Article Text

Abstract
Objectives Around 1% of the population test positive for anti-cyclic citrullinated peptide (anti-CCP) antibodies. This biomarker predicts the progression to rheumatoid arthritis (RA) but over a variable time frame. To increase its clinical relevance, this study sought to determine (1) if the proportion of anti-CCP-positive individuals could be enriched by case selection of people attending primary care with new non-specific musculoskeletal (MSK) symptoms but without clinical synovitis (CS) and (2) whether these individuals progress rapidly to inflammatory arthritis (IA), in particular RA.
Methods In this prospective cohort study, individuals aged ≥18 years with new non-specific MSK symptoms, without CS, were recruited from primary care in the UK. Anti-CCP-positive individuals were invited for follow-up in the rheumatology department, Leeds. Those who tested negative were sent questionnaires 12 months later.
Results 2028 individuals were recruited. Of these, 2.8% (57/2028) were anti-CCP positive, of whom 47% (27/57) developed IA – 24 RA, 1 undifferentiated IA (UIA), 2 polymyositis; 92.6% (25/27) within 12 months, median 1.8 months (IQR 1.0–4.3, range 0.3–16.1). Of the anti-CCP-negative individuals, 1.3% (20/1559) developed IA (1 UIA, 13 RA, 6 psoriatic arthritis); 75% (15/20) within 12 months. The relative risk for developing RA within 12 months in the anti-CCP-positive group was 66.8 (95% CI 32.2 to 138.4, p<0.001); for IA, it was 45.5 (95% CI 25.4 to 81.6, p<0.001).
Conclusions Selecting individuals with new non-specific MSK symptoms without CS enriched the prevalence of anti-CCP positivity to 2.8%. Those who tested positive had a high risk of rapidly developing RA. The cost-effectiveness of this approach will need to be determined.
Trial registration number NCT02012764.
- Ant-CCP
- Rheumatoid Arthritis
- Early Rheumatoid Arthritis
- Autoantibodies
Statistics from Altmetric.com
From cross-sectional studies, anti-cyclic citrullinated peptide antibodies (anti-CCP) are present in approximately 1% of the population.1 ,2 Their presence has been associated with a high risk of subsequent development of rheumatoid arthritis (RA).3 ,4 Anti-CCP antibodies, however, can be detected more than 10 years prior to disease onset.5 The risk of progression to RA in anti-CCP-positive individuals from the general population has been estimated at 5% over a 5-year period,1 meaning that this test is unlikely to be of value as a screening tool. In the years just prior to diagnosis, however, retrospective studies have found the predictive value of CCP testing to be much higher, with a positive predictive value (ppv) of 85% noted within 1.5 years of symptom onset.5
It is also recognised that people with RA often have musculoskeletal (MSK) complaints which may not be sufficiently suggestive of an inflammatory arthritis (IA) (from herein referred to as ‘non-specific symptoms’) in the months or years prior to development of RA. Joint pain, muscle cramps, stiffness, loss of motor control and weakness are described as the first symptoms in people with RA and anti-CCP-positive arthralgia.6 The majority of people present to their general practitioners (GPs) first. It has been estimated that people with RA visited their GPs on average four times before being referred to a specialist for a diagnosis.7 Identifying individuals with new non-specific symptoms with the anti-CCP antibody may therefore provide an enriched case selection for imminent RA.
In 2009, the National Audit Office estimated the prevalence of RA in adults in England at 580 000 with an incidence of 26 000 new cases per year.7 The estimated cost of RA to the UK National Health Service was approximately £560 million a year and the cost of work-related disability and sick leave was estimated at £1.8 billion a year. Delays in treatment have been associated with increased joint damage and poorer function.8 ,9 In contrast, early identification has been associated with improved clinical outcomes, health-related quality of life and work ability.10 Thus, very early identification and targeted treatment of individuals at risk of imminent RA11 has the potential to be cost-effective.
In this study, we aimed to show that individuals present with new-onset, non-specific MSK complaints in the preclinical phase of RA, and that these individuals can be identified by performing an anti-CCP antibody test. This should identify anti-CCP-positive individuals at risk of rapid progression to RA who would otherwise not be referred, allowing assessment of individuals at risk of IA at the earliest opportunity.
