access to all data at all points of the manuscript planning, drafting and post submission and all authors have read and approved the final version of the manuscript.
Funding The study was funded by the Oak foundation, the Swedish Rheumatism Association and the Lund University.
Competing interests None declared.
Ethics approval Regional Ethics Committee, Karolinska Institute, Stockholm, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.