The primary hypothesis was that a higher proportion of individuals with new-onset, non-specific MSK symptoms have anti-CCP antibodies compared with the general population. The secondary hypothesis was that the presence of the anti-CCP antibody in individuals with non-specific MSK symptoms would help to identify those at risk of rapid progression to RA.
Methods
This was a longitudinal prospective cohort study adopted by the National Institute of Health Research Clinical Research Network (NIHR CRN).12 It was initially conducted in West, North and North East Yorkshire and later opened to recruitment across the UK. Individuals were recruited between July 2007 and March 2015. GPs, MSK physicians, physiotherapists, nurse practitioners and other health professionals were asked to refer individuals aged ≥18 years with any new MSK complaint, whom they were not already planning to refer to a rheumatology unit with an IA, for an anti-CCP test. For the purpose of this study, a new MSK complaint was defined as any joint/MSK symptom, including (but not limited to) rotator cuff tendonitis, subacromial bursitis, carpal tunnel syndrome, tendonitis, for example, epicondylitis, which the patient had not previously reported to their GP. Individuals with documented IA were excluded.
Individuals consenting to study participation were instructed to go to their GPs/local phlebotomy centres to give a blood sample. The serum was sent to Chapel Allerton Hospital, Leeds, for the anti-CCP antibody tests to be performed. This was done using second-generation CCP assays. Anti-CCP positivity was determined using machine-specific cut-offs—initially using an ImmunoCAP 250 (Phadia) (reference range <7 U/mL) and later a BioPlex 2200 (Bio-Rad) machine (reference range <2.99 U/mL). They were also asked to complete a questionnaire and provide information on previous or current MSK diagnoses and mark their symptoms on a diagram. The questionnaire was updated during the course of the study to request details for information on family history of RA and smoking.
Individuals with positive anti-CCP antibody test results were contacted by the rheumatology department and offered an outpatient appointment at the CCP clinic at Chapel Allerton Hospital for clinical assessments, blood tests and imaging with X-rays and other modalities. Individuals with negative anti-CCP tests continued to be followed up with their GPs. They were also contacted via telephone/post 12 months after consenting to the study and sent a questionnaire. Follow-up was therefore either after a period of 12 months or until the development of clinical synovitis (CS). If necessary, GPs and rheumatology departments were also contacted for relevant diagnoses.
Outcomes
The primary outcome was the proportion of individuals with new-onset, non-specific MSK symptoms who were anti-CCP positive. Secondary outcomes included the number of anti-CCP-positive individuals who progressed to IA, in particular RA (according to the 2010 American College of Rheumatology (ACR) / European League Against Rheumatism (EULAR) RA Classification Criteria13), and the time to IA diagnosis. Other outcomes of interest included the initial presenting complaint of all individuals (anti-CCP positive and anti-CCP negative), as this may help to determine whether there is a symptom complex that would prompt autoantibody testing.
Statistical analysis
Statistical analyses were performed using SPSS V.21 and StataIC V.13. For the analyses, the date of the anti-CCP test was used as the baseline date. Demographic characteristics, the prevalence of anti-CCP positivity, the progression to IA and the associations with joint involvement were calculated using Pearson's χ2 tests. A one-sample binomial test was used to assess whether the proportion of individuals with anti-CCP antibodies was higher among those presenting with new MSK pain compared with the estimated proportion in the general population (1%). The median time to IA development was compared using a log-rank test. The sensitivity and specificity for the anti-CCP antibody test were calculated together with the 95% CIs (Wilson method). Binary logistic regression was used to assess the association between the involvement of specific joint types and the risk of being anti-CCP positive.
Results
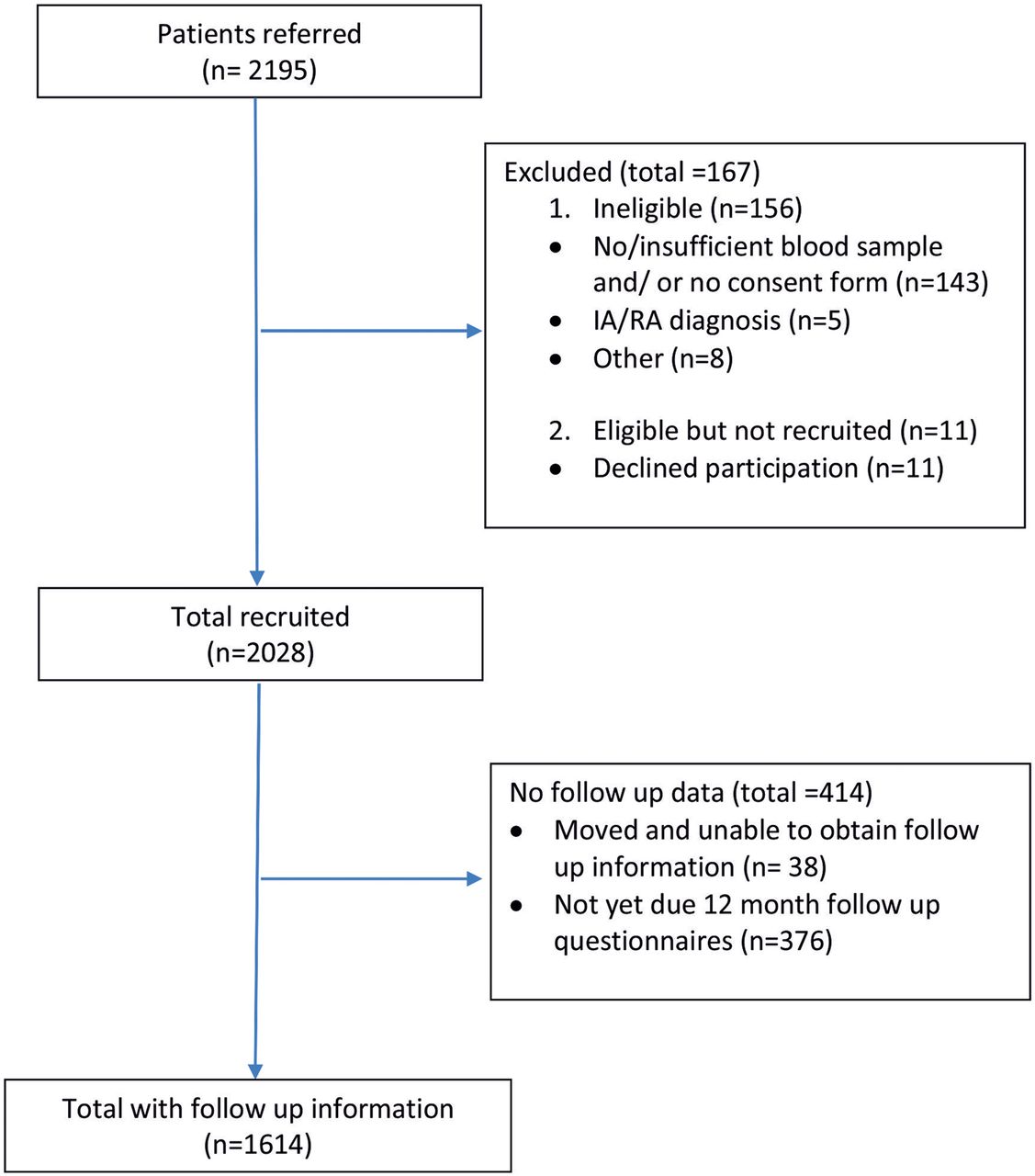
In total, 2195 individuals were referred, of whom 2028 individuals with new non-specific MSK symptoms were enrolled (figure 1). The mean age was 49.2 (13.6) years and the majority were women (75.9%). Of these, 2.8% (57/2028) were anti-CCP positive, a significantly higher proportion than the estimated 1% for the general population (95% CI 2.1% to 3.6%, p<0.001). There were no differences in demographic features between anti-CCP-positive and anti-CCP-negative individuals. Individuals had a range of MSK and associated conditions with no significant differences between those who were anti-CCP positive or anti-CCP negative (table 1).
Baseline characteristics of individuals with new non-specific MSK symptoms

Study recruitment. IA, inflammatory arthritis; RA, rheumatoid arthritis.
Of those who were antibody positive, 47.4% (27/57) were subsequently diagnosed with an IA—1 with undifferentiated IA (UIA), 24 with RA and 2 with polymyositis. Of those who were tested anti-CCP negative and completed at least 1 year of follow-up, 1.3% (20/1559) were diagnosed with an IA—1 with UIA, 13 with RA and 6 with psoriatic arthritis (PsA). The relative risk (RR) for ever-developing IA in the anti-CCP-positive group was 36.8 (95% CI 22.0 to 61.7, p<0.001) and the RR for developing RA was 50.4 (95% CI 27.1 to 93.8, p<0.001) (table 2). The sensitivity and specificity for the development of any IA in the anti-CCP-positive individuals were 57.4% (43.3% to 70.5%) and 98.1% (97.3% to 98.7%), respectively, and the ppv and negative predictive value (npv) were 47.4% (35.0% to 60.1%) and 98.7% (98.0% to 99.2%), respectively. The sensitivity, specificity, ppv and npv for the progression to RA were 64.9% (48.8% to 78.2%), 97.9% (97.1% to 98.5%), 42.1% (30.2% to 55.0%) and 99.2% (98.6% to 99.5%), respectively.
Outcomes of anti-CCP-positive and anti-CCP-negative individuals with new non-specific MSK symptoms
The median duration of follow-up of anti-CCP-positive individuals with MSK symptoms (to IA diagnosis or last assessment) was 11.5 months (IQR 1.5–28.2; range: 0.3–79.1 months). The median time for the progression to IA in the 25 anti-CCP-positive individuals was 1.8 months (95% CI 1.2 to 2.3, IQR 1.0–4.3, range 0.3–16.1 months). The majority (25/27 (92.6%)) were diagnosed within 12 months of the anti-CCP test. In the anti-CCP-negative individuals, the median time to IA diagnosis or last follow-up was 13.8 months (IQR: 12.5–21.5, range 1.2–84.4 months) and the median time to IA diagnosis was 5.1 months (95% CI 4.2 to 5.8; IQR 2.9–13.5, range 1.2–27.2 months, p=0.002 for anti-CCP positive vs anti-CCP negative); 75% (15/20) were diagnosed within 1 year of having the test. The RR for developing IA within 12 months in the anti-CCP-positive group was 45.5 (25.4 to 81.6), p<0.001 and the RR for developing RA within 12 months was 66.8 (32.2 to 138.4), p<0.001 (figure 2).

{kind=link}
{kind=link}
Kaplan–Meier graph: Time to RA progression in individuals with new non-specific MSK symptoms. Anti-CCP, anti-cyclic citrullinated peptide antibody; RA, rheumatoid arthritis; MSK, musculoskeletal symptoms.
Analyses of location of symptoms showed that individuals with pain affecting the regions of the wrists and/or hands or the feet were more likely to be anti-CCP positive (RR 2.9 (1.2 to 7.3, p=0.024) for wrists and/or hands and RR 2.1 (1.2 to 3.6, p=0.008) for feet). Those with shoulder symptoms were also more likely to have a positive anti-CCP result (RR 2.1 (1.2 to 3.7, p=0.010)) (table 3). The association between the location of symptoms and the progression to RA was not analysed as the number of patients per variable would be too small.14 ,15
Associations between joint symptoms and anti-CCP positivity in individuals with new non-specific MSK symptoms
Discussion
To our knowledge, this is the first prospective cohort study addressing the prevalence of anti-CCP in individuals with new non-specific MSK symptoms without CS and the progression to IA. In this cohort of individuals referred from primary care, 2.8% were anti-CCP antibody positive with 45% progressing to IA mainly RA, the majority within 1 year of antibody testing.
Several retrospective studies have identified the presence of RA-associated autoantibodies in individuals with RA prior to disease onset with a rise in prevalence in the years just prior to diagnosis.1 ,5 In a large population study, the prevalence of RA was found to be 19% in rheumatoid factor (RF)-positive individuals.16 The finding from the Nurses’ Health Study showed a sensitivity and specificity of 28% and 100%, respectively, in a single pre-RA diagnosis serum sample tested for anti-CCP antibodies. Higher antibody levels were associated with a shorter time to diagnosis.17 In another cohort, 20% (29/147) developed IA, of whom 50 were CCP positive, 52 RF positive and 45 positive for both antibodies, 45% developed RA after a median of 28 months. The presence of anti-citrullinated protein antibodies (ACPA), but not RF or shared epitope, was associated with disease progression.18
In recent years, there has been increasing focus on work addressing individuals at risk of developing RA.19 Other methods have also been evaluated for identifying these individuals early. Liang et al20 have explored the possibility of an internet-based method for identifying people with symptoms of an inflammatory polyarthritis of less than 12 weeks. In this study, 43 244 people took the on-line questionnaire. Of these, 60 took a self-scoring algorithm for IA, 48 screened positive, 24 were evaluated and 3 were diagnosed with IA. Of the 24 people, 17 completed a follow-up questionnaire at 1 year—3 were diagnosed with RA and were on methotrexate.
An important question that would need careful consideration prior to implementing any case-finding strategy is that of cost-effectiveness. On the one hand, there is the cost of the disease, which is associated with irreversible joint damage and increased morbidity, the cost of treatment and societal costs, including potential job loss.7 This needs to be balanced against the cost of performing investigations in order to find early treatable RA and prevent disease progression.
Testing of individuals with non-specific symptoms for anti-CCP provides a relatively easy and simple method for identifying individuals at risk at an early stage. Another possibility would be to refine the group to be tested and referred. Hand involvement has been reported to be more common in individuals who progress to RA.6 In our cohort, symptoms involving the wrists and/or hands, the feet and the shoulders were associated with anti-CCP positivity. A history of early morning stiffness (EMS), the presence of polyarticular pain, RF or inflammatory markers has been reported to increase the ppv of anti-CCP in individuals with early RA.21 In another cohort of ACPA-positive individuals with symmetric arthralgia of small joints and EMS, 60% progress to RA.18 The presence of anti-CCP together with inflammatory symptoms, the presence of shared epitope and imaging with ultrasound have also been shown to enable identification of individuals with RA at an early stage.11
While the majority of anti-CCP-positive individuals who progressed to IA in this cohort were classified as RA, two individuals were later diagnosed with Jo-1 polymyositis, one with high-level anti-CCP antibodies and the other with a borderline result. Studies suggest that the autoimmune process in ACPA-associated diseases may begin at mucosal sites, for example, the lung.22 These two individuals may have an overlap of RA and polymyositis. The possibility of a pathogenic link between polymyositis and ACPA with lung involvement in both, however, is an interesting one.
The study has its limitations. These findings have been compared with an estimated 1% based on blood donor cohorts.1 ,2 While this may be a reasonable approximation of anti-CCP positivity in the general population, it is known that screening of donors excludes individuals with medical conditions and may therefore underestimate the population prevalence of the antibody. Despite this, the findings from this study suggest that individuals with rapid progression to RA may be identified. Another limitation is that participants in this study have mainly been recruited from Yorkshire, UK. The antibody prevalence may differ in other populations and ethnic groups. Of the individuals who progressed to RA, approximately one-third were anti-CCP negative. While anti-CCP positivity has been associated with more severe destructive disease, the study confirms the need for additional biomarkers for the diagnosis of seronegative RA and other inflammatory arthritis, for example, PsA. The joint symptoms and associated conditions were all self-reported from patient questionnaires. It is possible that there may be a bias towards under-reporting as patients may have only reported what they may have perceived as relevant to this study.
In conclusion, in our study selecting individuals with new non-specific MSK symptoms without CS enriched the prevalence of anti-CCP positivity to 2.8%, with anti-CCP-positive individuals being found to be at high risk of rapidly developing an IA, in particular RA. The cost-effectiveness of this approach will need to be determined.
Acknowledgments
The authors would like to thank all the participating GPs and health professionals for their referrals to the study and the UKCRN teams for their support in primary care. The authors would also like to acknowledge Dr Sally Cox for help with study set up; Chris Brooks, Mark Harrison, Hazel Rowson and Christine Thomas for administrative support, and Dianne Corscadden, Karen Henshaw and Katie Barnes for laboratory support.
References
Footnotes
Handling editor Tore K Kvien
Contributors PE was responsible for the study design and overseeing the study. JLN was responsible for study recruitment, data collection, data analysis and writing of the manuscript. LH assisted with recruitment and EMAH with the data analysis. All coauthors contributed to revising the manuscript.
Funding This study presents independent research supported by the National Institute for Health Research (NIHR). This study was supported by AbbVie who provided funding for the anti-CCP testing.
Disclaimer The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests Paul Emery is an Arthritis Research UK Professor of Rheumatology.
Ethics approval Leeds West Research Ethics Committee (REC reference number 06/Q1205/169).
Provenance and peer review Not commissioned; externally peer reviewed.